Posterior Glenohumeral Dislocation: Epidemiology, Anatomy, Diagnosis & Management
Key Takeaway
Posterior glenohumeral dislocation (PGHD) is an uncommon shoulder injury, often misdiagnosed, accounting for 2-5% of dislocations. It's classically linked to high-energy muscle contractions from epileptic seizures or electric shock. Key features include a reverse Hill-Sachs lesion (humeral head impaction) and potentially a reverse Bankart lesion (posterior labral tear), requiring prompt diagnosis and tailored management.
Introduction & Epidemiology
Posterior glenohumeral dislocation (PGHD) is a relatively uncommon injury, accounting for only 2-5% of all shoulder dislocations, significantly less frequent than anterior dislocations. Despite its lower incidence, it is often misdiagnosed or diagnosed late, with up to 50% of acute posterior dislocations missed on initial presentation, leading to increased morbidity and complex treatment challenges. The delay in diagnosis is largely attributable to the subtle clinical presentation and often misinterpreted conventional radiographs.
The typical mechanism of injury involves indirect trauma, classically associated with high-energy muscle contractions such as those occurring during epileptic seizures, electroconvulsion therapy, or electrical shock . Direct trauma to the anterior aspect of the shoulder, leading to posterior displacement of the humeral head, can also cause this injury, particularly in high-impact sports or motor vehicle accidents. Other less common causes include falls, assaults, or iatrogenic injuries during surgical procedures. PGHD can be unilateral or bilateral, with bilateral dislocations almost pathognomonic for seizure activity or electrocution.
Acute diagnosis and prompt reduction are paramount to minimize complications such as avascular necrosis (AVN) of the humeral head, recurrent instability, chronic pain, and debilitating functional limitations. The recognition of specific radiographic signs and a high index of clinical suspicion are critical for timely intervention.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the glenohumeral joint is essential for addressing posterior shoulder dislocations. The glenohumeral joint is inherently unstable, relying heavily on dynamic stabilizers (rotator cuff muscles) and static stabilizers (capsuloligamentous structures, glenoid labrum, negative intra-articular pressure) for its stability.
Static Stabilizers
- Glenoid Labrum : The fibrocartilaginous rim deepens the glenoid fossa, increasing its articular surface area and providing an attachment point for the joint capsule and glenohumeral ligaments. A reverse Bankart lesion , an avulsion of the posterior labrum and periosteum from the posterior glenoid rim, is a common finding in PGHD.
- Glenohumeral Ligaments : The superior, middle, and inferior glenohumeral ligaments reinforce the joint capsule. The posterior band of the inferior glenohumeral ligament (PIGHL) and the posterior capsule are the primary static stabilizers resisting posterior translation of the humeral head, especially in internal rotation and adduction.
- Glenoid Retroversion : The glenoid typically has slight retroversion (0-7 degrees). Excessive glenoid retroversion can predispose to posterior instability.
Dynamic Stabilizers
-
Rotator Cuff Muscles
:
- Subscapularis : The largest and most powerful rotator cuff muscle, primarily responsible for internal rotation and anterior stability. In posterior dislocations, the subscapularis and pectoralis major often remain unopposed, pulling the humerus into internal rotation.
- Infraspinatus and Teres Minor : These muscles primarily externally rotate the humerus and contribute significantly to posterior and inferior stability by compressing the humeral head into the glenoid. In PGHD, severe internal rotation often leads to a mechanical block due to the humeral head impacting the posterior glenoid rim, preventing external rotation.
Osseous Structures
- Humeral Head : The articular surface of the humeral head can sustain an impaction fracture on its anteromedial aspect when forcefully driven against the posterior glenoid rim. This lesion is termed a reverse Hill-Sachs lesion (or McLaughlin lesion) and is a hallmark of posterior dislocations. Its size and location are critical determinants of joint stability and reducibility.
- Glenoid Fossa : Fractures of the posterior glenoid rim can occur, either as part of a reverse Bankart lesion or as a larger posterior bony glenoid defect. The size of this defect impacts stability and often necessitates surgical reconstruction.
