Lumbar Spine Applied Anatomy: Master the Posterior Surgical Approach

Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Lumbar Spine Applied Anatomy: Master the Posterior Surgical Approach. The lumbar spine applied surgical anatomy involves understanding superficial and deep muscle layers, detached as a mass during posterior approach. Key landmarks include the thick spinous processes, posterior superior iliac spine, and iliac crest, crucial for orientation. A midline incision follows the spinous processes, healing well. Dissection reveals the dorsal lumbar fascia and supraspinous ligaments, forming a sheath for sacrospinalis muscles.
Lumbar Spine Applied Anatomy: Master the Posterior Surgical Approach
Introduction & Epidemiology
The posterior approach to the lumbar spine is a cornerstone procedure in orthopedic and neurosurgical practice, providing direct access to the posterior vertebral elements, neural structures, and disc space. This approach is fundamental for a myriad of spinal pathologies, including degenerative conditions, traumatic injuries, infections, and deformities. Understanding the intricate applied anatomy, meticulous surgical technique, and potential pitfalls associated with this approach is paramount for residents, fellows, and practicing spine surgeons. Mastery of posterior lumbar anatomy facilitates precise surgical execution, minimizes iatrogenic injury, and optimizes patient outcomes.
Lumbar spinal pathologies constitute a significant burden on global healthcare systems. Degenerative conditions such as lumbar spinal stenosis (LSS), degenerative disc disease (DDD), and spondylolisthesis are increasingly prevalent with an aging population. Lumbar spinal stenosis, for instance, affects up to 11% of the adult population, with surgical intervention demonstrating superior outcomes compared to conservative management in carefully selected patients, particularly those with neurogenic claudication refractory to non-operative modalities. Similarly, lumbar disc herniation (LDH), while often amenable to non-operative treatment, necessitates surgical decompression in cases of refractory radiculopathy, progressive neurological deficit, or cauda equina syndrome. Traumatic lumbar spine fractures, particularly those involving posterior column disruption or neurological compromise, frequently require posterior stabilization to restore spinal column integrity and facilitate neurological recovery. Furthermore, conditions such as spinal infections (e.g., epidural abscess, discitis), primary and metastatic spinal tumors, and adult spinal deformities often mandate a posterior surgical approach for decompression, debridement, biopsy, or corrective osteotomies and fusion. The ability to precisely identify and navigate the anatomical structures through a posterior corridor is thus foundational for any surgeon managing complex spinal disorders.
Surgical Anatomy & Biomechanics
A thorough understanding of the three-dimensional anatomy of the lumbar spine is critical for safe and effective posterior surgical intervention. This includes detailed knowledge of the bony architecture, ligamentous complex, muscular layers, and neurovascular elements.
Bony Anatomy
The lumbar spine typically consists of five vertebrae (L1-L5), each characterized by a large, kidney-shaped vertebral body anteriorly, designed for weight-bearing. Posteriorly, the vertebral arch encloses the spinal canal. Key elements of the vertebral arch include:
*
Pedicles:
Short, stout processes extending posteriorly from the vertebral body, forming the lateral walls of the vertebral canal. These structures are crucial for pedicle screw fixation.
*
Laminae:
Flat, broad plates extending posteromedially from the pedicles, meeting in the midline to form the spinous process. Decompression procedures often involve laminectomy or laminotomy.
*
Spinous Process:
A prominent posterior projection providing attachment for ligaments and muscles. Used as a landmark for midline incision and initial dissection.
*
Transverse Processes:
Lateral projections providing attachment for deep back muscles and offering an alternative site for fusion if necessary.
*
Articular Processes (Facets):
Superior and inferior articular processes form synovial facet joints, guiding segmental motion and contributing significantly to spinal stability. The orientation of lumbar facets (sagittal plane dominance) limits rotation but allows for significant flexion/extension. These joints are often targeted in decompression (medial facetectomy) and fusion procedures.

