Congenital Scoliosis: Comprehensive Academic and Surgical Guide
Key Takeaway
Congenital scoliosis arises from embryological defects during the fifth to sixth week of gestation, leading to failures of vertebral formation or segmentation. Because 75% of these curves are progressive and rigid, early detection is paramount. Treatment relies heavily on surgical intervention, ranging from in situ fusion to complex hemivertebra excision, tailored to the patient's specific anatomical anomaly and remaining growth potential.
Introduction and Embryology
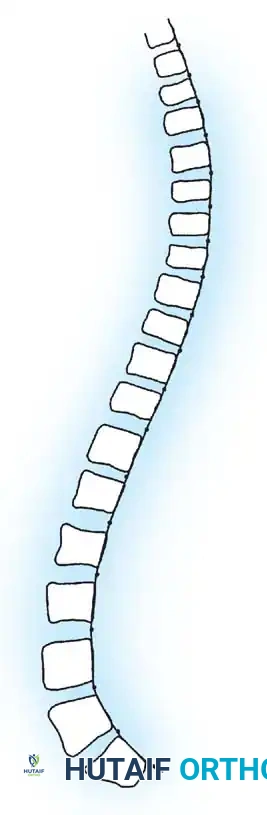
Congenital scoliosis is a structural lateral curvature of the spine resulting from anomalous vertebral development that creates a profound imbalance in the longitudinal growth of the spinal column. The critical embryological window for spinal development occurs between the fifth and sixth weeks of intrauterine life. During this period of somitogenesis and subsequent resegmentation, any disruption can lead to permanent congenital anomalies.
Because congenital scoliosis is inherently rigid and surgical correction of severe, neglected deformities is fraught with neurological risk, early detection is paramount. The overarching philosophy of management is to institute appropriate treatment while the curve is small, rather than attempting high-risk salvage procedures once severe deformity has established itself.
Extensive epidemiological studies, notably by Wynne-Davies, have found no definitive genetic etiology for isolated congenital abnormalities such as hemivertebrae. Furthermore, Winter’s comprehensive review of 1,250 family histories revealed only 13 patients with first- or second-degree relatives exhibiting congenital spinal deformities. Consequently, the prevailing consensus is that most congenital scoliosis arises from non-genetic, fetal environmental factors, though these specific teratogenic insults are rarely identifiable by patient history.
Classification of Congenital Scoliosis
The classification system proposed by MacEwen et al., and subsequently modified by Winter, Moe, and Eilers, remains the universally accepted standard. This system categorizes anomalies based on the specific embryological failure. Furthermore, curves must be classified by their anatomical region (cervicothoracic, thoracic, thoracolumbar, and lumbosacral), as regional biomechanics heavily dictate prognosis.
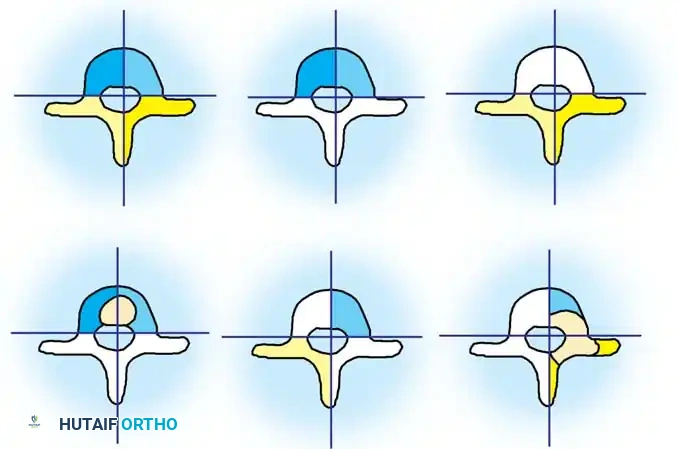
Failure of Formation
Failures of formation occur when a portion of the vertebra fails to develop.
* Partial Failure (Wedge Vertebra): A unilateral partial failure resulting in a wedged appearance.
* Complete Failure (Hemivertebra): A complete unilateral failure. Hemivertebrae can be further subdivided into:
* Incarcerated Hemivertebra: Tucked between adjacent normal vertebrae without causing significant deformity.
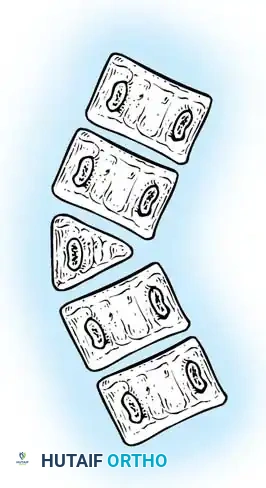
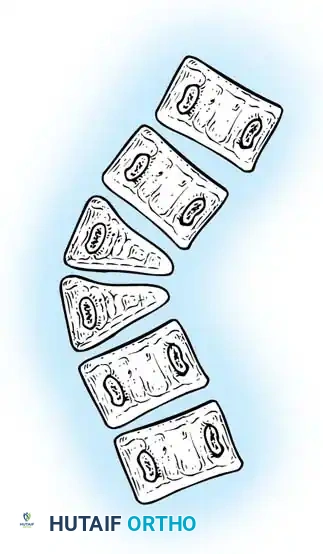
* Free/Segmented Hemivertebra: Separated from adjacent vertebrae by functional discs and physes, acting as an active wedge that drives progressive deformity.
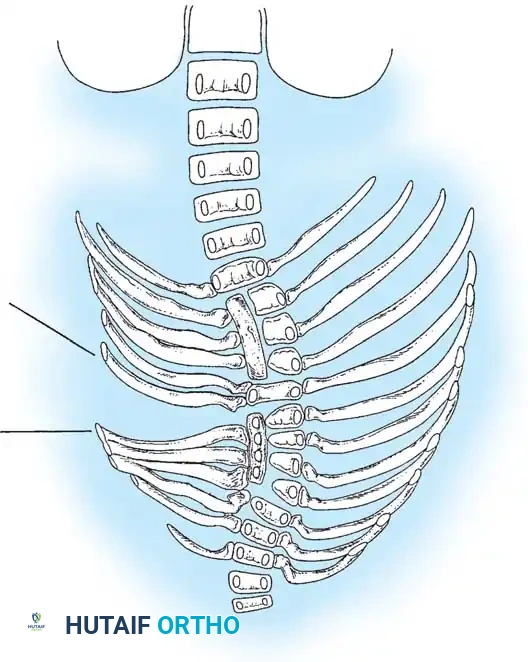
Fig. 38-120 Defects of formation. A, Anterior central defect. B, Incarcerated hemivertebra. C, Free hemivertebra. D, Wedge vertebra. E, Multiple hemivertebrae.