The pathomechanics of PGHD typically involves a force that drives the humeral head posteriorly while the arm is in an adducted, internally rotated, and often flexed position. This can lead to the humeral head becoming locked in internal rotation behind the posterior glenoid rim, creating the characteristic clinical and radiographic presentation.
Indications & Contraindications
The decision-making process for managing posterior glenohumeral dislocations is complex, depending on several factors including the duration of dislocation (acute vs. chronic), the presence and size of associated osseous defects (reverse Hill-Sachs, reverse Bankart/glenoid rim fracture), patient age, functional demands, and overall medical status.
Non-Operative Indications
Closed reduction is the initial treatment of choice for acute posterior dislocations, especially those without significant associated bony lesions.
*
Acute Dislocation
: Within 3 weeks of injury.
*
Reducible Dislocation
: Manual reduction under adequate sedation and muscle relaxation can successfully restore joint congruity.
*
Minimal Osseous Defects
: Reverse Hill-Sachs lesion involving less than 20-25% of the articular surface.
*
Stable Post-Reduction
: The joint remains concentrically reduced with a full range of motion, particularly external rotation.
*
First-time Dislocation
: Without significant underlying instability.
Operative Indications
Surgical intervention is indicated for dislocations that are irreducible, chronic, associated with significant bony defects, or result in recurrent instability after closed reduction.
*
Irreducible Acute Dislocation
: Mechanical block preventing closed reduction (e.g., incarcerated posterior labrum, displaced glenoid fracture, or large reverse Hill-Sachs lesion engaging the glenoid).
*
Chronic Dislocation
: Dislocations present for more than 3 weeks, where soft tissue contractures and adhesions make closed reduction difficult and risky, increasing the risk of AVN or iatrogenic fracture.
*
Significant Reverse Hill-Sachs Lesion
: Typically involving >25-40% of the articular surface, leading to persistent instability or recurrent dislocations.
*
Significant Posterior Glenoid Rim Fracture (Reverse Bankart)
: Defects involving >25% of the glenoid width, contributing to instability.
*
Failed Closed Reduction
: Recurrent instability despite appropriate post-reduction immobilization and rehabilitation.
*
Associated Injuries
: Concomitant rotator cuff tears that require surgical repair, or neurological deficits not resolving after reduction.
Contraindications
While few absolute contraindications exist for treating PGHD, certain conditions may influence the timing, method, or feasibility of treatment.
*
Unstable Patient
: Severe medical comorbidities that preclude general anesthesia or prolonged surgical procedures.
*
Local Infection
: Active infection in the shoulder region.
*
Severe Comminution
: Irreparable damage to the humeral head or glenoid, potentially necessitating arthroplasty as a primary treatment.
*
Extensive Soft Tissue Damage
: Compromised soft tissue envelope preventing a safe surgical approach.
Summary of Operative vs. Non-Operative Indications
| Feature / Indication | Non-Operative Management | Operative Management |
|---|---|---|
| Duration of Dislocation | Acute (<3 weeks) | Chronic (>3 weeks); Irreducible acute |
| Reducibility | Successfully reducible via closed technique | Irreducible by closed means |
| Reverse Hill-Sachs Lesion | <20-25% of articular surface | >25-40% of articular surface; engaging lesion |
| Posterior Glenoid Defect | Minimal or no significant defect | >25% of glenoid width or displaced fracture |
| Post-Reduction Stability | Stable with full ROM | Unstable (re-dislocates) or restricted ROM |
| Associated Injuries | No significant associated soft tissue or bony injuries | Rotator cuff tears requiring repair; significant nerve injury |
| Patient Factors | Young, compliant, low demand, first-time dislocation | High demand, recurrent instability, failed non-operative Rx |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is crucial for successful management of posterior shoulder dislocations, especially given the propensity for missed diagnoses and associated complex pathology.
Diagnosis & Imaging
- Clinical Examination : Patients typically present with the affected arm held in adduction and internal rotation , often unable to externally rotate or abduct. The shoulder may appear flattened anteriorly and a prominence may be palpable posteriorly. Pain is significant. Assessment of neurovascular status (especially axillary nerve) is mandatory.
