Cervical Spine Fractures: Epidemiology, Surgical Anatomy, and Biomechanics
Key Takeaway
Cervical spine fractures are critical traumatic injuries often resulting from high-energy events like motor vehicle accidents, falls, or sports. They impact 2-6% of trauma patients, with 40% experiencing neurological involvement. Understanding detailed surgical anatomy, especially of the upper cervical spine (C0-C2) and key ligaments like the transverse ligament, is crucial for effective management.
Cervical Spine Fracture: An Interactive Orthopedic Mastery Module
Introduction & Epidemiology
Cervical spine fractures represent a critical subset of traumatic injuries, demanding immediate and precise management due to the potential for catastrophic neurological sequelae. Understanding the epidemiology and mechanisms of these injuries is paramount for effective triage and treatment planning.
Cervical spine injuries typically result from high-energy transfer mechanisms. The most common etiologies include:
*
Motor Vehicle Accidents (MVAs):
Accounting for approximately 45% of all cervical spine trauma. These often involve significant deceleration forces, direct impact, or complex loading patterns.
*
Falls from Height:
Contributing to roughly 20% of cases, particularly in elderly populations or those with pre-existing conditions affecting balance or bone quality.
*
Athletic Participation:
Responsible for about 15% of injuries, predominantly observed in contact sports such as American football, rugby, and diving. The forces involved often include axial loading, hyperflexion, or hyperextension.
*
Acts of Violence:
Also accounting for approximately 15%, encompassing penetrating trauma, assaults, and gunshot wounds, which can lead to complex fracture patterns and direct neurological compromise.
A critical consideration in cervical spine trauma is the high incidence of neurological involvement. Approximately 40% of patients with cervical spine fractures will sustain some form of neurologic injury, ranging from transient radiculopathy to complete spinal cord transection. It is notable that spinal cord damage is more frequently associated with fractures and dislocations in the lower cervical spine (C3-C7) compared to the upper cervical spine (C1-C2). This predilection is attributed to the relatively larger spinal canal diameter in the upper cervical region and the unique biomechanics of the craniocervical junction.
Overall, cervical spine fractures are present in 2% to 6% of all trauma patients presenting to emergency departments. When considering patients with spinal cord trauma, the cervical region is implicated in a significant proportion, ranging from 19% to 51% of cases. Furthermore, a substantial 20% of trauma patients who present with any focal neurologic deficit will have an associated cervical spine fracture, underscoring the necessity for a high index of suspicion and comprehensive radiographic evaluation in this demographic. Early diagnosis and stabilization are crucial to minimize secondary injury and optimize long-term outcomes.
Surgical Anatomy & Biomechanics
A profound understanding of cervical spine anatomy and its intricate biomechanics is foundational for any orthopedic surgeon managing cervical spine fractures. The cervical spine comprises seven vertebrae, distinguished by unique morphological features and specialized ligamentous and muscular attachments that collectively permit extensive range of motion while providing vital protection for the spinal cord and exiting nerve roots.
Upper Cervical Spine (C0-C2)
C0 (Occiput):
The base of the skull articulates with C1, forming the atlanto-occipital joint. This joint allows for approximately 25 degrees of flexion and extension, contributing significantly to total neck movement. Stability is primarily conferred by the tectorial membrane and the alar ligaments.
*
Tectorial Membrane:
A superior extension of the posterior longitudinal ligament, it attaches to the clivus superiorly and C2 body inferiorly, limiting flexion and extension at the atlanto-occipital and atlanto-axial joints.
*
Alar Ligaments:
Paired ligaments originating from the apex of the odontoid process and inserting onto the medial aspects of the occipital condyles. They restrict axial rotation and lateral bending at the craniocervical junction.
C1 (Atlas):
Uniquely structured, the atlas is the first cervical vertebra and lacks a vertebral body and a spinous process. Its primary function is to support the skull and facilitate rotation.
*
Lateral Masses:
These are the large, primary weight-bearing components, articulating superiorly with the occipital condyles and inferiorly with the superior articular facets of C2. They are crucial for transmitting forces between the skull and the rest of the spine.
*
Anterior Arch:
Features an anterior tubercle and a fovea dentis, which articulates with the odontoid process. This articulation is stabilized anteriorly by the
transverse ligament of the atlas
.
*
Transverse Ligament of the Atlas (Gray’s Anatomy):
This robust ligament originates from the medial aspect of one lateral mass and inserts into the medial aspect of the contralateral lateral mass, holding the odontoid process firmly against the anterior arch of C1. It is the primary restraint against anterior translation of C1 on C2 and provides critical stability for the atlanto-axial joint.
*
Cruciate Ligament:
Composed of the transverse ligament and superior/inferior longitudinal bands, further reinforcing craniocervical stability.
*
Posterior Arch:
Features a posterior tubercle, representing a rudimentary spinous process. The vertebral artery traverses the posterior arch through the groove for the vertebral artery.

Depiction of the atlas (C1) anatomy, highlighting the lateral masses and the position of the transverse ligament.

Articulated view of the C1-C2 complex, demonstrating the relationship of the atlas to the odontoid process.
C2 (Axis):
Distinguished by its prominent superior projection, the odontoid process (dens).