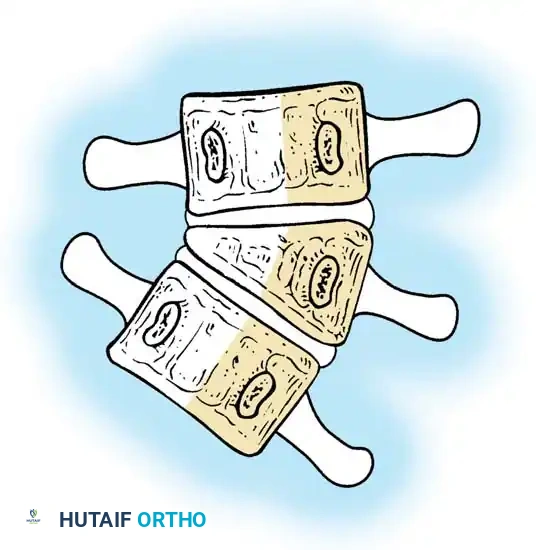
Failure of Segmentation
Failures of segmentation occur when the embryological somites fail to separate, creating a bony tether.
* Unilateral Failure (Unsegmented Bar): A solid bony bar on one side of the spine that completely tethers growth on that side, while the contralateral side continues to grow, leading to rapid and severe curvature.
* Bilateral Failure (Block Vertebra): Symmetrical failure of segmentation resulting in a fused block. This typically causes shortening rather than severe lateral curvature.
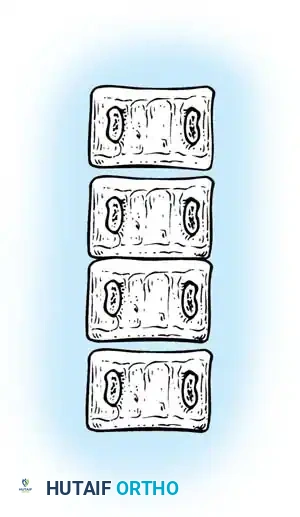
Fig. 38-121 Block vertebra.
Mixed and Miscellaneous Anomalies
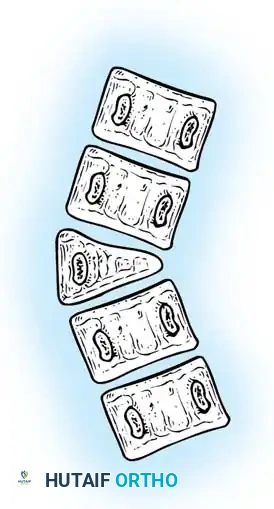
The most malignant of all congenital anomalies is a mixed deformity: a unilateral unsegmented bar with a contralateral hemivertebra at the same level. This creates a simultaneous tether on the concavity and an expansile force on the convexity.
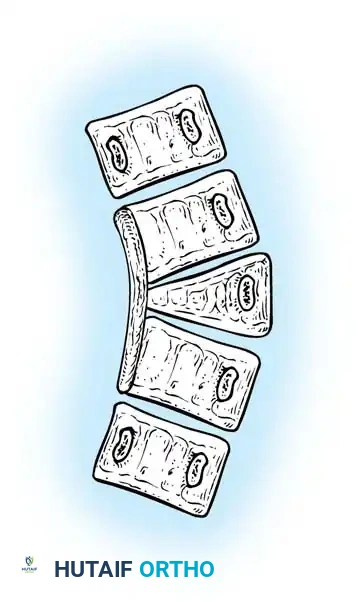
Fig. 38-125 Unilateral and unsegmented bar with contralateral hemivertebra.
Comprehensive Patient Evaluation
Clinical Examination
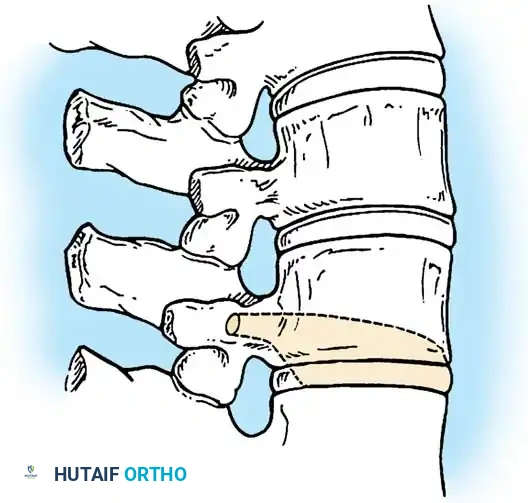
Patients presenting with congenital scoliosis require a meticulous physical examination extending beyond the spine. The skin of the back must be scrutinized for cutaneous stigmata of spinal dysraphism.
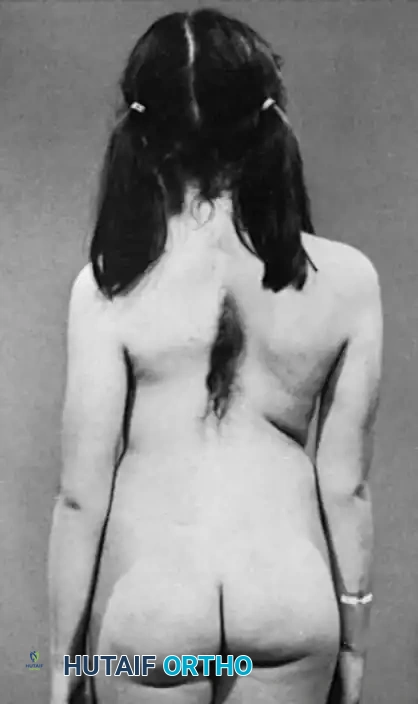
Fig. 38-122 Hair patch associated with diastematomyelia and congenital scoliosis.
A rigorous neurological evaluation is mandatory. Subtle signs such as asymmetric abdominal reflexes, calf atrophy, cavovarus foot deformity, or unilateral hyperreflexia may be the only clinical indicators of an underlying tethered cord or diastematomyelia.
Associated Systemic Anomalies (VACTERL)
Congenital scoliosis is frequently a manifestation of broader embryological insults.
* Genitourinary (GU) Anomalies: Present in up to 18% to 40% of patients. Drvaric et al. recommend routine screening ultrasound for all patients, as obstructive uropathy can be life-threatening.
* Cardiovascular Anomalies: Present in approximately 7% of patients.
* Intraspinal Anomalies: Diastematomyelia occurs in roughly 5% of patients, and overall spinal dysraphism is seen in 10%.