Surgical exposure demonstrating the posterior bony elements, highlighting spinous processes, laminae, and facet joints.
The pars interarticularis is the bony bridge between the superior and inferior articular processes, a common site for stress fractures (spondylolysis) and subsequent spondylolisthesis.
Ligamentous Anatomy
The posterior ligamentous complex provides significant stability and guides segmental motion. Key ligaments include:
*
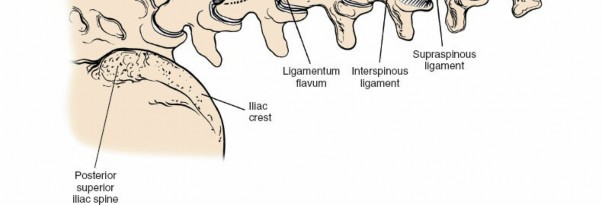
Supraspinous Ligament:
Connects the tips of the spinous processes from C7 to the sacrum.
*
Interspinous Ligament:
Connects adjacent spinous processes, situated anterior to the supraspinous ligament. Both are important for posterior tension band stability.
*
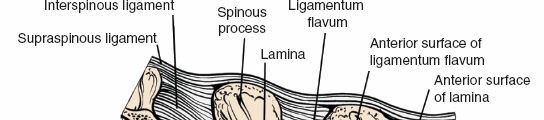
Ligamentum Flavum:
A strong, elastic ligament connecting the laminae of adjacent vertebrae. It forms the posterior border of the spinal canal and its hypertrophy is a common cause of spinal stenosis. Its elastic nature makes it susceptible to buckling during extension.
*
Posterior Longitudinal Ligament (PLL):
Runs along the posterior aspect of the vertebral bodies, within the spinal canal, limiting disc protrusion.
*
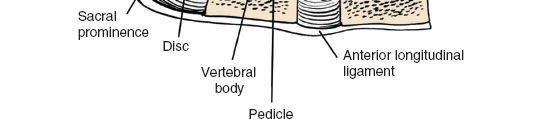
Anterior Longitudinal Ligament (ALL):
Runs along the anterior aspect of the vertebral bodies, limiting extension.

Anatomical illustration depicting the ligamentous structures of the lumbar spine, including the ligamentum flavum and interspinous ligaments.
Muscular Anatomy
The musculature of the posterior spine is layered and provides both dynamic stability and movement. A midline posterior approach requires careful subperiosteal dissection to preserve muscle integrity.
*
Superficial Layer:
Latissimus dorsi and trapezius. These are typically retracted or minimally dissected.
*
Intermediate Layer:
Serratus posterior inferior.
*
Deep Layer (Erector Spinae Group):
The most relevant group.
*
Iliocostalis:
Most lateral, attaching to ribs and transverse processes.
*
Longissimus:
Intermediate, attaching to transverse processes.
*
Multifidus:
The deepest and most medial, directly adjacent to the spinous processes and laminae. It plays a critical role in segmental stability. Preservation of the multifidus, particularly its deep fibers, is associated with improved post-operative outcomes and reduced muscle atrophy.
Demonstration of deep lumbar paraspinal muscles during surgical exposure, specifically highlighting the multifidus muscle.
These muscles are innervated by the dorsal rami of spinal nerves. Subperiosteal dissection helps minimize denervation and muscle damage.

Cross-sectional view illustrating the relationships of the erector spinae muscles to the posterior vertebral elements.
Neurovascular Anatomy
The spinal cord typically terminates as the conus medullaris around the L1-L2 vertebral level in adults, continuing as the cauda equina (horse's tail) below this level. The cauda equina comprises the lumbar, sacral, and coccygeal nerve roots. Each lumbar nerve root exits below its corresponding pedicle (e.g., L4 nerve root exits below the L4 pedicle).
*
Dural Sac:
The tough fibrous membrane enclosing the spinal cord, cauda equina, and cerebrospinal fluid (CSF).
*
Nerve Roots:
Individual nerve roots exit the dural sac, covered by arachnoid and dura, traversing the lateral recess and exiting via the neuroforamen. Awareness of the traversing (superior) and exiting (inferior) nerve roots at each level is crucial during decompression.

Close-up view of the lumbar spinal canal, showing the cauda equina and traversing nerve roots within the dural sac.
Vascular supply to the lumbar spine originates from segmental arteries (lumbar arteries) arising from the aorta. These arteries typically run over the vertebral bodies, supplying the posterior elements via small branches. The venous plexus is extensive, particularly the epidural venous plexus (Baston's plexus), which can cause significant bleeding if not carefully managed during decompression.
Biomechanics
The lumbar spine is engineered for high load-bearing and controlled mobility.
*
Load Bearing:
The vertebral bodies and intervertebral discs bear approximately 80% of axial compressive loads. The posterior elements (facet joints) bear the remaining 20%.
*
Motion:
Lumbar motion primarily occurs in flexion and extension, with limited rotation and lateral bending due to the sagittal orientation of the facet joints and tautness of the posterior ligamentous complex.
*
Stability:
Stability is conferred by the combined action of the bony architecture, strong ligamentous structures, and dynamic muscular control. Injury or degeneration of any of these components can lead to instability.