*
Odontoid Process:
Articulates with the anterior arch of C1, serving as a pivot point for C1 rotation. Its base is the most common site of fracture.
*
Pars Interarticularis:
The segment of bone between the superior and inferior articular facets. Fractures through this region are known as Hangman's fractures.
*
Superior Articular Facets:
Project superolaterally, articulating with the C1 lateral masses.
*
Inferior Articular Facets:
Articulate with the superior facets of C3.
*
Vertebral Artery:
Courses superiorly through the transverse foramina of C6 to C1, then turns medially across the posterior arch of C1 before entering the foramen magnum. Its tortuous course around C1-C2 makes it vulnerable to injury in fractures or dislocations of this region.

Detailed view of C2 (axis) anatomy, showing the odontoid process and pars interarticularis.
Approximately 50% of the total neck flexion and extension range of motion occurs between the occiput and C2, with 25 degrees at the occiput–C1 joint and 20 degrees at the C1–C2 joint. Crucially, C1-C2 accounts for approximately 50% of cervical rotation. This high degree of mobility, coupled with vital neurovascular structures, renders the craniocervical junction particularly susceptible to complex injuries.
Subaxial Cervical Spine (C3-C7)
The subaxial cervical vertebrae share common features, including:
*
Vertebral Body:
Anterior, cylindrical portion, weight-bearing.
*
Pedicles:
Connect the body to the posterior elements.
*
Laminae:
Form the posterior wall of the spinal canal.
*
Spinous Process:
Bifid from C2-C6, long and non-bifid at C7 (vertebra prominens).
*
Transverse Processes:
Contain the transverse foramina, through which the vertebral artery (C6 to C1) and venous plexus pass.
*
Superior and Inferior Articular Processes/Facets:
Form the synovial facet joints, which guide motion and provide stability against shear forces. The orientation of these facets influences the type and degree of motion permitted.
*
Uncovertebral Joints (Joints of Luschka):
Posterolateral articulations between the uncinate processes of the inferior vertebra and the inferolateral surface of the superior vertebral body. They contribute to lateral stability and guide flexion/extension, but can also be sources of osteophyte formation and nerve root impingement.

Schematic illustration of a typical subaxial cervical vertebra, highlighting key anatomical features.
Ligamentous Structures:
The robust ligamentous complex provides static stability to the cervical spine:
*
Anterior Longitudinal Ligament (ALL):
Thick, strong ligament running along the anterior aspect of the vertebral bodies, resisting hyperextension.
*
Posterior Longitudinal Ligament (PLL):
Runs along the posterior aspect of the vertebral bodies within the spinal canal, resisting hyperflexion and posterior disc herniation.
*
Ligamentum Flavum:
Connects adjacent laminae, elastic in nature, maintaining constant spinal canal diameter and assisting in extension.
*
Capsular Ligaments:
Surround the facet joints, providing significant resistance to shear and rotatory forces.
*
Interspinous Ligaments:
Connect adjacent spinous processes.
*
Supraspinous Ligament:
Runs along the tips of the spinous processes, continuous with the nuchal ligament in the cervical spine.

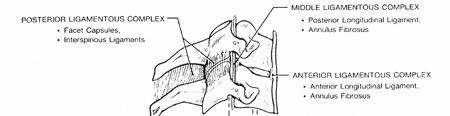
Sagittal view of the cervical spine, depicting the major longitudinal ligaments.
Musculature: The cervical muscles are critical for dynamic stability and motion. They are broadly categorized into superficial, intermediate, and deep layers, with intrinsic deep extensors (e.g., semispinalis cervicis, multifidus) being crucial for segmental stability.
Biomechanics of Stability:
The cervical spine's stability can be conceptualized using the
three-column theory (Denis)
, though primarily applied to the thoracolumbar spine, its principles are relevant:
*
Anterior Column:
ALL, anterior two-thirds of the vertebral body and annulus fibrosus.
*
Middle Column:
PLL, posterior one-third of the vertebral body and annulus fibrosus.
*
Posterior Column:
Pedicles, laminae, spinous processes, facet joints, and posterior ligamentous complex (ligamentum flavum, interspinous, supraspinous ligaments).
Injury to two or more columns often signifies instability.
The two-column theory (White and Panjabi) focuses on functional stability. It emphasizes the importance of both the anterior osteoligamentous complex (vertebral bodies, discs, ALL, PLL) and the posterior osteoligamentous complex (facet joints, ligamentum flavum, interspinous, supraspinous ligaments). Disruption of both complexes, particularly with significant facet involvement, indicates gross instability.
Understanding the specific contributions of these structures to resisting various forces (e.g., ALL for hyperextension, PLL and posterior ligaments for hyperflexion, facet capsules for rotation and shear) allows for accurate assessment of injury patterns and appropriate stabilization strategies.
Indications & Contraindications
The decision-making process for operative versus non-operative management of cervical spine fractures is multifaceted, balancing the goals of neural decompression, spinal stability, and patient safety.
