Juvenile Idiopathic Scoliosis: Comprehensive Principles and Operative Management
Key Takeaway
Juvenile idiopathic scoliosis (JIS) presents in children aged 4 to 10 years and carries a significantly higher risk of curve progression compared to adolescent variants. Management requires a rigorous, evidence-based approach, transitioning from serial observation and orthotic bracing to advanced surgical interventions like dual growing rod constructs. This guide details the biomechanical principles, preoperative MRI indications, and step-by-step surgical techniques necessary to prevent the crankshaft phenomenon and optimize spinal growth.
Introduction and Natural History
Juvenile idiopathic scoliosis (JIS) is defined as a spinal deformity presenting in children between the ages of 4 and 10 years. While multiple curve patterns can manifest, the convexity of the thoracic curve is predominantly to the right, mirroring the typical presentation of adolescent idiopathic scoliosis (AIS). However, the natural history and prognostic trajectory of JIS are markedly distinct and generally considered to be far more aggressive and progressive than those of AIS.
The propensity for relentless curve progression in this demographic is well documented. Seminal research by Lonstein demonstrated that 67% of patients diagnosed before the age of 10 exhibited significant curve progression. More critically, the risk of progression escalates to an absolute 100% in patients younger than 10 years who present with initial curves exceeding 20 degrees. This aggressive natural history necessitates a highly vigilant, proactive approach to both clinical observation and therapeutic intervention.
Clinical Evaluation and Preoperative Workup
The clinical evaluation of a patient with juvenile idiopathic scoliosis must extend beyond the standard scoliometer measurements and radiographic assessments. A critical component of the diagnostic workup is the evaluation of the neural axis.
Maenza and colleagues identified a alarmingly high incidence of neural axis abnormalities in children younger than 11 years presenting with scoliosis. In their cohort, 26.7% of patients who met the indications for surgical intervention possessed underlying magnetic resonance imaging (MRI) abnormalities—such as syringomyelia, Chiari malformations, or tethered cord syndrome—despite being considered neurologically normal during standard preoperative clinical examinations.
Clinical Pearl: Routine MRI evaluation of the entire neuroaxis is strongly recommended as an indispensable component of the preoperative workup for any patient with juvenile idiopathic scoliosis.
While some debate persists regarding the absolute necessity of routine MRI in asymptomatic, mild cases, there is universal consensus among orthopedic spine surgeons that specific "red flag" clinical factors mandate immediate and comprehensive MRI evaluation. These factors include:
* Presence of significant back pain.
* Rapid, atypical curve progression.
* Left-sided thoracic deformity (which carries a higher association with syrinx).
* Neurological abnormalities, specifically alterations or absence of the superficial abdominal reflexes.
* Any evidence of bowel or bladder dysfunction.
* Foot deformities such as unilateral cavus foot.
Non-Operative Management: Observation and Orthotics
Despite its high likelihood of progression and eventual surgical requirement, the initial management of juvenile idiopathic scoliosis adheres to guidelines structurally similar to those utilized for adolescent idiopathic scoliosis, albeit with a lower threshold for intervention.
Observation Protocols
For coronal curves measuring less than 20 degrees, conservative observation is the indicated primary course of action. This involves rigorous clinical examination and standing posteroanterior (PA) and lateral full-spine radiographs at intervals of every 4 to 6 months.
Orthotic Intervention
Evidence of radiographic progression—defined as a documented change of at least 5 to 7 degrees between serial evaluations—warrants the immediate initiation of brace treatment. If the curve remains stable, observation is continued until the patient reaches skeletal maturity.
Historically, the Milwaukee brace (cervico-thoraco-lumbo-sacral orthosis or CTLSO) was the gold standard for orthotic treatment in juvenile idiopathic scoliosis, primarily because it avoids the compressive forces on the developing thoracic cage that can lead to restrictive pulmonary disease. However, a custom-molded Thoracolumbosacral Orthosis (TLSO) is now frequently utilized for thoracic curves where the apex is located at T8 or below.