Sagittal view illustrating the biomechanical interplay of vertebral bodies, discs, and facet joints under axial load.
Surgical interventions, particularly extensive decompression or fusion, alter the inherent biomechanics. Decompression removes bone and ligament, potentially increasing instability. Fusion aims to achieve arthrodesis, eliminating motion at the fused segment, which can transfer stress to adjacent segments, contributing to adjacent segment disease (ASD). The choice of instrumentation (e.g., pedicle screws, interbody cages) aims to restore stability and facilitate fusion in a biomechanically favorable manner.
Indications & Contraindications
The posterior lumbar approach is versatile, indicated for a broad spectrum of spinal pathologies.
Indications
1. Degenerative Conditions:
*
Lumbar Spinal Stenosis:
Central, lateral recess, or foraminal stenosis causing neurogenic claudication or radiculopathy refractory to conservative management. Decompression (laminectomy, laminotomy, foraminotomy) is the primary goal.
*
Lumbar Disc Herniation (LDH):
Radiculopathy unresponsive to non-operative treatment, progressive neurological deficit, or cauda equina syndrome. Microdiscectomy or standard discectomy is performed.
*
Degenerative Spondylolisthesis:
Instability or neurological symptoms associated with forward slip of one vertebra over another. Decompression and instrumented fusion (PLIF/TLIF) are often indicated.
*
Degenerative Disc Disease (DDD):
Chronic axial low back pain with discogenic features, often requiring fusion after conservative failure.

Preoperative MRI (sagittal T2-weighted) demonstrating severe lumbar spinal stenosis at multiple levels.
2. Traumatic Injuries:
*
Unstable Lumbar Fractures:
Fractures involving the posterior column (e.g., Chance fractures, burst fractures with neurological deficit, posterior ligamentous complex disruption) requiring stabilization, decompression, and often fusion.
*
Fracture-Dislocations:
Requiring reduction and rigid fixation.
3. Spinal Deformity:
*
Adult Degenerative Scoliosis/Kyphosis:
Progressive deformity with associated pain, neurological compromise, or functional decline. Posterior instrumentation, corrective osteotomies (e.g., posterior column osteotomy, pedicle subtraction osteotomy), and fusion.
4. Infections:
*
Epidural Abscess:
Surgical drainage and debridement, often requiring laminectomy.
*
Discitis/Osteomyelitis:
Debridement and stabilization, especially in cases of spinal instability or neurological compromise.
5. Neoplastic Conditions:
*
Primary or Metastatic Spinal Tumors:
Decompression of neural elements, tumor biopsy/resection, and stabilization in cases of structural compromise.