Operative Indications
Surgical intervention is generally indicated for:
*
Spinal Instability:
As determined by fracture morphology (e.g., significant three-column injury, ligamentous disruption), displacement, angulation, or subluxation. Instability can be classified based on classification systems such as the AO Spine Cervical Spine Injury Classification System or the Subaxial Cervical Spine Injury Classification (SLIC) system, where a score of ≥5 often warrants surgical stabilization.
*
Progressive Neurologic Deficit:
Worsening motor or sensory function in the presence of a fracture or dislocation indicates ongoing spinal cord or nerve root compression requiring urgent surgical decompression.
*
Irreducible Dislocations:
Persistent facet dislocations or translational deformities after adequate closed reduction attempts (e.g., skull traction) often necessitate open reduction and internal fixation.
*
Vertebral Artery Injury with Instability:
Fractures involving the transverse foramen of C1-C7, especially with associated instability, may require stabilization to prevent further injury or to facilitate vertebral artery reconstruction if indicated.
*
Specific Unstable Fracture Types:
*
Odontoid Type II fractures (Anderson & D'Alonzo):
Particularly those with significant displacement (>5-6mm), angulation (>10 degrees), or in elderly patients, due to high rates of nonunion with conservative management. Odontoid Type III fractures with significant displacement may also benefit from surgery.
*
C1 Burst Fractures (Jefferson fractures):
With significant transverse ligament disruption (lateral mass displacement >7mm on open mouth odontoid view) or neurological compromise.
*
Hangman's Fractures (C2 traumatic spondylolisthesis):
Type II and Type IIA fractures (Levine-Edwards classification) due to instability and potential for neurological deficit.
*
Subaxial Bilateral Facet Dislocations:
These are inherently unstable and typically require surgical reduction and fusion.
*
Subaxial Burst Fractures:
Especially those with retropulsion into the spinal canal causing significant stenosis or neurological deficits.
*
Failure of Non-Operative Management:
Persistent instability, progressive deformity, or intractable pain despite adequate bracing or halo immobilization.
*
Polytrauma Patients:
Early stabilization of cervical spine injuries can facilitate overall patient care, mobilization, and pulmonary hygiene.
Non-Operative Indications
Conservative management is typically reserved for:
*
Stable Fractures:
*
Odontoid Type I fractures:
Often stable due to ligamentous attachments and treated with cervical orthosis.
*
Minimally displaced Odontoid Type III fractures:
May be managed with halo vest immobilization, especially in younger patients.
*
Stable C1 Fractures (Jefferson fractures):
Without significant transverse ligament disruption (lateral mass displacement <7mm) and no neurological deficit, managed with a hard collar or halo vest.
*
Hangman's Fractures Type I (Levine-Edwards):
Characterized by minimal displacement (<3mm) and no angulation, indicating an intact C2-C3 disc and posterior longitudinal ligament, often treated with a cervical orthosis or halo vest.
*
Stable Subaxial Compression Fractures:
Without signs of posterior column injury, significant angulation, or spinal canal compromise.
*
Isolated spinous process fractures (Clay-Shoveler's fracture):
Managed symptomatically with a cervical collar.
*
Minor Ligamentous Injuries:
Without demonstrable instability on static or dynamic imaging.
*
Neurologically Intact Patients:
With stable fracture patterns.
*
Patients with Significant Comorbidities:
Where the risks of surgery outweigh the benefits, and the fracture pattern allows for non-operative management.
*
Patient Refusal:
After thorough discussion of risks and benefits.
Contraindications
Absolute Contraindications:
*
Severe Medical Comorbidities:
Patients who cannot physiologically tolerate anesthesia and surgical stress (e.g., uncontrolled sepsis, severe cardiopulmonary compromise).
*
Uncontrolled Infection:
At the surgical site or systemic, requiring resolution prior to elective surgery.
Relative Contraindications:
*
Inability to Tolerate Immobilization:
For non-operative cases, a patient's inability to comply with brace or halo vest protocols may shift the indication towards surgery.
*
Severe Osteoporosis:
Affecting the ability to achieve adequate hardware purchase, necessitating alternative fixation strategies or cement augmentation.
*
Pre-existing Spinal Deformity:
May complicate standard approaches and require specialized planning.
Table: Operative vs. Non-Operative Indications for Cervical Spine Fractures
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Instability | AO Spine C > A0 or SLIC ≥ 5 | AO Spine A0, SLIC < 5 (if stable) |
| Neurology | Progressive deficit, acute cord compression, irreducible dislocation with deficit | Neurologically intact (unless instability/pain mandates surgery) |
| Fracture Type | Odontoid Type II (>5-6mm displacement/angulation), Type III with significant displacement; C1 burst (transverse ligament disruption >7mm); Hangman Type II/IIA; Bilateral facet dislocation; Unstable subaxial burst fractures. | Odontoid Type I, stable Type III; C1 stable (lateral mass displacement <7mm); Hangman Type I; Isolated stable compression fracture; Spinous process fracture. |
| Reduction | Failed closed reduction attempts | Successful closed reduction (maintained stability) |
| Pain/Deformity | Intractable pain or progressive deformity despite conservative treatment | Manageable pain, no progressive deformity |
| Comorbidity | Patient physiologically able to tolerate surgery | Significant comorbidities precluding surgery |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and careful patient positioning are paramount to optimize surgical outcomes and minimize complications in cervical spine fracture management.