Bracing Protocol:
1. Initial Phase: The orthosis is prescribed for full-time wear, strictly defined as 22 out of 24 hours per day.
2. Weaning Phase: If the curve demonstrates improvement or stabilization after a minimum of 1 year of full-time compliance, the daily wear time can be incrementally decreased. This often transitions to a nighttime-only bracing program, which significantly improves patient compliance and psychosocial tolerance, particularly as the child approaches the onset of puberty.
3. Surveillance: The patient must be meticulously monitored during the weaning process. Any radiographic sign of curve progression mandates an immediate return to the full-time bracing protocol.
The success rates of nonoperative management are highly variable. Literature from Figueiredo and James indicates that 44% of patients were successfully managed conservatively, while 56% ultimately required spinal fusion. Similarly, Tolo and Gillespie reported a 27% surgical fusion rate for progressive curves in their series.
The Rib-Vertebra Angle Difference (RVAD)
Predicting which curves will progress remains a clinical challenge. Tolo and Gillespie noted that initial curve pattern, degree of curvature, and age at diagnosis were insufficient predictors. However, the Rib-Vertebra Angle Difference (RVAD), originally described by Mehta, serves as a critical prognostic tool when measured serially.
Mannherz et al. confirmed that while the initial RVAD measurement might lack predictive power, a progressive increase in the RVAD to greater than 10 degrees over time is strongly associated with relentless curve progression. Furthermore, a higher incidence of progression is noted in patients presenting with less than 20 degrees of thoracic kyphosis (hypokyphosis) and those with double major curve patterns.
Evaluation of Brace Treatment of Juvenile Idiopathic Scoliosis by the RVAD:
* If the RVAD progresses above 10 degrees during brace wear, curve progression is highly expected.
* If the RVAD values decline as treatment continues, transitioning to part-time Milwaukee brace wear is generally adequate.
* Curves presenting with RVAD values near or below 0 degrees at the time of diagnosis typically require only a short duration of full-time brace wear before part-time wear can be safely initiated.
Kahanovitz, Levine, and Lardone demonstrated that patients with curves less than 35 degrees and RVADs less than 20 degrees exhibited excellent prognoses with a part-time Milwaukee brace program. Conversely, patients with curvatures exceeding 45 degrees at the onset of bracing, coupled with RVADs greater than 20 degrees, universally failed conservative management and required spinal fusion.
Biomechanics of Spinal Growth and the Crankshaft Phenomenon
Understanding the biomechanics of pediatric spinal growth is paramount when planning surgical interventions in the juvenile population. Dimeglio's foundational studies on spinal growth velocity provide the critical framework for this understanding.
During the first 5 years of life, the spine from T1 to S1 grows at a rapid rate of more than 2 cm per year. Between the ages of 5 and 10 years, this velocity decelerates to approximately 0.9 cm per year, before accelerating again to 1.8 cm per year during the adolescent pubertal growth spurt.
The Crankshaft Phenomenon
A profound complication unique to early-onset and juvenile scoliosis surgery is the "crankshaft phenomenon." In a landmark study of 24 children with infantile or juvenile idiopathic scoliosis, Hefti and McMaster demonstrated that achieving a solid posterior spinal fusion effectively arrests the longitudinal growth of the posterior elements. However, the neurocentral synchondrosis and the anterior vertebral body physes remain open and continue to grow anteriorly.