Axial CT image demonstrating bone destruction from a metastatic lesion in a lumbar vertebra, potentially requiring posterior stabilization.
Contraindications
Absolute contraindications are rare but include:
*
Active Systemic Infection:
Uncontrolled sepsis, increasing surgical site infection risk.
*
Severe Medical Comorbidities:
Patients unable to tolerate anesthesia or major surgery (e.g., severe cardiopulmonary disease, uncontrolled coagulopathy).
*
Anterior Column Instability Requiring Anterior Support:
For instance, severe burst fractures with significant anterior column compromise without posterior column involvement, which may necessitate an anterior approach for reconstruction.
*
Patient Refusal.
Relative contraindications often involve patient factors that increase risk but may be outweighed by potential benefits:
*
Severe Osteoporosis:
May compromise hardware purchase, necessitating augmentation or alternative strategies.
*
Obesity:
Increased operative time, blood loss, and risk of wound complications.
*
Previous Lumbar Surgery:
May complicate dissection due to scar tissue.
Table: Operative vs. Non-Operative Indications
| Condition | Primary Non-Operative Indications | Primary Operative Indications |
|---|---|---|
| Lumbar Spinal Stenosis | Mild to moderate symptoms, tolerable neurogenic claudication, no neurological deficit, trial of NSAIDs, PT, epidural injections. | Refractory neurogenic claudication, progressive motor weakness, cauda equina syndrome. |
| Lumbar Disc Herniation | Radiculopathy resolving or stable, no progressive deficit, trial of NSAIDs, PT, steroid injections (oral/epidural), watchful waiting (up to 6-12 weeks). | Refractory radiculopathy (>6-12 weeks), progressive motor weakness, cauda equina syndrome, severe intractable pain. |
| Degenerative Spondylolisthesis | Mild symptoms, stable slip, no neurological deficit, PT, core strengthening, epidural injections. | Progressive slip, persistent neurological symptoms (radiculopathy, neurogenic claudication) refractory to conservative care, mechanical low back pain with demonstrated instability. |
| Lumbar Fractures | Stable compression fractures (AO type A1/A2) with intact posterior ligamentous complex, no neurological deficit, appropriate bracing. | Unstable fractures (e.g., burst, Chance, fracture-dislocation), neurological deficit (progressive or severe), significant kyphotic deformity. |
| Spinal Deformity | Mild, non-progressive curves, minimal pain, no neurological compromise, bracing (for adolescents). | Progressive curves, severe pain, neurological deficits, sagittal imbalance, functional decline. |
| Spinal Infection | Localized discitis without neurological compromise, systemic signs controlled with antibiotics, no instability. | Epidural abscess, neurological deficit, spinal instability, extensive bone destruction, refractory infection. |
| Spinal Tumors | Asymptomatic, stable lesions, responsive to radiation/chemotherapy, no impending neurological compromise. | Neurological compromise, spinal instability, intractable pain, progressive tumor growth, biopsy for diagnosis. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and careful patient positioning are crucial for surgical success and minimizing complications.
Pre-Operative Planning
- Clinical Assessment: Thorough history and physical examination, including detailed neurological assessment.
-
Imaging Review:
- MRI: Essential for evaluating neural compression, disc pathology, soft tissue abnormalities, and tumor/infection.
- CT Scan: Provides detailed bony anatomy, crucial for pedicle screw trajectory planning, assessing fracture patterns, facet arthritis, and pars defects.
- Dynamic X-rays: Flexion/extension views to assess segmental stability, particularly in cases of spondylolisthesis.
- Myelography/Post-Myelography CT: Occasionally used when MRI is contraindicated or inconclusive, or for specific anatomical details in complex revision cases.
- Surgical Strategy: Define the levels to be addressed, type of decompression (laminectomy, laminotomy, foraminotomy), need for fusion, type of interbody graft (autograft, allograft, synthetic), and instrumentation (pedicle screws, rods).
- Patient Optimization: Address medical comorbidities (e.g., diabetes, hypertension, cardiac disease), optimize nutritional status, discontinue antiplatelet/anticoagulant medications as per protocol, and administer prophylactic antibiotics.
- Informed Consent: Discuss risks, benefits, alternatives, and potential complications specific to the planned procedure.
Patient Positioning
Proper patient positioning is paramount to facilitate surgical access, optimize physiological parameters, and prevent iatrogenic complications.
1.
Anesthesia Induction:
Performed on the stretcher, followed by careful intubation.
2.
Prone Position:
The patient is carefully turned prone onto a specialized spinal operating table or bolsters.
*
Jackson Table or Wilson Frame:
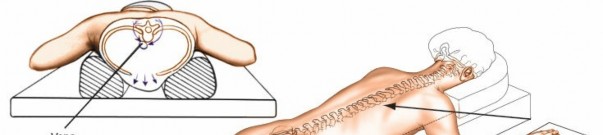
These frames elevate the chest and pelvis, allowing the abdomen to hang freely. This minimizes intra-abdominal pressure, which in turn reduces pressure on the epidural venous plexus, thereby decreasing intraoperative blood loss and improving visualization of the neural structures.
*
Padding:
All pressure points (eyes, ears, shoulders, breasts, iliac crests, knees, dorsum of feet) must be meticulously padded to prevent nerve palsies (e.g., brachial plexus, ulnar nerve, peroneal nerve) and skin breakdown. The eyes should be checked for corneal abrasion.