Pre-Operative Planning
-
Comprehensive Patient Assessment:
- Detailed History: Mechanism of injury, associated symptoms, prior neck surgery, comorbidities (e.g., osteoporosis, inflammatory arthropathies, coagulopathies).
- Thorough Neurologic Examination: Document baseline motor strength (e.g., ASIA scale), sensory levels, reflexes, and bowel/bladder function. This serves as a critical reference for assessing post-operative changes.
- Concomitant Injuries: Evaluate for other traumatic injuries, particularly head trauma, chest injuries, and extremity fractures, which may influence timing and approach.
-
Advanced Imaging Review:
- Computed Tomography (CT) Scan: Essential for detailed bony anatomy. Axial, sagittal, coronal, and 3D reconstructions are critical for delineating fracture patterns, assessing spinal canal compromise, and identifying potential foramen transversarium involvement.
- Magnetic Resonance Imaging (MRI): Indispensable for evaluating soft tissue structures, including the spinal cord (edema, contusion, hemorrhage, transection), intervertebral discs (herniation), and ligaments (rupture). Crucial for assessing the integrity of the transverse ligament in C1 fractures and the posterior ligamentous complex in subaxial injuries.
- Dynamic Flexion/Extension Radiographs: While controversial in the acute setting due to the risk of neurological deterioration, they can be valuable in assessing chronic instability or for equivocal cases where stability remains uncertain after static imaging. Must be performed under direct physician supervision with strict attention to patient symptoms.
-
Computed Tomography Angiography (CTA) or Magnetic Resonance Angiography (MRA):
Indicated for fractures involving the transverse foramen (C1-C7), particularly C1-C2 fractures, subluxations, or high-energy mechanisms, to assess for vertebral artery injury (dissection, pseudoaneurysm, occlusion).

Axial CT image demonstrating a cervical spine fracture with significant canal compromise.

Sagittal MRI scan showing a cervical fracture with associated spinal cord edema and ligamentous injury.
-
Surgical Approach Selection: Based on the fracture morphology, instability pattern, location of neural compression (anterior vs. posterior), and surgeon preference. Decisions regarding anterior, posterior, or combined approaches are made at this stage.
-
Hardware Selection: Pre-operative templating from imaging helps determine appropriate plate length, screw sizes, and graft dimensions. Instrumentation systems vary, and familiarity with the chosen system is essential.
-
Anesthesia and Consultations: Coordination with anesthesia regarding airway management (awake intubation, fiberoptic intubation may be required), blood product availability, and potential for neuromonitoring (SSEP, MEP) and fluoroscopy. Neurosurgery consultation may be required for complex neurological injury patterns.
-
Closed Reduction Attempts: For dislocations (especially facet dislocations), closed reduction with skull traction (Gardner-Wells tongs or halo ring) can be attempted pre-operatively. Gradual weight addition, often under fluoroscopic guidance and neurological monitoring, is employed. Successful reduction often simplifies the surgical procedure and can improve neurological outcomes.
Patient Positioning
Maintaining strict cervical spine alignment and protecting the spinal cord during positioning is non-negotiable. Anesthesia and surgical teams must collaborate closely.
-
Anterior Approach (Supine Positioning):
- The patient is supine on the operating table.
- Head Support: A donut headrest, foam head ring, or Mayfield three-point skull clamp (for rigid head immobilization and avoidance of traction on the endotracheal tube) is used.
- Shoulder Depression: Gel rolls or tape are placed under the shoulders to gently depress them inferiorly. This helps to extend the cervical spine slightly and provides better fluoroscopic visualization of the lower cervical segments (C6-T1 junction).
- Neck Extension: A slight degree of neck extension may be achieved with a small roll under the shoulders/upper back, but care must be taken to maintain neutral alignment or gentle traction if a fracture/dislocation is present.
- Traction: If skull traction was applied pre-operatively, it is maintained during positioning and throughout the case, often using a halo ring or Gardner-Wells tongs.
-
Neuromonitoring:
Somatosensory Evoked Potentials (SSEPs) and Motor Evoked Potentials (MEPs) are typically used for continuous monitoring of spinal cord function during positioning and surgery.

Patient positioned supine for an anterior cervical approach, with appropriate head and shoulder support.
-
Posterior Approach (Prone Positioning):
- The patient is carefully log-rolled from supine to prone while maintaining cervical spine alignment. A minimum of 4-6 personnel is required.
- Chest and Pelvic Support: Radiolucent chest rolls, a Jackson table with bolsters, or a four-poster frame are used to support the torso, allowing the abdomen to hang free. This reduces intra-abdominal pressure, minimizing epidural venous bleeding.
- Head Support: The head is typically secured in a Mayfield three-point skull clamp (preferred) or a specific prone headrest. The clamp allows for fine adjustments of neck flexion/extension and rotation, crucial for optimal exposure and reduction.
- Cervical Alignment: The neck is often positioned in slight flexion (often 10-15 degrees) to facilitate exposure of the posterior elements and reduction of certain fracture types. However, this must be carefully managed to avoid excessive flexion, especially in unstable injuries.