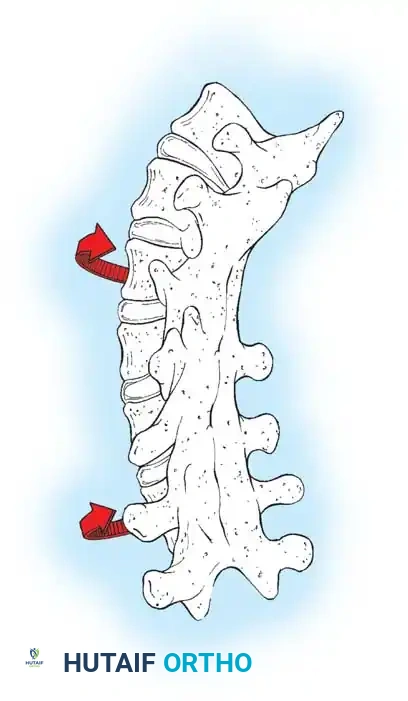
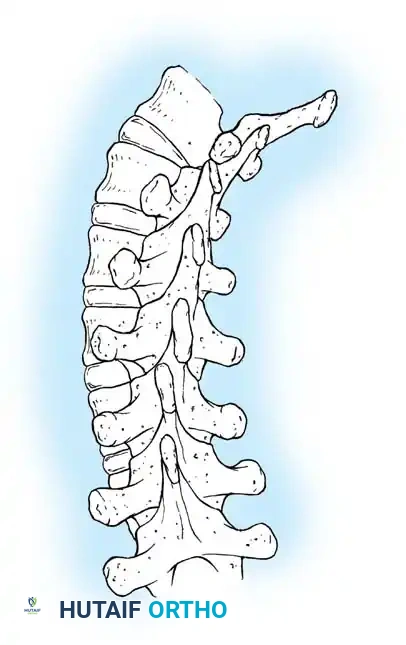
This continued anterior growth against a fixed posterior tether forces the vertebral bodies and intervertebral discs to bulge laterally toward the convexity of the curve. The spine essentially pivots on the solid posterior fusion mass, resulting in a severe loss of coronal correction, a dramatic increase in apical vertebral rotation, and the clinical recurrence of the rib hump deformity. Dubousset, Herring, and Shufflebarger have extensively documented and confirmed the biomechanics of this crankshaft phenomenon.
Surgical Indications and Decision Making
When orthotic treatment fails to halt progression, surgical intervention becomes mandatory. The choice of procedure is heavily dictated by the patient's age, remaining growth potential, and the size of the deformity.
- Children Younger Than 8 Years: The ideal treatment is the insertion of a growth-friendly construct, such as a subcutaneous dual growing rod system, with or without a localized anterior apical growth arrest procedure.
- Children Aged 9 to 10 Years: Definitive spinal fusion may be appropriate. However, to prevent the crankshaft phenomenon, a combined anterior and posterior spinal fusion must be strongly considered.
Surgical Warning: If a child is 9 or 10 years old, premenarchal, possesses a Risser sign of 0, and the iliac crest apophysis has not yet appeared, they retain massive anterior growth potential. A posterior-only fusion in this demographic carries an unacceptably high risk of postoperative crankshaft deformity.



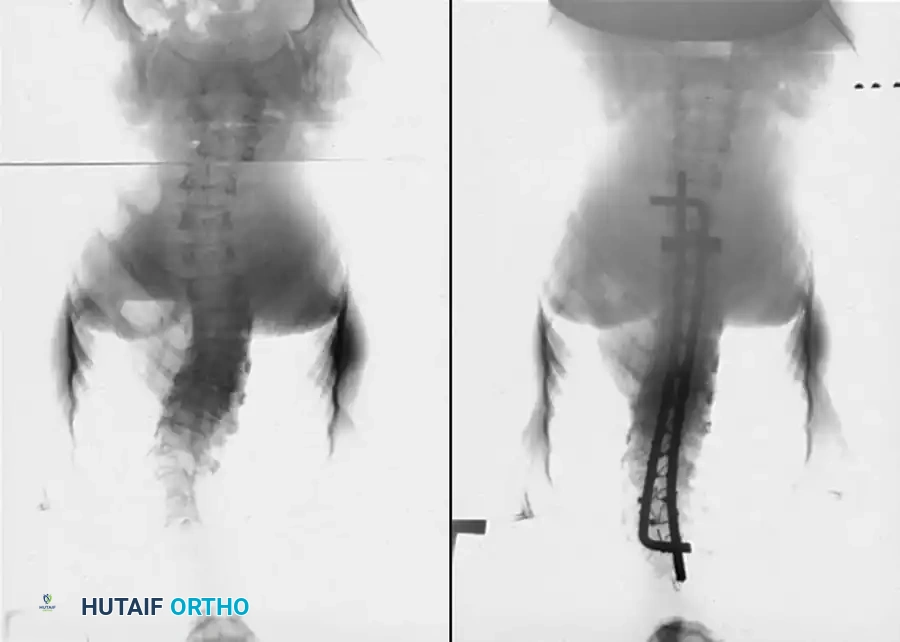
The sequence above illustrates a 57-degree curve corrected to 39 degrees with posterior fusion and instrumentation. Three years postoperatively, the deformity has severely recurred due to the crankshaft phenomenon.