Illustration depicting a patient in the prone position on a spinal frame, emphasizing proper cushioning and abdominal decompression.
3.
Spinal Alignment:
Ensure the spine is in a neutral or slightly flexed position to maximize interspinous space for easier surgical access and to facilitate reduction of spondylolisthesis if present. Avoid excessive lumbar lordosis.
4.
Neuromonitoring:
Somatosensory evoked potentials (SSEPs), motor evoked potentials (MEPs), and electromyography (EMG) are typically utilized, especially in deformity correction, tumor surgery, or cases with pre-existing neurological deficits. Leads are placed before final draping.
5.
Fluoroscopy:
Ensure adequate anterior-posterior (AP) and lateral fluoroscopic views can be obtained at the targeted spinal levels to confirm appropriate skin incision, verify levels, and guide instrumentation.
Intraoperative lateral fluoroscopic image confirming the correct lumbar vertebral level.
Detailed Surgical Approach / Technique
The posterior lumbar surgical approach involves a series of sequential steps from skin incision to closure, each requiring precision and anatomical awareness.
1. Skin Incision & Initial Dissection
- Level Localization: Using fluoroscopy, identify the correct vertebral level(s) and mark the skin. A needle can be placed at the spinous process to confirm the level on AP and lateral views.
- Incision: A midline skin incision is made directly over the spinous processes of the targeted levels. The length of the incision is dictated by the number of levels involved.
- Subcutaneous Dissection: Dissect through the subcutaneous fat down to the thoracolumbar fascia.
-
Fascial Incision:
Incise the thoracolumbar fascia longitudinally in the midline, directly over the tips of the spinous processes.
Initial surgical incision centered over the lumbar spine, before fascial dissection.
2. Subperiosteal Exposure
- Muscle Stripping: Using subperiosteal elevators (e.g., Cobb elevators), meticulously strip the paraspinal muscles (primarily multifidus and erector spinae) off the spinous processes, laminae, and facet capsules. Begin superiorly and work inferiorly.
- Exposure Extent: For decompression, exposure typically extends laterally to the medial borders of the facet joints. For fusion and instrumentation, the exposure should extend more laterally to the tips of the transverse processes, especially at the L5-S1 junction.
-
Hemostasis:
Meticulous hemostasis is maintained throughout using electrocautery and bipolar cautery, as the paraspinal muscles are highly vascular.

Subperiosteal dissection of paraspinal muscles from the lumbar laminae and spinous processes, exposing the bony architecture. - Interspinous Ligament: The interspinous ligament can be incised or elevated depending on the required exposure.
3. Decompression (Laminectomy/Laminotomy, Foraminotomy, Discectomy)
a. Laminectomy/Laminotomy
- Partial Laminectomy (Laminotomy): Typically performed for contained disc herniations or mild to moderate stenosis. A high-speed burr or Kerrison rongeurs are used to remove a portion of the lamina, preserving the facet joint capsule as much as possible.
- Complete Laminectomy: Required for severe central stenosis, often involving removal of the entire lamina, sometimes extending to the medial aspect of the facet joints. Care must be taken to not destabilize the spine excessively.
- Ligamentum Flavum Resection: After bone removal, the ligamentum flavum, which forms the posterior wall of the spinal canal, is meticulously resected. This is performed carefully, often with a blunt probe or dissecting instrument, to detach it from the dura without causing a dural tear. Kerrison rongeurs are then used to remove the ligament in segments.
b. Foraminotomy
- Performed to decompress the exiting nerve root, typically for foraminal stenosis caused by osteophytes, disc material, or superior articular process hypertrophy.
- This involves removal of bone from the superior aspect of the inferior pedicle and/or the inferior aspect of the superior pedicle, as well as removal of any soft tissue compression (ligamentum flavum, disc herniation).
c. Discectomy (Microdiscectomy)
- Annulotomy: After adequate neural decompression and retraction of the dural sac and nerve root, an annulotomy is performed on the posterolateral annulus fibrosus using a scalpel or pituitary rongeur.
-
Disc Excision:
Pituitary rongeurs are then used to remove extruded or sequestered disc fragments and a portion of the degenerated nucleus pulposus. The goal is to remove compressive elements and avoid extensive curettage that might promote segmental instability.

Intraoperative view during lumbar microdiscectomy, showing the retracted nerve root, incised annulus, and disc material being removed.
4. Spinal Fusion & Instrumentation (if indicated)
If instability is present, or anticipated following extensive decompression, fusion and instrumentation are performed. This typically involves pedicle screw fixation.
a. Pedicle Screw Placement
- Entry Point: Critical for accurate screw trajectory. Typically, at the junction of the transverse process, the superior articular process, and the pars interarticularis. Specific entry points vary slightly by level and anatomical variations.
- Pilot Hole: An awl or burr creates a starting point.
- Pedicle Probe/Ball-tip Probe: A pedicle probe is used to create a channel down the pedicle, ensuring cortical containment. This is then "sounded" with a ball-tip probe in all five directions (medial, lateral, superior, inferior, anterior) to confirm cortical integrity and absence of breaches.
- Tapping: The pedicle is tapped to create threads, matching the screw diameter.
-
Screw Insertion:
Pedicle screws are then inserted, often with image guidance (fluoroscopy, navigation) to ensure optimal placement. The screw length and diameter are chosen based on patient anatomy and bone quality.