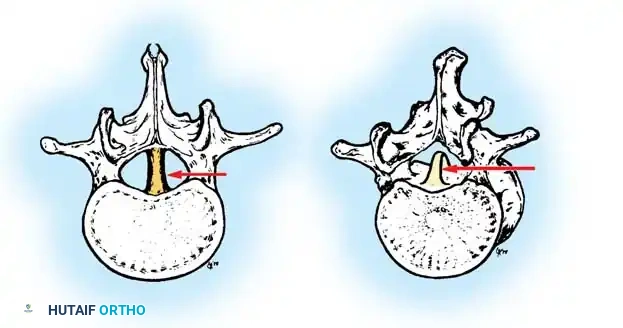
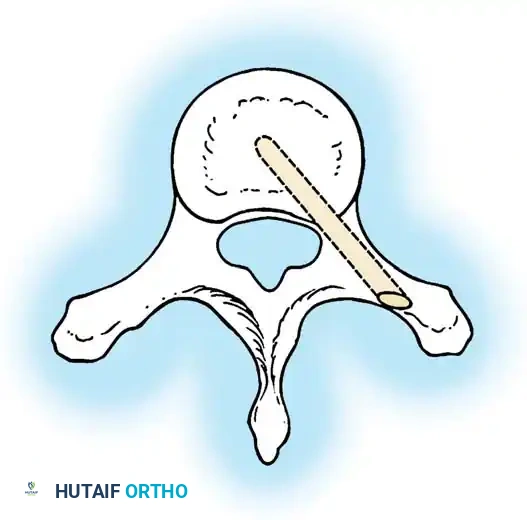
Fig. 38-123 Diastematomyelia spicule invaginating the dura and dividing the spinal cord.
Radiographic and Advanced Imaging
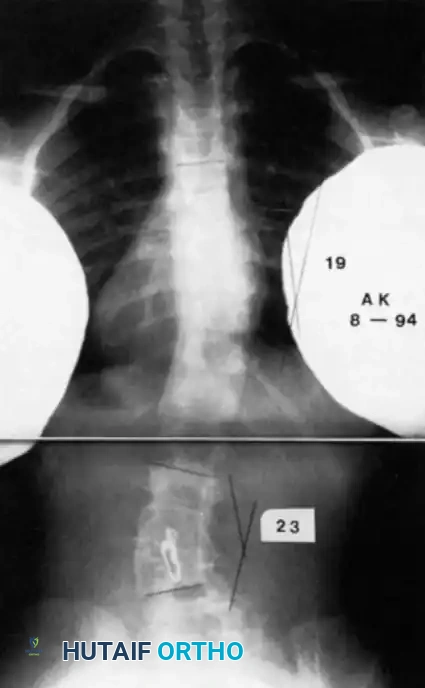
High-quality plain radiography is the cornerstone of diagnosis. Initial evaluation should include 40-inch supine films using slow-speed film to maximize bony detail before severe deformity obscures the anatomy.
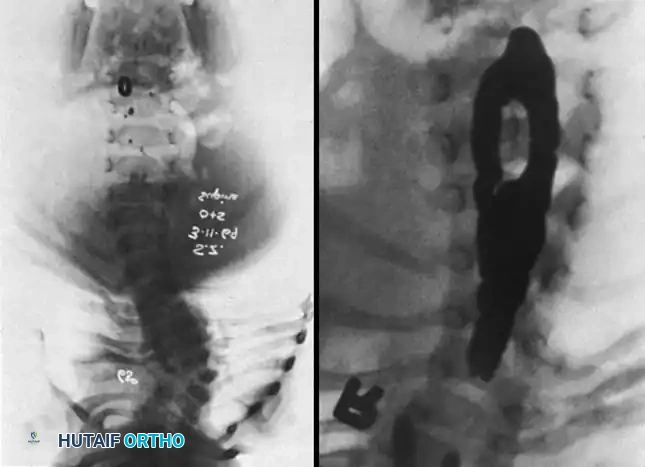
Fig. 38-124 A, Widening of spinal canal. B, Myelogram showing classic midline defect of diastematomyelia.
Clinical Pearl: Always evaluate the pedicles on the AP radiograph. Widening of the interpedicular distance is a strong indicator of an underlying intraspinal anomaly, necessitating immediate MRI evaluation.
MRI is essential for evaluating the neural axis, particularly in infants where cartilaginous anatomy is not yet ossified. It is critical to rule out tethered cord, syringomyelia, or diastematomyelia before any surgical correction of the spine is attempted, to prevent iatrogenic neurological injury.
Advanced imaging modalities are critical for preoperative planning and 3D anatomical understanding.
Natural History and Prognostication
Understanding the natural history is the most critical factor in surgical decision-making. McMaster and Ohtsuka’s landmark study of 216 untreated patients established the prognostic hierarchy of congenital anomalies.
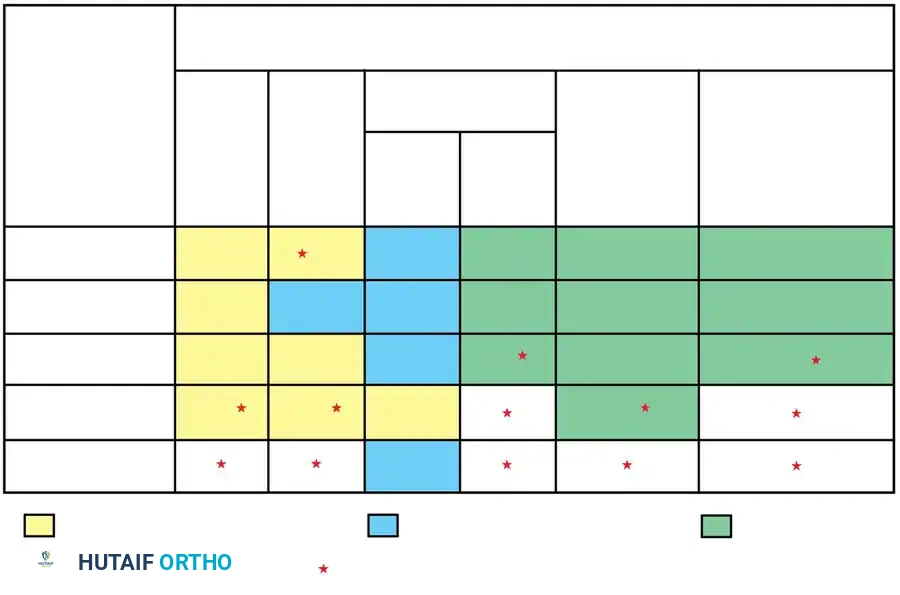
Fig. 38-126 Median yearly rate of deterioration without treatment.