To mitigate this, Shufflebarger and Clarke recommend that patients with a Risser sign of 0 or 1, a Tanner grade of less than 2, and a significant three-dimensional deformity undergo a preliminary anterior periapical release and fusion prior to posterior instrumentation. Sanders, Herring, and Browne further suggest that an open triradiate physis in the pelvis is a definitive indicator for supplementary anterior fusion. While modern pedicle screw instrumentation offers superior three-dimensional rotational control and may lessen the absolute need for anterior fusion in borderline cases, the risk must be carefully weighed.
Operative Management: Dual Growing Rod Instrumentation
Historically, Moe et al. described the use of a single subcutaneous Harrington rod without fusion, supplemented by full-time external bracing. While this allowed an average length gain of 3.8 cm, it was plagued by a 50% complication rate, primarily hook dislocation and rod fracture.
Modern surgical management relies on the Dual Growing Rod technique. Thompson et al. and Akbarnia et al. have demonstrated that dual growing rods are highly effective in controlling severe spinal deformities while safely permitting continued spinal growth. The dual-rod construct provides superior biomechanical stability, eliminating the need for an apical fusion during the treatment course and significantly reducing the incidence of implant failure compared to single-rod techniques.
Preoperative Planning and System Selection
A multihook or hybrid pedicle screw/hook segmental instrumentation system, such as the CD Horizon Legacy system (Medtronic Sofamor Danek), is utilized. For children weighing less than 30 lbs, an infant spinal set with smaller diameter rods (e.g., 3.5 mm or 4.0 mm) is necessary. Because these smaller rods are inherently more flexible, supplementary postoperative external immobilization (TLSO) is required until the child grows sufficiently to accommodate a larger pediatric rod system.
🔪 Surgical Technique: Dual Growing Rod Insertion
1. Positioning and Exposure:
* Place the patient prone on a specialized pediatric Jackson frame or radiolucent operating table, ensuring all bony prominences are meticulously padded.
* Prepare and drape the entire spine in a standard sterile fashion.
* Utilize preoperative and intraoperative fluoroscopy to precisely identify the neutral vertebrae at both the cranial and caudal ends of the curve.
* Make a single, long, straight midline incision extending from the upper to the lower planned foundation vertebrae.
* Carry the dissection down through the subcutaneous tissue and fascia to the spinous processes of the end vertebrae only.
2. Foundation Construction:
* CRITICAL STEP: Strip the periosteum from the lamina and transverse processes only at the specific upper and lower foundation sites. Do not perform any subperiosteal dissection between the hook/screw sites across the apex of the curve, as this will induce spontaneous autofusion and arrest spinal growth.
* Upper Foundation (Claw Construct): The upper anchors can utilize hooks or pedicle screws. If hooks are selected, create a stable "claw" by inserting a pedicle hook onto the lower of the two upper foundation vertebrae, and a superior transverse process hook on the upper of the two vertebrae. Perform this bilaterally on both the concave and convex sides.
* Lower Foundation: Form the lower claw by placing a supralaminar hook on the upper vertebra of the lower foundation and an infralaminar hook on the lower vertebra. Alternatively, if anatomically feasible and the pedicles are of sufficient diameter, bilateral pedicle screw fixation provides exceptional biomechanical pull-out strength for the lower foundation.
3. Rod Contouring and Insertion:
* Select two rods of appropriate diameter. Meticulously contour the rods to replicate the natural sagittal profile, incorporating appropriate thoracic kyphosis and lumbar lordosis.
* Insert the rods under direct vision into the upper and lower foundations.
* Secure the rods using the appropriate set screws within the hooks or pedicle screws.
* Join the proximal and distal rod segments centrally using low-profile extended tandem connectors. This allows for future distraction.