Anatomical depiction of the optimal pedicle screw entry point and trajectory within a lumbar vertebra.

Intraoperative image demonstrating pedicle screw insertion, highlighting careful hand position and screw alignment. - Reduction/Contouring: If spondylolisthesis is present, reduction maneuvers are performed using the pedicle screws and rods. The rods are contoured to restore physiological lordosis.
b. Fusion Bed Preparation
- Decortication: The posterior elements (lamina, facet joints, transverse processes) are decorticated using a burr or osteotome to expose cancellous bone, promoting bleeding and enhancing bone graft incorporation.
- Bone Grafting: Autograft (local bone from laminectomy, iliac crest), allograft, or synthetic bone graft substitutes are placed over the decorticated surfaces (posterolateral fusion).
-
Interbody Fusion (PLIF/TLIF):
- Posterior Lumbar Interbody Fusion (PLIF): Involves bilateral removal of posterior disc material and insertion of two interbody cages (filled with bone graft) into the disc space after distracting the vertebral bodies. This provides anterior column support.
-
Transforaminal Lumbar Interbody Fusion (TLIF):
A unilateral approach, removing a portion of the facet joint and lateral annulus to access the disc space. A single, larger interbody cage is inserted obliquely into the disc space. This is often preferred due to less neural retraction and potentially reduced risk of dural injury compared to PLIF.

Surgical view during a TLIF procedure, showing nerve root retraction and preparation of the disc space for interbody cage insertion.

Lateral fluoroscopic image demonstrating the placement of an interbody cage within the disc space and pedicle screws during a lumbar fusion.
5. Final Checks & Closure
- Neural Decompression: Ensure complete and adequate decompression of all neural elements.
- Hemostasis: Achieve meticulous hemostasis.
- Hardware Check: Confirm all screws are secure, rods are properly seated, and locking caps are tightened.
- Drain Placement: A closed suction drain may be placed in the surgical bed to prevent hematoma formation, especially in extensive procedures.
-
Layered Closure:
- Fascia: Close the thoracolumbar fascia using strong, absorbable sutures. This layer is crucial for preventing seroma and muscle herniation.
- Subcutaneous Tissue: Close with interrupted absorbable sutures to obliterate dead space.
-
Skin:
Close with staples or absorbable/non-absorbable sutures.