- Pressure Point Protection: All pressure points (eyes, ears, nose, breasts, genitalia, knees, ankles) are meticulously padded to prevent pressure sores or nerve palsies.
-
Neuromonitoring:
SSEPs and MEPs are essential during prone positioning and throughout the posterior cervical procedure.

Patient positioned prone for a posterior cervical approach, demonstrating proper head and torso support.
Detailed Surgical Approach / Technique
Surgical management of cervical spine fractures involves diverse approaches depending on the fracture type, location, and the need for decompression and stabilization. Here, we outline the general principles and steps for common anterior and posterior approaches.
Anterior Cervical Discectomy and Fusion (ACDF) / Anterior Cervical Corpectomy and Fusion (ACCF)
The anterior approach is widely used for C2-C7 fractures, particularly for direct anterior decompression of the spinal cord and robust ventral stabilization.
-
Incision and Exposure:
- Incision Type: A transverse skin crease incision (typically between C4-C6) is generally preferred for subaxial pathology. For multi-level disease or to facilitate exposure, an oblique or longitudinal incision along the anterior border of the sternocleidomastoid (SCM) can be used.
- Platysma: The platysma muscle is identified and incised in line with the skin incision. It can be sharply dissected or cauterized.
- Internervous Plane: The anterior approach utilizes a relatively avascular and internervous plane. The SCM is retracted laterally. The carotid sheath (containing the common carotid artery, internal jugular vein, and vagus nerve) is identified and carefully retracted laterally. The strap muscles (sternohyoid, sternothyroid, omohyoid) are retracted medially.
- Deep Dissection: The prevertebral fascia is identified. The esophagus and trachea lie deep to the strap muscles and are retracted medially. Care must be taken to identify and protect the recurrent laryngeal nerve, which typically ascends in the tracheoesophageal groove. Its course varies, with the right recurrent laryngeal nerve often hooking around the subclavian artery and the left around the aortic arch, making it more predictable.
- Longus Colli Muscles: Once the prevertebral fascia is opened, the longus colli muscles are exposed. These paired muscles originate from the cervical transverse processes and insert onto the anterior aspects of the vertebral bodies. They are often partially detached from the vertebral body to expose the anterior annulus and vertebral endplates.
-
Level Identification:
Fluoroscopy is essential for accurate level identification. A spinal needle can be inserted into the disc space to confirm the correct level.

Illustration of the anterior cervical approach, demonstrating retraction of muscles and neurovascular structures.
-
Decompression and Preparation:
- Discectomy (ACDF): For burst fractures with posterior displacement of disc material, a complete discectomy is performed. The annulus fibrosus is incised, and disc material is removed using rongeurs, curettes, and pituitary grasping forceps. The posterior longitudinal ligament (PLL) is meticulously resected to decompress the spinal cord.
- Corpectomy (ACCF): For severe burst fractures involving the vertebral body or multilevel pathology, a corpectomy is performed. The involved vertebral body is removed, typically using osteotomes and high-speed burrs, until the posterior cortical wall is adequately resected, and the spinal cord is fully decompressed.
- Endplate Preparation: The endplates of the adjacent vertebral bodies are prepared by removing cartilage and sclerotic bone to create a bleeding bed for fusion.
-
Reduction and Fixation:
- Reduction of Dislocations: For anterior dislocations (e.g., bilateral facet dislocations), reduction can often be achieved anteriorly by distracting the involved segment with temporary pins in adjacent vertebral bodies, followed by cantilever bending with the plate. Gentle posterior translation of the superior vertebra relative to the inferior can also be achieved.
-
Grafting:
- ACDF: A structural graft (autograft from iliac crest, allograft, or PEEK cage) is inserted into the disc space.
- ACCF: A larger structural cage or fibular allograft is typically used to reconstruct the corpectomy defect.
-
Plating:
A cervical plate is then applied to the anterior aspects of the vertebral bodies, spanning the fused segments. Screws are inserted bicortically for maximal purchase, ensuring proper trajectory to avoid neurovascular structures and adjacent discs.

Anterior cervical plate fixation after discectomy and fusion, showing screw placement.
-
Closure: Layered closure of the longus colli fascia, platysma, and skin. A drain may be placed, especially after corpectomy.
Posterior Cervical Fusion (PCF)
The posterior approach is indicated for posterior compression, instability from posterior ligamentous complex disruption, irreducible facet dislocations, or fractures of C1 and C2 requiring posterior fixation.
-
Incision and Exposure:
- Incision Type: A midline longitudinal incision extending from the occiput (for C1/C2 fusions) or C2 spinous process down to the required caudal level (e.g., C7/T1).
- Subperiosteal Dissection: The fascia is incised in the midline, and the muscle attachments (nuchal ligament, trapezius, rhomboids, splenius, semispinalis) are meticulously stripped from the spinous processes and laminae using electrocautery and periosteal elevators. This dissection should be as subperiosteal as possible to minimize muscle damage and preserve the nuchal ligament for closure.
- Exposure: The laminae, spinous processes, and lateral masses are exposed. For C1-C2 fusions, the posterior arch of C1 and the lamina/spinous process of C2 are exposed. For subaxial fusions, the lateral masses and facet capsules are exposed.