Progression Risk by Anomaly Type (Highest to Lowest):
1. Unilateral unsegmented bar with contralateral hemivertebra.
2. Unilateral unsegmented bar.
3. Double convex hemivertebrae.
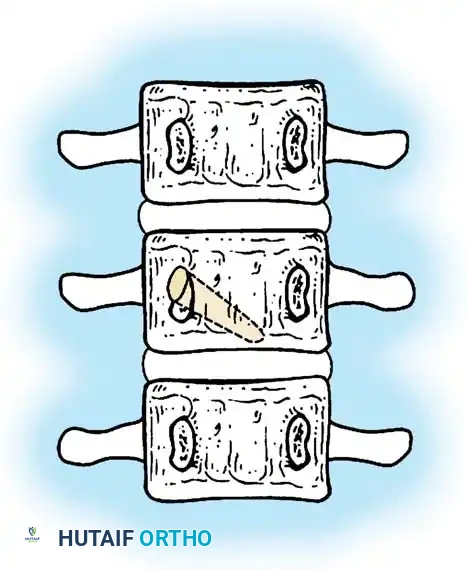
4. Single segmented hemivertebra.
5. Block vertebra (rarely progressive).

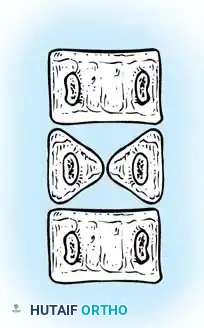
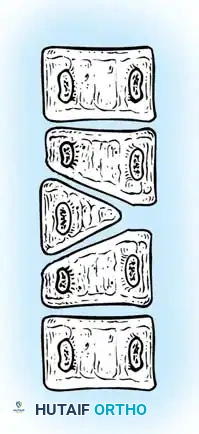
Fig. 38-127 Segmented hemivertebra with two functioning physes.
Progression Risk by Region:
Thoracolumbar anomalies carry the highest risk of progression due to the lack of stabilizing rib cage structures and the high biomechanical loads at the transition zone.
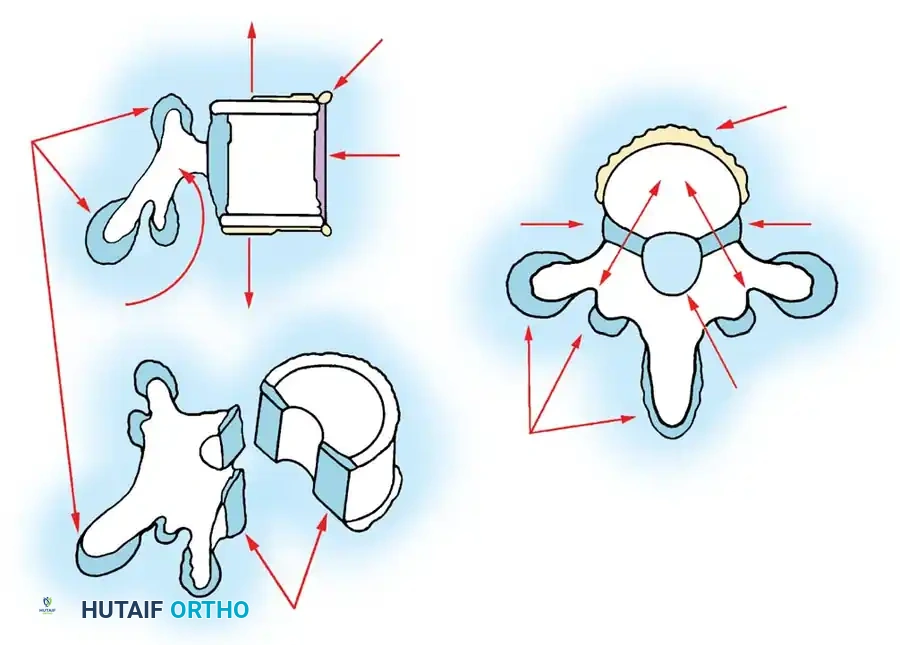
Fig. 38-128 Vertebral growth analysis is essential for predicting 3D deformity progression.
Nonoperative Management
Nonoperative treatment has a highly restricted role in congenital scoliosis. Because the deformity is structural and driven by asymmetric growth, orthoses cannot correct the primary anomaly.
Bracing (e.g., Milwaukee brace or TLSO) is effective in only 5% to 10% of cases. Its primary indication is the control of long, flexible compensatory curves that develop above or below the rigid congenital segment. Short, sharp, rigid congenital curves will not respond to bracing and attempting to brace them only delays inevitable surgery while allowing secondary structural changes to occur.
Operative Management: Principles and Techniques
Because 75% of congenital curves are progressive, surgery is the definitive treatment. The goal is to halt progression, achieve a balanced spine, and preserve as much longitudinal growth as possible.
1. Posterior Spinal Fusion Without Instrumentation (In Situ Fusion)
In situ fusion is indicated for young children with progressive curves that are currently of acceptable magnitude. The goal is to create a solid arthrodesis across the anomalous segments to prevent further deterioration.
Surgical Steps:
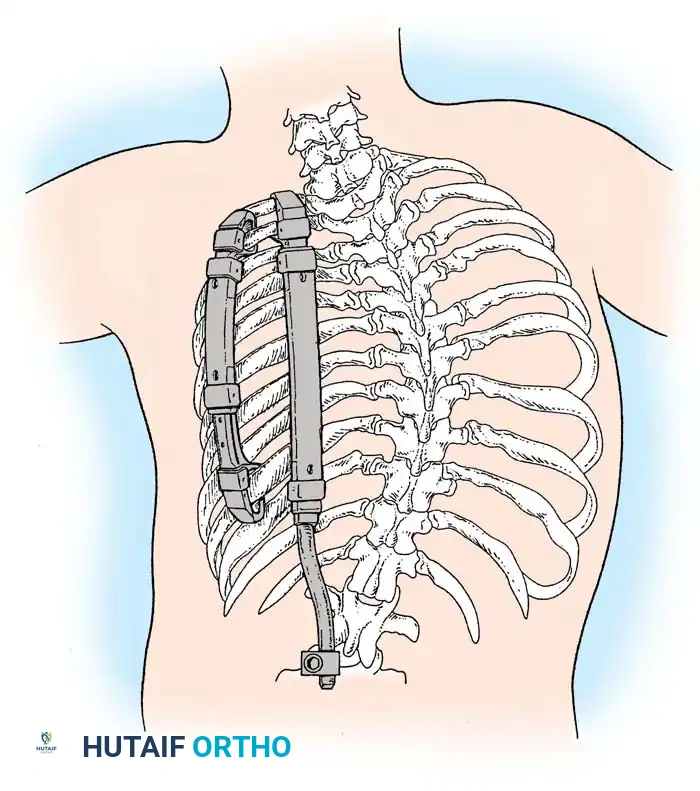
1. Positioning: Prone on a radiolucent frame, ensuring the abdomen is free to reduce venous pressure.
2. Exposure: Subperiosteal dissection is performed meticulously. In congenital spines, the anatomy is distorted; laminae may be absent, and the dura may be exposed subcutaneously (spina bifida occulta).