Final intraoperative image showing the wound closure with skin staples after a posterior lumbar surgical procedure.
Complications & Management
Despite advancements, lumbar spine surgery carries inherent risks. A thorough understanding of potential complications and their management is essential.
General Surgical Complications
-
Infection:
Superficial or deep surgical site infection (SSI). Incidence varies from 0.7-5%.
- Management: Prophylactic antibiotics, meticulous sterile technique, wound irrigation, debridement, targeted antibiotics.
-
Bleeding/Hematoma:
Can lead to epidural hematoma and neurological compromise.
- Management: Meticulous hemostasis, intraoperative cell salvage, transfusion, post-operative drain, consider re-exploration for expanding hematoma with neurological deficit.
-
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
- Management: Mechanical prophylaxis (compression stockings, SCDs), early ambulation, chemical prophylaxis in high-risk patients.
-
Anesthetic Complications:
Related to patient comorbidities and intubation.
- Management: Pre-operative optimization, skilled anesthesia care, vigilant monitoring.
Spine-Specific Complications
-
Dural Tear / Cerebrospinal Fluid (CSF) Leak:
Incidence ranges from 1-17%, higher in revision surgery. Can lead to persistent headache, pseudomeningocele, or meningitis.
- Management: Primary repair (suture), patch grafts (fascia, fat, allograft), fibrin glue, muscle/fat graft over repair, bed rest, head of bed flat, sometimes lumbar drain.
-
Nerve Root Injury / Neurological Deficit:
Can result from direct trauma, excessive retraction, thermal injury, or malpositioned hardware. Incidence 0.1-2%.
- Management: Intraoperative neuromonitoring, careful dissection, removal of offending hardware/bone, post-operative imaging (MRI/CT) to rule out compression.
-
Hardware Malposition / Failure:
Pedicle screw malposition can lead to nerve root irritation, vascular injury, or decreased stability. Screw pullout or rod breakage can lead to pseudarthrosis.
- Management: Intraoperative fluoroscopy/navigation, post-operative imaging. Revision surgery if symptomatic or compromising fusion.
-
Pseudarthrosis (Non-Union):
Failure of bone fusion. Incidence 5-20% depending on patient factors and levels fused.
- Management: Symptomatic treatment, bracing, electrical stimulation. Revision surgery with additional grafting, improved fixation, or alternative fusion techniques.
-
Adjacent Segment Disease (ASD):
Degeneration at levels adjacent to a fusion. Symptomatic ASD requiring surgery occurs in 2-5% per year post-fusion.
- Management: Conservative treatment for mild symptoms. Decompression or extension of fusion for refractory symptoms or neurological deficit.
-
Vascular Injury:
Major vessel injury (aorta, iliac vessels) is rare but catastrophic, often related to anterior pedicle breach or disc space violation during interbody fusion.
- Management: Immediate surgical repair (vascular surgeon consultation), often requiring an anterior approach.
-
Ureteral Injury:
Rare, usually associated with L5-S1 anterior pedicle breach or aggressive dissection during anterior approaches, but possible with very lateral screw trajectories.
- Management: Urological consultation, stent placement or repair.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Typical Incidence (%) | Salvage Strategies |
|---|---|---|
| Dural Tear / CSF Leak | 1-17 | Primary suture repair, fascial/fat graft, fibrin glue, lumbar drain, bed rest. |
| Nerve Root Injury | 0.1-2 | Removal of compressive elements (hematoma, hardware), neurolysis, medication for neuropathic pain, observation. |
| Surgical Site Infection (SSI) | 0.7-5 | Targeted antibiotics, wound debridement, hardware retention vs. removal (depending on depth/severity). |
| Hardware Malposition/Failure | 1-5 | Revision surgery for symptomatic malposition, repositioning/removal, revision fixation, augmentation. |
| Pseudarthrosis (Non-Union) | 5-20 | Conservative management, revision fusion with stronger fixation/grafting, bone stimulators. |
| Adjacent Segment Disease (ASD) | 2-5/year | Conservative management, decompression, or extension of fusion. |
| Epidural Hematoma | <1 | Urgent surgical evacuation, decompression. |
| Major Vascular Injury | Rare (<0.1) | Immediate vascular surgical consultation and repair. |
| Transient Neurological Deficit | 2-10 | Observation, supportive care, physical therapy. |
| Post-Op Pain (Persistent) | Variable | Multi-modal analgesia, physical therapy, pain clinic referral, psychological support. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is integral to optimizing functional recovery, restoring strength, and preventing recurrence or secondary complications. Protocols vary based on the procedure performed (decompression vs. fusion), patient age, and overall health status.
1. Immediate Post-Operative Phase (Days 0-7)
- Pain Management: Aggressive multi-modal analgesia (opioids, NSAIDs, acetaminophen, muscle relaxants, gabapentinoids) to facilitate early mobilization.
-
Mobilization:
- Day 0-1: Out of bed with assistance, standing, short walks. Emphasis on log-rolling technique to minimize spinal torsion.
- Day 1-7: Progressive ambulation, increasing distance and frequency. Avoid prolonged sitting.
- Activity Restrictions: Avoid bending, lifting (heavy objects), twisting (BLT precautions). No strenuous activity.
- Wound Care: Monitor for signs of infection or hematoma. Dressing changes as per protocol.
- Bracing: Typically not required for single-level decompressions or uncomplicated fusions. May be used for multi-level fusions, significant instability, or in patients with poor bone quality to provide external support.
- DVT Prophylaxis: Continue mechanical prophylaxis (SCDs) and consider chemical prophylaxis as appropriate.