-
Radiographs
:
-
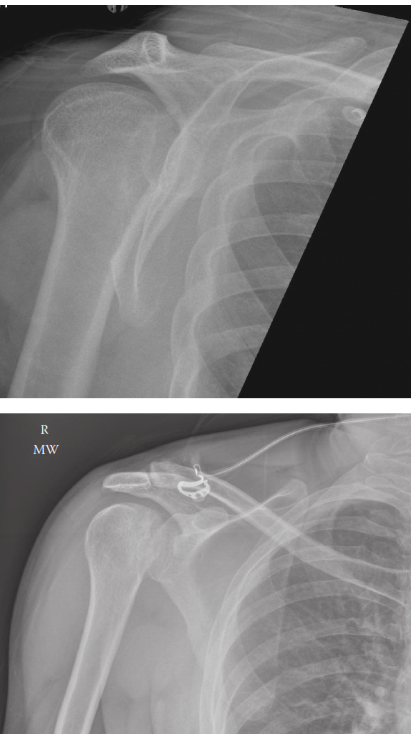
Anteroposterior (AP) View
: Often the most misleading. The humeral head appears round or "lightbulb-shaped" due to its fixed internal rotation, making it difficult to discern the normal glenoid-humeral overlap. The "trough line" or "double rim sign" may be visible, representing the impaction fracture (reverse Hill-Sachs) on the anteromedial humeral head.
Illustration of the "Lightbulb Sign" on an AP radiograph, demonstrating the fixed internal rotation of the humeral head. - Scapular Y-View : The humeral head will be positioned posterior to the glenoid, providing a clearer indication of posterior displacement.
- Axillary View (or Velpeau View, West Point View) : This is the most diagnostic view, directly visualizing the posterior displacement of the humeral head relative to the glenoid. However, it can be painful and difficult to obtain in acute, painful settings.
-
Anteroposterior (AP) View
: Often the most misleading. The humeral head appears round or "lightbulb-shaped" due to its fixed internal rotation, making it difficult to discern the normal glenoid-humeral overlap. The "trough line" or "double rim sign" may be visible, representing the impaction fracture (reverse Hill-Sachs) on the anteromedial humeral head.
-
Computed Tomography (CT) Scan
: Essential for detailed assessment of chronic or complex dislocations. It accurately delineates the size and location of osseous defects:
- Reverse Hill-Sachs Lesion : Quantifies the percentage of articular surface involved. Crucial for surgical planning (e.g., if a bone graft or remplissage procedure is needed).
- Posterior Glenoid Bone Loss (Reverse Bankart Lesion) : Measures the extent of the posterior glenoid rim fracture, guiding decisions on labral repair versus glenoid augmentation.
- Joint Congruity and Chronicity : Confirms the direction of dislocation and identifies any intervening soft tissue blocks.
- Magnetic Resonance Imaging (MRI) : Useful for evaluating soft tissue injuries, such as rotator cuff tears, labral pathology, and capsular integrity, though less critical for initial diagnosis of dislocation.
Pre-Operative Considerations
- Anesthesia : General anesthesia with muscle relaxation is typically required for both closed and open reductions due to significant pain and muscle guarding.
- Informed Consent : Discussion of risks, benefits, alternatives, and potential complications including AVN, recurrence, stiffness, and nerve injury.
- Equipment : Appropriate instrumentation for arthroscopy, open reduction, bone grafting, and internal fixation (suture anchors, screws, plates). Fluoroscopy may be beneficial for confirming reduction.
Patient Positioning
-
Closed Reduction
:
- Supine Position : The patient is supine on the operating table. The affected arm is free-draped. Adequate padding for pressure points.
-
Open Reduction/Stabilization
:
- Beach Chair Position : Common for anterior approaches (deltopectoral), allowing good access to the anterior aspect of the shoulder. The patient is semi-recumbent with the head secured. The arm is free-draped.