3. Decortication: The facet joints are destroyed, and the laminae and transverse processes are decorticated.
4. Bone Grafting: Copious autograft (iliac crest) or high-quality allograft is packed into the decorticated beds.
5. Postoperative Care: Because no instrumentation is used, the patient must be immobilized in a rigid cast or custom TLSO for 4 to 6 months until solid fusion is confirmed.

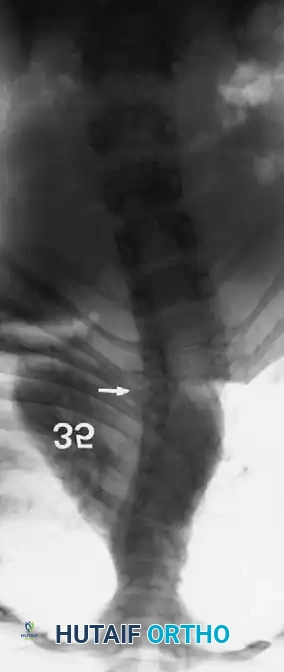
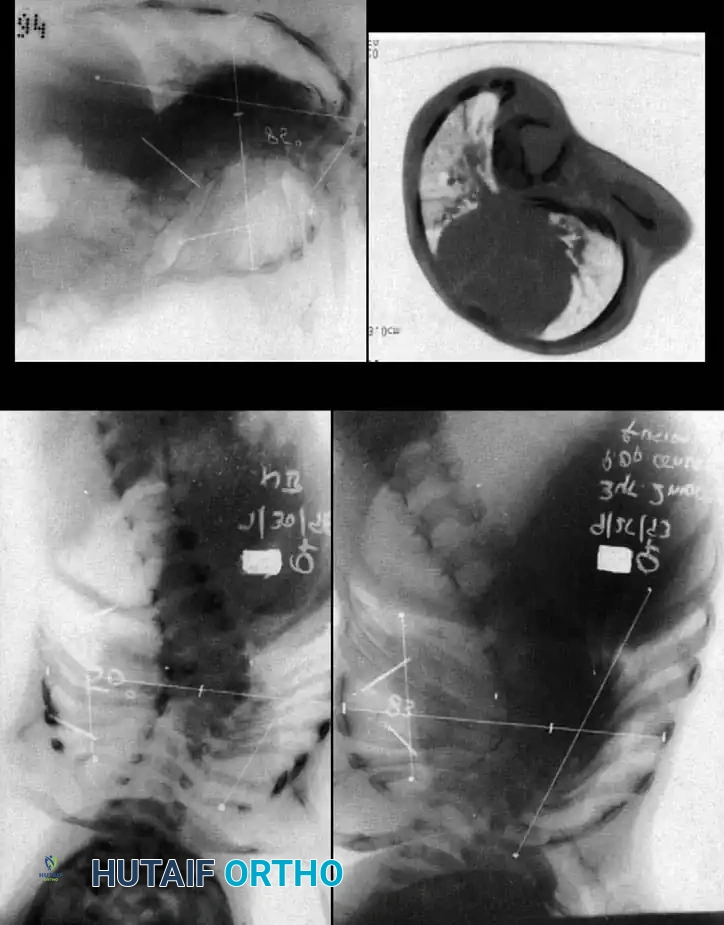
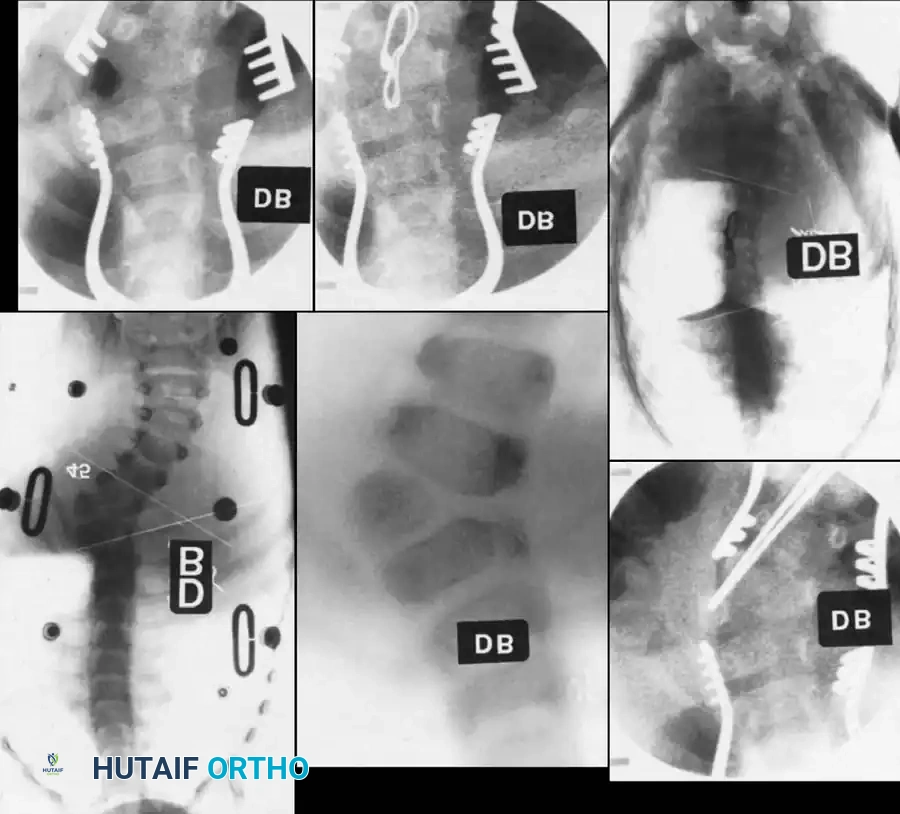
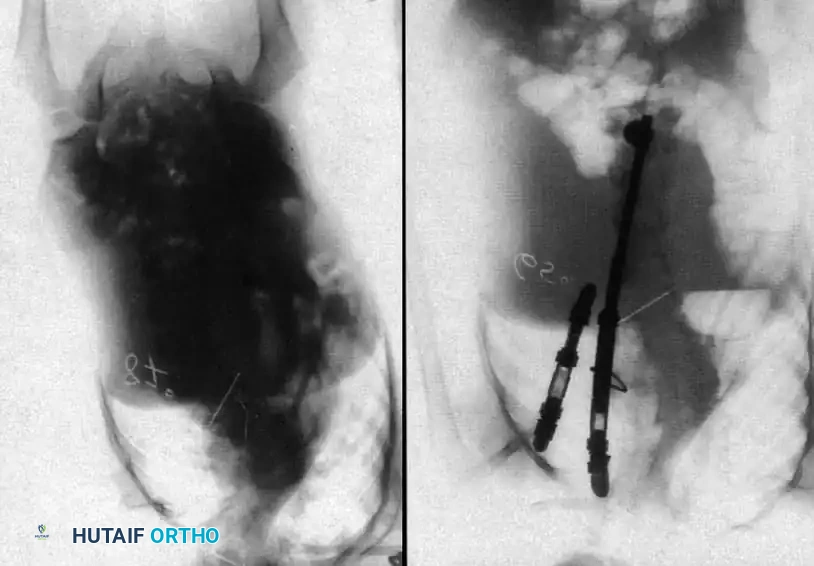
Radiographic examples of progressive congenital curves requiring early intervention.