2. Early Rehabilitation Phase (Weeks 2-6)
-
Physical Therapy (PT):
Initiate a structured PT program focused on:
- Core Stability: Gentle core strengthening exercises (e.g., pelvic tilts, gentle abdominal bracing) to improve spinal support.
- Flexibility: Gentle range of motion exercises, avoiding extremes of motion, especially flexion and twisting.
- Gait Training: Improve walking mechanics and endurance.
- Activity Progression: Gradual increase in ambulation. Light household activities. Continued adherence to BLT precautions.
- Education: Reinforce proper body mechanics, posture, and strategies for daily activities.
3. Intermediate Rehabilitation Phase (Weeks 6-12)
- Advanced PT: Progress to more intensive core and paraspinal muscle strengthening. Introduction of proprioceptive and balance exercises.
- Cardiovascular Conditioning: Stationary cycling, swimming (once wound is healed), elliptical training.
- Activity Progression: Gradual return to light work activities, driving (if cleared by surgeon). Lifting restrictions gradually eased, often with a limit of 5-10 lbs.
- Fusion Assessment: For fusion patients, radiographic assessment (X-rays, sometimes CT) may be performed around 3 months to assess early signs of fusion.
4. Late Rehabilitation Phase (Months 3-6+)
- Functional Training: Focus on sport-specific or work-specific activities. High-level strengthening and conditioning.
- Impact Activities: Gradually introduce low-impact activities, progressing to higher impact as tolerated and if clinically appropriate, with surgeon approval.
- Return to Work/Sport: Gradual return based on job demands and patient's recovery, with appropriate restrictions. Full return to strenuous activities typically 6-12 months post-fusion, contingent on radiographic evidence of solid fusion.
- Long-term Maintenance: Lifelong commitment to core strengthening, maintaining flexibility, and proper body mechanics to prevent recurrence and promote spinal health.
The progression through these phases is individualized, guided by patient symptoms, functional status, and radiographic findings. Communication between the surgeon, physical therapist, and patient is paramount for a successful outcome.
Summary of Key Literature / Guidelines
The evidence base supporting posterior lumbar surgery is extensive, with ongoing research refining indications, techniques, and outcomes. Several landmark studies and guidelines inform contemporary practice.
-
SPORT Trial (Spine Patient Outcomes Research Trial): A multi-center randomized controlled trial comparing surgical and non-surgical treatments for various lumbar pathologies (disc herniation, spinal stenosis, spondylolisthesis).
- Disc Herniation: Demonstrated significantly greater improvement in pain and function with surgery compared to non-operative treatment for patients with symptomatic lumbar disc herniation who failed conservative care, especially those who crossed over to surgery.
- Spinal Stenosis: Found that surgical decompression resulted in significantly greater improvement in pain and function compared to non-operative treatment in patients with symptomatic lumbar spinal stenosis, with benefits sustained over several years.
- Spondylolisthesis: Showed that decompression with fusion provided superior outcomes compared to decompression alone for degenerative spondylolisthesis with associated instability.
- Conclusion: The SPORT trial provided strong evidence for the efficacy of surgical intervention in carefully selected patients with lumbar degenerative conditions.
-
Fusion vs. Decompression Alone for Degenerative Spondylolisthesis: Multiple studies and meta-analyses have largely concluded that instrumented fusion combined with decompression provides superior long-term stability and pain relief compared to decompression alone for symptomatic degenerative spondylolisthesis, particularly for grades I and II with mechanical instability or significant radicular symptoms. The benefits often outweigh the increased risks of fusion surgery in this specific patient population.
-
Minimally Invasive Spine Surgery (MISS): Techniques such as tubular microdiscectomy, minimally invasive TLIF (MI-TLIF), and percutaneous pedicle screw fixation have gained prominence. Literature suggests that MISS can achieve comparable clinical outcomes to open techniques, with potential benefits including reduced blood loss, shorter hospital stays, less post-operative pain, and faster recovery, particularly in skilled hands. However, it typically has a steeper learning curve and may not be suitable for all complex pathologies.
-
Evidence for Lumbar Fusion in Chronic Low Back Pain: The role of fusion for purely discogenic low back pain without instability remains controversial. While some patients benefit, the outcomes are less predictable than for radicular pain or instability. Strict patient selection, psychological evaluation, and failure of comprehensive non-operative management are critical.
-
Guidelines: Organizations like the North American Spine Society (NASS), AOSpine, and the American Academy of Orthopaedic Surgeons (AAOS) regularly publish evidence-based clinical practice guidelines that help standardize indications, diagnostic criteria, and treatment recommendations for various lumbar spinal pathologies. These guidelines are crucial for informing evidence-based practice and improving patient care.
In conclusion, the posterior approach to the lumbar spine remains a critical and effective surgical modality for a wide range of debilitating conditions. Continued mastery of applied anatomy, rigorous surgical technique, and adherence to evidence-based guidelines are essential for optimal patient outcomes in this complex field.
You Might Also Like