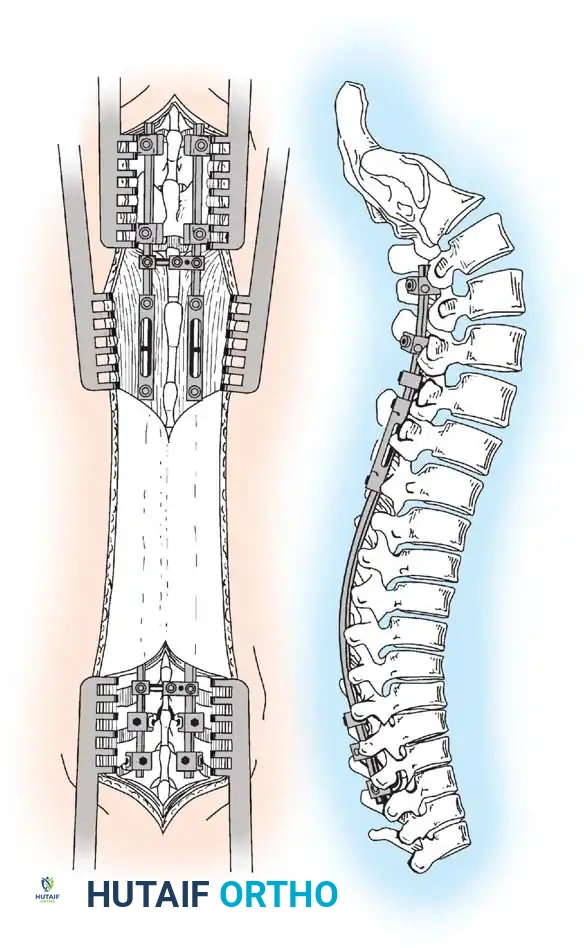
Technique of dual-rod instrumentation showing anteroposterior and lateral views. The construct is carefully contoured to maintain sagittal alignment, with extended tandem connectors placed in the thoracolumbar spine to minimize soft-tissue profile.
4. Local Arthrodesis and Closure:
* Decorticate the anatomy strictly within the upper and lower foundation sites.
* Pack locally harvested autograft or freeze-dried crushed cancellous allograft bone tightly around the upper and lower anchors to ensure a solid, localized arthrodesis at the foundation blocks.
* Irrigate copiously and close the wound in multiple anatomical layers to eliminate dead space and minimize the risk of postoperative seroma or infection.
Postoperative Protocol and Serial Lengthening
Immediate Postoperative Care:
The child is placed in a custom-molded TLSO orthosis for the first 6 months postoperatively. This protects the construct while the upper and lower foundation sites achieve solid bony fusion. Once radiographic evidence confirms foundation fusion, the orthosis can generally be discontinued.
Serial Lengthening Procedures:
The growing rods must be lengthened at regular intervals, typically every 6 months, to keep pace with the child's somatic growth.
* This is performed as a minor surgical procedure, often on an outpatient or short-stay basis.
* A small incision is made directly over the central tandem connectors.
* The set screws on the connectors are loosened.
* A specialized distraction instrument is applied to lengthen the rods, effectively distracting the spine and gaining length.
* The set screws are retightened, and the wound is closed.
Final Arthrodesis
Serial lengthenings are continued until the patient reaches skeletal maturity or until no further distraction can be safely achieved due to spontaneous autofusion or soft tissue tethering. At this juncture, the patient undergoes a definitive final arthrodesis.
The final procedure involves exposing the entire spine, removing the tandem connectors, and often removing the original rods. If the proximal and distal anchor foundations remain solidly fixed and well-fused, they are retained and incorporated into the final construct. A definitive multihook or pedicle screw segmental system (e.g., CD Horizon Legacy) is implanted.
To achieve the final fusion, meticulous facetectomies and widespread decortication are performed. We have observed excellent clinical success, particularly in younger children, utilizing freeze-dried crushed cancellous allograft bone supplemented with local bone, thereby achieving a robust, solid fusion while entirely avoiding the significant donor-site morbidity associated with harvesting autologous posterior iliac crest bone graft.
You Might Also Like