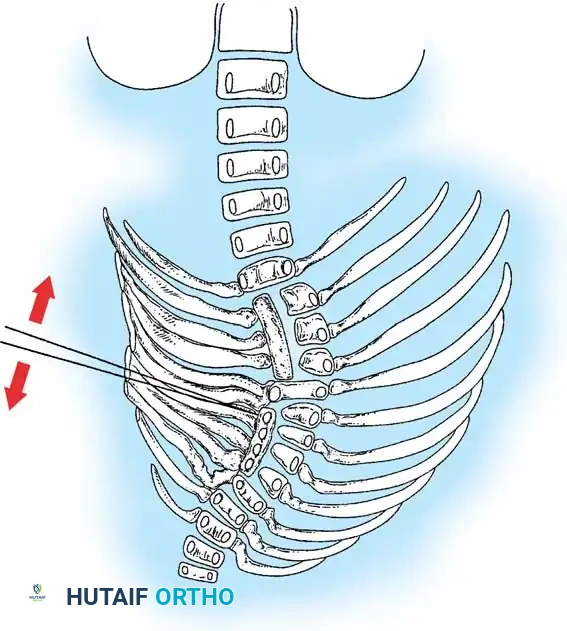
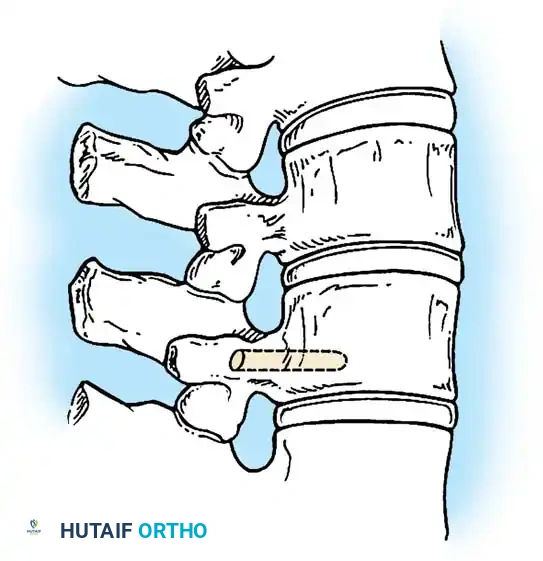
2. Combined Anterior and Posterior Convex Hemiepiphysiodesis
This technique harnesses the patient's remaining growth potential. By arresting growth on the convex side of the curve (both anteriorly and posteriorly) while allowing the concave side to continue growing, gradual spontaneous correction of the deformity can occur over time.
Indications:
* Young patients (typically under 5 years old).
* Progressive curves less than 50 degrees.
* Documented growth potential on the concave side (no unsegmented bars).
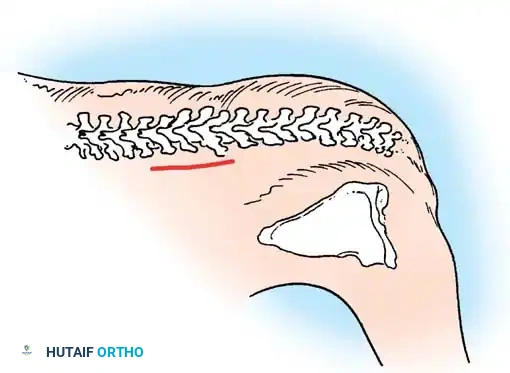
Surgical Steps:
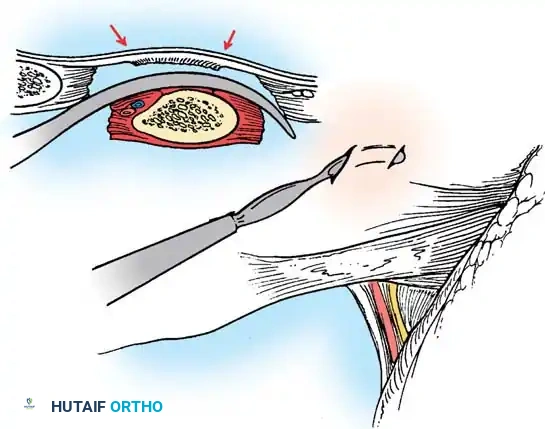
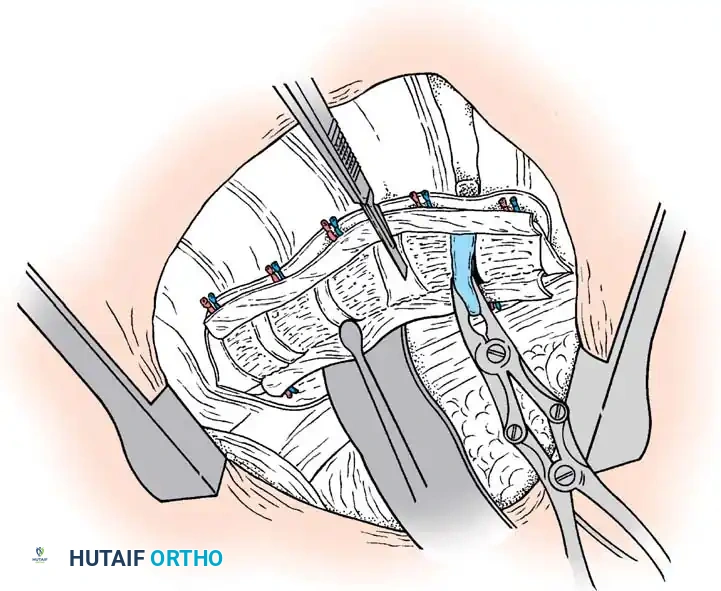
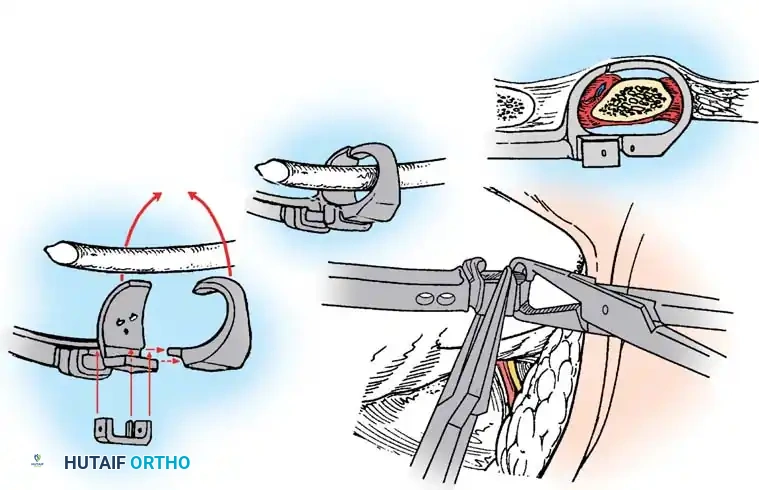
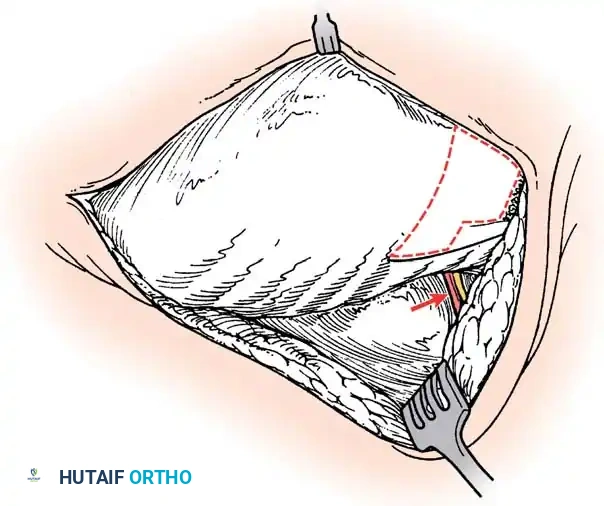