-
Reduction and Decompression:
- Reduction of Facet Dislocations: For unilateral or bilateral facet dislocations, reduction can often be achieved intraoperatively. This may involve gentle distraction, leverage with reduction clamps, or direct manipulation. If closed reduction attempts failed, an open reduction may be necessary. If the facets are locked, a partial facetectomy may be required to disengage them.
- Decompression (Laminectomy/Laminoplasty): For posterior spinal cord compression (e.g., from lamina fragments, severe kyphosis with cord impingement, or multilevel stenosis), a laminectomy (removal of lamina) or laminoplasty (hinged door or open-door technique) may be performed to decompress the spinal cord.
-
Fixation:
-
C1-C2 Fusion (Harms/Goel-Laure Technique):
This technique involves placing screws into the C1 lateral masses and C2 pedicles or pars interarticularis. Rods connect the screws, and bone graft is placed for fusion.
- C1 Lateral Mass Screws: Placed by identifying the posterior arch, then directing the screw inferomedially. Careful attention to vertebral artery anatomy is paramount.
-
C2 Pars/Pedicle Screws:
Placed into the pars interarticularis or pedicle. The entry point is usually superior and medial to the C2-C3 facet joint, aiming slightly medially and superiorly to avoid the vertebral artery anteriorly and the spinal canal medially.

C1-C2 posterior fixation using lateral mass and pedicle screws (Harms technique).
-
Subaxial Fixation (C3-C7):
- Lateral Mass Screws: The most common method for subaxial posterior fixation. The entry point is typically at the center of the lateral mass (Roy-Camille or Magerl techniques). Screws are directed laterally and superiorly to avoid nerve roots and the vertebral artery.
- Pedicle Screws: Can be used in the lower cervical spine (C7 and occasionally C6 or C5) where pedicles are sufficiently large. They offer superior biomechanical stability but require precise placement due to the proximity of the spinal cord and vertebral artery. Navigated surgery is often beneficial for pedicle screw placement.
-
Bone Grafting:
Autograft (local bone, iliac crest) or allograft is placed over the decorticated laminae and facet joints to promote fusion.

Subaxial cervical posterior fixation utilizing lateral mass screws and connecting rods.
-
C1-C2 Fusion (Harms/Goel-Laure Technique):
This technique involves placing screws into the C1 lateral masses and C2 pedicles or pars interarticularis. Rods connect the screws, and bone graft is placed for fusion.
-
Closure: Meticulous layered closure, reapproximating the nuchal ligament and paraspinal muscles to restore anatomical layers. A drain may be placed.
Complications & Management
Despite advancements in surgical techniques and technology, cervical spine fracture surgery is associated with a range of potential complications. Vigilant intra-operative monitoring and comprehensive post-operative care are crucial for early detection and effective management.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication Category | Specific Complication | Incidence (Approx.) | Salvage Strategy |
|---|---|---|---|
| Neurological | New/Worsening Neurologic Deficit | 1-5% | Immediate re-evaluation (imaging), re-exploration for decompression/hematoma evacuation, spinal cord cooling, steroid pulse, targeted rehabilitation. |
| C5 Nerve Root Palsy | 2-10% (Posterior) | Often transient; physiotherapy, nerve mobilization, bracing. Rarely surgical exploration/neurolysis for persistent severe deficits. | |
| Dural Tear / CSF Leak | 1-5% | Intraoperative primary repair (suture/patch), fibrin sealant, lumbar drain (post-op), strict bed rest, re-exploration if persistent leak/pseudomeningocele. | |
| Vascular | Vertebral Artery Injury | <1% | Intraoperative direct repair if possible, ligation (with collateral flow), angiography, embolization, antiplatelet/anticoagulation, consider foramen expansion. |
| Epidural Hematoma | <1% | Urgent surgical evacuation. | |
| Implant-Related | Hardware Malposition | 1-5% | Intraoperative revision. Post-op revision if symptomatic (neurologic deficit, dysphagia, pain) or mechanically failing. |
| Hardware Failure (Pullout/Break) | 2-10% | Revision surgery with stronger fixation, longer construct, alternative approach, consider cement augmentation. Prolonged external immobilization. | |
| Fusion-Related | Nonunion / Pseudoarthrosis | 5-15% | Revision surgery with debridement, additional bone grafting (autograft), stronger/longer instrumentation, biologic adjuncts (e.g., BMP), consider change in approach (e.g., adding posterior fusion to failed anterior). |
| Adjacent Segment Disease (ASD) | 2-4% per year | Initial non-operative management (pain control, PT). Surgical intervention (decompression, fusion) for progressive symptoms, neurological deficit, or instability. | |
| Infection | Surgical Site Infection (SSI) | 1-5% | Superficial: Wound care, oral antibiotics. Deep: Surgical debridement, intravenous antibiotics, irrigation, possibly hardware removal (after fusion), flap coverage for chronic/recalcitrant infections. |
| Airway/Swallowing | Dysphagia | 10-70% (Post-ACDF) | Often transient (due to swelling/esophageal manipulation). Soft diet, speech/swallowing therapy, steroids. Surgical exploration for severe cases (hematoma, esophageal perforation). |
| Dysphonia / Recurrent Laryngeal Nerve Palsy | 5-10% (Post-ACDF) | Often transient. Speech therapy. ENT evaluation. May require re-exploration for hematoma. | |
| General | Post-Operative Hematoma | 1-5% | Urgent surgical evacuation, especially if causing airway compromise or neurological deterioration. |
| Myelopathy (from positioning) | <1% | Prevention through meticulous positioning and neuromonitoring. If suspected, immediate repositioning, surgical decompression if indicated. |
Management Principles
- Prevention: The best strategy is prevention through meticulous surgical technique, careful patient selection, thorough pre-operative planning (including imaging review and neuromonitoring), and appropriate perioperative antibiotic prophylaxis.