1. Anterior Approach: A thoracotomy or retroperitoneal approach is utilized to access the convex aspect of the anomalous vertebrae.
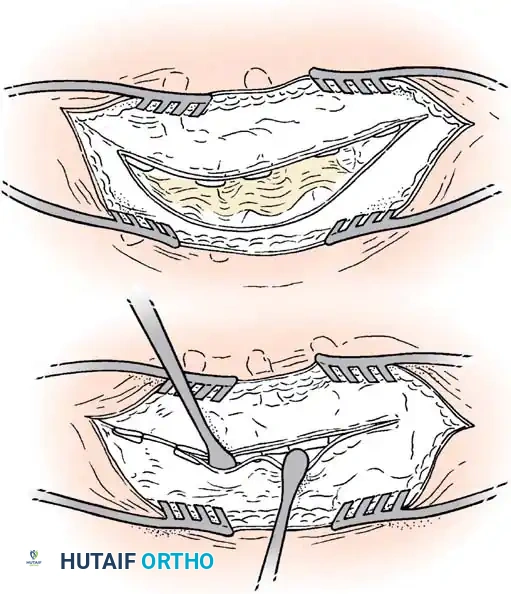
2. Discectomy and Epiphysiodesis: The discs on the convex side are excised, and the cartilaginous endplates (physes) are destroyed. The defects are packed with bone graft.
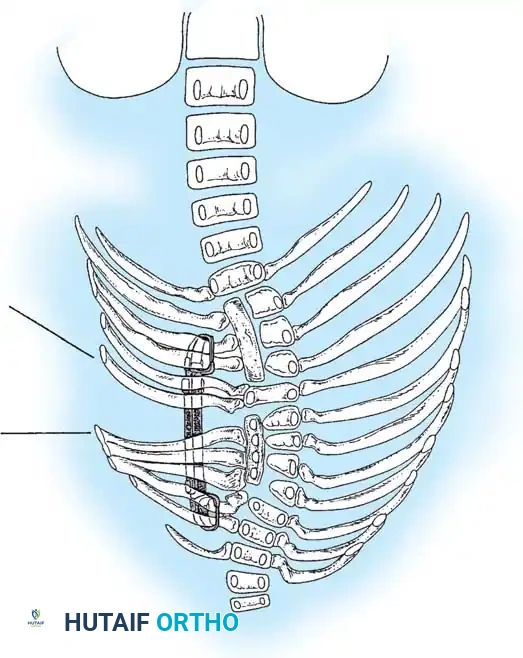
3. Posterior Approach: The patient is flipped prone. A unilateral posterior exposure of the convexity is performed.
4. Posterior Fusion: The convex facet joints are excised and fused.
Surgical Warning: The success of a hemiepiphysiodesis relies entirely on the presence of healthy, active growth plates on the concavity. If the concavity is tethered, this procedure will fail.
Surgical planning and execution of complex congenital curve corrections.
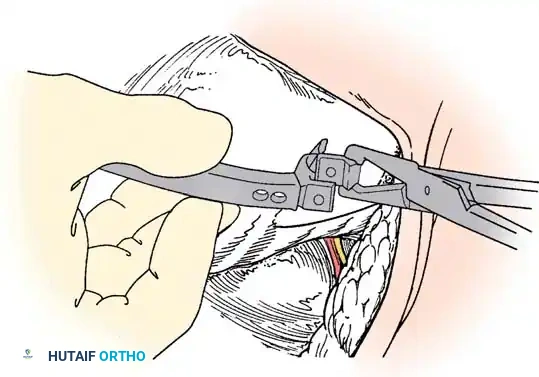
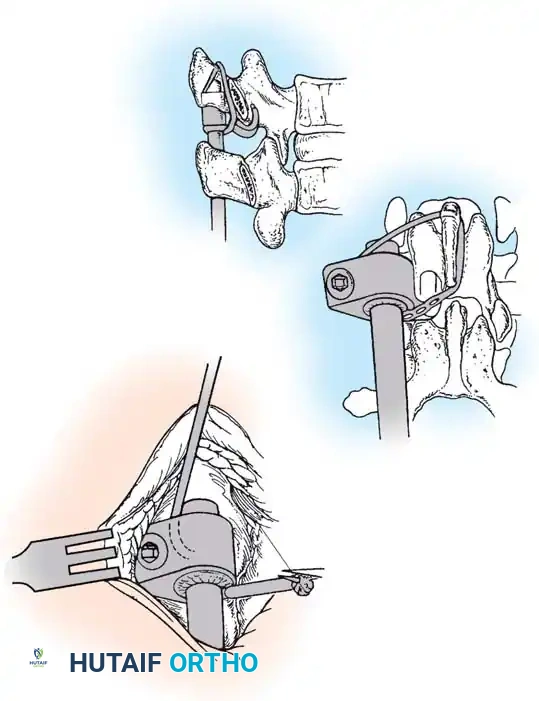
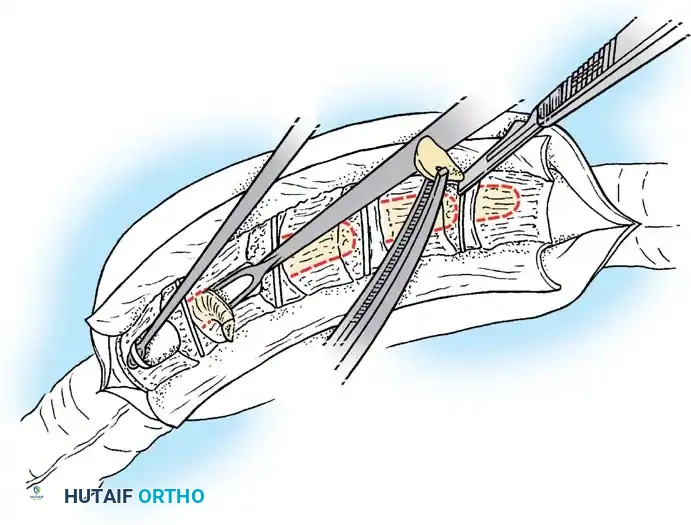
3. Hemivertebra Excision
Hemivertebra excision is the gold standard for a fully segmented, progressive hemivertebra, particularly in the lumbosacral junction where it causes severe coronal decompensation. Historically performed via a combined anterior-posterior approach, it is now frequently performed via an all-posterior, pedicle subtraction
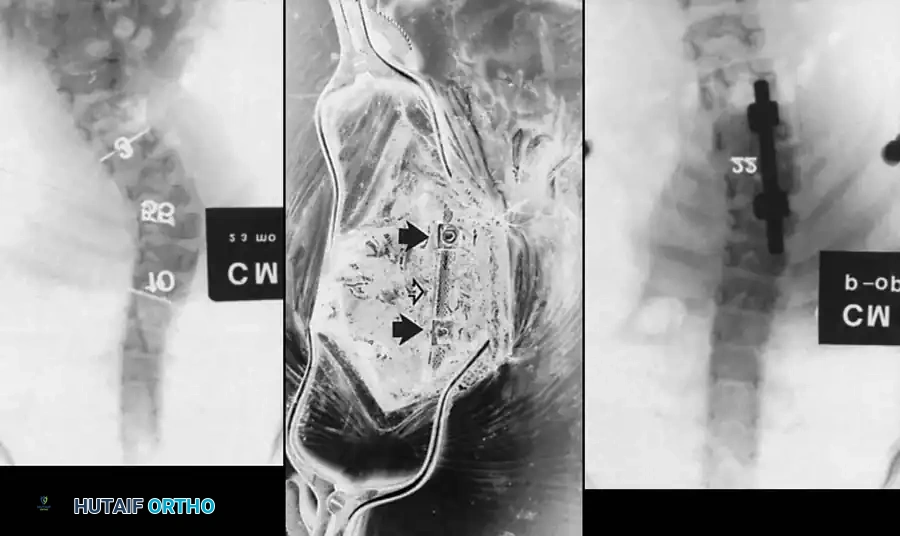
Associated Surgical & Radiographic Imaging




📚 Medical References
- congenital scoliosis: report of two cases, J Bone Joint Surg 14:555, 1932.
- Darling GE, McBroom R, Perrin R: Modifi ed anterior approach to the cervicothoracic junction, Spine 20:1519, 1995.
- Ebraheim NA, Skie M, Heck BE, et al: Vulnerability of the recurrent laryngeal nerve in the anterior approach to the lower cervical spine, Spine 22:2664, 1997.
- Fang HSY, Ong GB: Direct anterior approach to the upper cervical spine, J Bone Joint Surg 44A:1588, 1962.
- Fang HSY, Ong GB, Hodgson AR: Anterior spinal fusion: the operative approaches, Clin Orthop Relat Res 35:16, 1964.
- Fraser RD: A wide muscle-splitting approach to the lumbosacral spine, J Bone Joint Surg 64B:44, 1982.
- Freeman BL: The pediatric spine. In Canale ST, Beaty JH, eds: Operative pediatric orthopaedics, St Louis, 1991, Mosby. Graham AW III, Macmillan M, Fessler RG: Lateral extracavitary approach to the thoracic and thoracolumbar spine, Orthopedics 20:605, 1997.
- Hodgson AR, Stock FE, Fang HYS, et al: Anterior spinal fusion: the operative approach and pathological fi ndings in 412 patients with Pott’s disease of the spine, Br J Surg 48:172, 1960.
- Jasani V, Jaffray D: The anatomy of the iliolumbar vein: a cadaver study. J Bone Joint Surg 84B:1046, 2002.
- Johnson RM, McGuire EJ: Urogenital complications of anterior approaches to the lumbar spine, Clin Orthop Relat Res 154:114, 1981.
- Johnson RM, Southwick WO: Surgical approaches to the cervical spine. In Rothman RH, Simeone FA, eds: The spine, 2nd ed, Philadelphia, 1982, Saunders. Koriwchak MJ, Courey MS, Winkle M, et al: Vocal fold paralysis following the anterior approach to the cervical spine, Ann Otol Rhinol Laryngol 105:85, 1996.
- Lehman RM, Grunberg B, Hall T: Anterior approach to the cervicothoracic junction: an anatomic dissection, J Spinal Disord 10:33, 1997.
- Leventhal MR: Surgical approaches in the treatment of
You Might Also Like