- Early Detection: Neuromonitoring (SSEP, MEP) is crucial for intraoperative detection of neurological compromise. Close post-operative neurological checks and vital sign monitoring are essential.
- Imaging: Post-operative plain radiographs are routine. If complications are suspected (e.g., hardware malposition, new neurological deficit, severe dysphagia), a CT scan or MRI may be necessary.
- Multidisciplinary Approach: Managing complex complications often requires collaboration with neurologists, intensivists, infectious disease specialists, ENT specialists, and rehabilitation physicians.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following cervical spine fracture stabilization is critical for optimizing functional recovery, preventing long-term complications, and facilitating a safe return to activities. Protocols are individualized based on the fracture type, surgical approach, stability of fixation, and presence of neurological deficits.
Phase 1: Immediate Post-Operative (Days 0-6 Weeks)
Goals: Protect surgical fixation, control pain, prevent secondary complications, initiate early mobility.
-
Immobilization:
- External Orthosis: A rigid cervical collar (e.g., Miami J, Aspen) or a cervicothoracic orthosis (CTO) is typically prescribed, especially for single-level anterior fusions, or multi-level fusions with stable constructs.
- Halo Vest: May be indicated for highly unstable fractures, failed fusion, or as an adjunct after complex C1-C2 fusions, providing maximal immobilization.
- Duration: Generally 6-12 weeks, depending on the fracture healing and surgeon preference.
- Pain Management: Multimodal analgesia (opioids, NSAIDs, acetaminophen, muscle relaxants) to facilitate early mobilization and minimize opioid dependence.
- Wound Care: Daily inspection of incision site for signs of infection (erythema, swelling, discharge). Dressing changes as per protocol.
-
Early Mobilization:
- Out of bed activity, ambulation with assistance as tolerated, ensuring maintenance of spinal precautions.
- Gentle diaphragmatic breathing exercises and upper extremity range of motion (out of brace/collar) to prevent stiffness and deep vein thrombosis.
- Avoidance of cervical spine flexion, extension, rotation, and lateral bending, as dictated by the specific brace.
- Neurological Monitoring: Frequent neurological checks to detect any new or worsening deficits.
- Patient Education: Reinforce spinal precautions, proper body mechanics, and warning signs of complications.
Phase 2: Early Recovery / Progressive Strengthening (Weeks 6-12)
Goals: Gradually increase cervical range of motion (ROM) and strength, enhance postural control, wean from external immobilization (if appropriate).
- Weaning from Brace: If radiographs demonstrate signs of early fusion and clinical stability, the external orthosis may be gradually weaned. This decision is made by the surgeon based on fracture healing and fusion progress.
-
Gentle Range of Motion:
- Initiate active-assisted or active cervical ROM exercises, carefully staying within pain-free limits.
- Focus on global neck movements (flexion, extension, lateral bending, rotation) with gentle stretches.
- Isometric Strengthening: Begin isometric exercises for neck musculature (flexors, extensors, rotators) to restore muscle strength without stressing the fusion site.
- Scapular Stabilization: Strengthening exercises for the periscapular muscles (rhomboids, trapezius, serratus anterior) to improve shoulder girdle stability and reduce cervical strain.
- Core Stabilization: Education and exercises for abdominal and core musculature to improve overall spinal stability.
- Avoidance: Still restrict heavy lifting, overhead activities, twisting motions, and high-impact activities.
Phase 3: Advanced Strengthening & Return to Activity (Months 3-6+)
Goals: Maximize strength, endurance, and flexibility; improve proprioception; gradually return to sport/work-specific activities.
- Aggressive Strengthening: Progress to dynamic strengthening exercises for cervical and upper extremity muscles, using resistance bands, light weights, and bodyweight exercises.
- Proprioception and Balance Training: Incorporate exercises to improve neck and head proprioception and balance, crucial for complex motor tasks and preventing re-injury.
- Cardiovascular Conditioning: Gradually increase cardiovascular activity (walking, cycling, swimming) to improve overall fitness.
- Functional Training: Tailored exercises to mimic work or sport-specific movements, progressively increasing intensity and complexity.
-
Return to Activity:
- Gradual return to light duty work and recreational activities.
- High-impact sports, contact sports, or activities involving significant axial loading are typically restricted for 6-12 months post-fusion, contingent on radiographic evidence of solid fusion and excellent clinical recovery.
- Final clearance for unrestricted activity should come from the treating surgeon, often following a confirmatory CT scan to assess fusion status.
- Monitoring Neurological Recovery: For patients with pre-existing neurological deficits, ongoing physical and occupational therapy to maximize motor and sensory recovery, address spasticity, and adapt to functional limitations.
Throughout all phases, a close working relationship between the surgeon, physical therapist, and occupational therapist is vital to ensure protocol adherence, monitor progress, and modify the rehabilitation plan as needed. Education regarding ergonomic principles and lifelong spinal health maintenance is also paramount.
Summary of Key Literature / Guidelines
The management of cervical spine fractures is continuously refined through evidence-based research and expert consensus. Key guidelines and classification systems inform current practice.
Classification Systems
- AO Spine Cervical Spine Injury Classification System: This comprehensive system provides a standardized language for describing all cervical spine fractures and dislocations (C0-C7). It categorizes injuries based on morphology (A: compression, B: tension, C: translation), neurological status (N0-N4), and presence of facet injury (F0-F4). Its systematic approach aids in predicting stability and guiding treatment decisions.
- Subaxial Cervical Spine Injury Classification (SLIC) System: Developed specifically for subaxial injuries (C3-C7), the SLIC score integrates three components: injury morphology (compression, burst, distraction, rotation), integrity of the disco-ligamentous complex (DLC), and neurological status. A score ≥5 typically indicates an operative injury, while a score ≤3 suggests non-operative management, with intermediate scores requiring clinical judgment.
-
Anderson & D'Alonzo Classification for Odontoid Fractures:
- Type I: Oblique fracture through the tip of the odontoid. Generally stable, treated non-operatively.
- Type II: Fracture at the base of the odontoid. Most common type, high rate of nonunion, often requires surgery (anterior odontoid screw or posterior C1-C2 fusion), especially with >5-6mm displacement or >10 degrees angulation.
- Type III: Fracture extending into the body of C2. Larger cancellous bone surface, better healing potential than Type II. Management varies based on displacement and age (halo vs. surgery).
-
Levine and Edwards Classification for Hangman's Fractures (C2 Traumatic Spondylolisthesis):
- Type I: Bilateral C2 pars interarticularis fractures with <3mm anterior C2-C3 displacement and no angulation. Stable, intact C2-C3 disc and PLL. Treated with rigid collar.
- Type II: Significant C2-C3 displacement (>3mm) and/or angulation. C2-C3 disc is disrupted. Unstable. Often requires halo vest or surgical stabilization.
- Type IIA: Minimal C2-C3 displacement but severe angulation. Result of a flexion-distraction injury, C2-C3 disc often severely disrupted. Distraction in traction can worsen deformity; requires extension for reduction. Unstable, often operative.
- Type III: Type II with unilateral or bilateral C2-C3 facet dislocation. Highly unstable, typically requires surgical reduction and fusion.
Evidence-Based Recommendations & Trends
- Initial Resuscitation and Immobilization: Consensus emphasizes immediate spinal immobilization (rigid cervical collar, backboard) at the scene, followed by meticulous log-rolling and comprehensive ATLS protocol adherence.
- Neurological Deterioration: Any signs of neurological decline mandate immediate re-evaluation, imaging (CT/MRI), and consideration for emergent surgical decompression and stabilization.
- Timing of Surgery: While specific guidelines vary, the trend favors early surgical stabilization (within 24-72 hours) for unstable fractures with neurological deficits, as this has been associated with improved neurological recovery and reduced complications. For neurologically intact patients with unstable injuries, early surgery is also often favored to facilitate rehabilitation and reduce hospital stay.
-
Surgical Approach:
- Anterior Cervical Approach: Preferred for anterior compression (e.g., burst fractures, disc herniation with cord compression), kyphotic deformity, and for single or two-level fusions, offering excellent biomechanical stability with plating.
- Posterior Cervical Approach: Indicated for instability of the posterior column, irreducible facet dislocations, C1-C2 fractures requiring fusion, and for multi-level fusions, particularly for long constructs or severe kyphosis.
- Combined Approach: May be necessary for highly unstable injuries (e.g., three-column injuries), severe deformities, or revision surgery, to achieve circumferential decompression and robust stability.
- Hardware and Fusion: Modern instrumentation (lateral mass screws, pedicle screws, anterior plates, interbody cages) provides rigid fixation, allowing for earlier mobilization. The choice of bone graft (autograft vs. allograft vs. biologics) depends on patient factors, defect size, and surgeon preference. Autograft remains the gold standard for fusion rates.
- Vertebral Artery Injury: Incidence is low but significant. Screening (CTA/MRA) is recommended for fractures involving the transverse foramen, C1-C2 subluxation, and hangman's fractures. Management ranges from observation with anticoagulation to endovascular intervention or surgical repair/ligation.
- Neuromonitoring: Intraoperative SSEPs and MEPs are considered standard of care during cervical spine surgery to detect impending neurological compromise and guide surgical maneuvers.
The AO Spine Knowledge Forum and publications from organizations like the North American Spine Society (NASS) continually update guidelines and research, providing valuable resources for evidence-based practice in cervical spine trauma. Continued engagement with this literature is essential for any orthopedic spine surgeon.
Clinical & Radiographic Imaging




You Might Also Like