- Lateral Decubitus Position : Less common for posterior dislocations unless a specific posterior approach is planned, or for concurrent arthroscopic procedures. The patient is placed on their side with the affected arm elevated or suspended in traction.
Detailed Surgical Approach / Technique
The surgical technique depends heavily on the chronicity of the dislocation, reducibility, and the presence and size of associated bony defects.
A. Closed Reduction (Acute Dislocations)
This is the primary treatment for acute, reducible posterior dislocations and should be attempted first.
1.
Anesthesia
: Adequate intravenous analgesia and sedation are critical, often requiring procedural sedation or general anesthesia to achieve complete muscle relaxation.
2.
Traction-Countertraction
: The patient is supine. An assistant provides countertraction on the ipsilateral axilla or torso. The surgeon applies gentle, sustained inline traction to the arm, in the direction of the deformity (adducted, internally rotated, slightly flexed).
3.
Specific Maneuvers
:
*
External Rotation and Forward Flexion
: While maintaining traction, slowly and gently bring the arm into slight abduction and progressive external rotation. Some recommend gradual forward flexion to approximately 90 degrees.
*
Leverage
: Once sufficient muscle relaxation is achieved, a gentle posterior-to-anterior force can be applied to the humeral head, often by placing the opposite hand in the axilla, while the traction force is maintained. The reduction is often felt as a palpable clunk.
*
Hippocratic Maneuver (Modified)
: Not recommended due to axillary nerve injury risk, but variants using a sheet in the axilla for countertraction are safer.
4.
Post-Reduction Assessment
:
*
Clinical
: Check for restoration of normal range of motion, particularly external rotation. Assess neurovascular status.
*
Radiographic
: Immediate post-reduction radiographs (AP, Y, and Axillary views) are mandatory to confirm concentric reduction and rule out iatrogenic fractures.
*
Stability
: Assess stability in various positions, especially internal rotation and adduction. If unstable, consider immobilization in slight external rotation and abduction.
B. Open Reduction and Internal Fixation (Chronic or Irreducible Dislocations)
Open reduction is indicated for failed closed reduction, chronic dislocations, or those with significant bony lesions.
1. Surgical Approach
-
Deltopectoral Approach (Anterior Approach)
: This is the most common approach for both reduction and addressing anterior-medial humeral head defects (reverse Hill-Sachs) or posterior glenoid defects.
- Incision : A curvilinear incision is made from the coracoid process inferiorly along the deltopectoral groove for approximately 8-10 cm.
- Interval : The deltopectoral interval is identified between the deltoid and pectoralis major muscles. The cephalic vein is identified and retracted laterally with the deltoid.
- Conjoint Tendon : The conjoint tendon (coracobrachialis and short head of biceps) is identified and retracted medially, protecting the musculocutaneous nerve.
- Subscapularis : The subscapularis tendon is exposed. For reduction, a subscapularis split or tenotomy (repaired later) may be performed to allow access to the joint and facilitate reduction. In chronic cases, the subscapularis may be severely contracted and require careful release.
- Capsulotomy : An anterior capsulotomy is performed to gain access to the humeral head.
2. Reduction Technique (Open)
- Once the joint is exposed, the humeral head is visualized. It is often entrapped posteriorly by the glenoid rim.
- Gentle traction, manipulation, and levering using a blunt instrument (e.g., periosteal elevator or specific humeral head retractors) are used to disengage the humeral head from the posterior glenoid and bring it back into the glenoid fossa.
- Care must be taken to avoid further damage to the articular cartilage or neurovascular structures.
- Once reduced, assess stability through a range of motion.
3. Addressing Associated Lesions
-
Reverse Hill-Sachs Lesion (Anteromedial Humeral Head Impaction Fracture) :
- Small (non-engaging, <20-25%) : Often managed conservatively after reduction.
-
Moderate (25-40%, engaging)
:
- Remplissage (Medialization of Infraspinatus/Posterior Capsule) : If the defect is on the anteromedial aspect, an open or arthroscopic remplissage can be performed. The infraspinatus tendon and posterior capsule are tenodesed into the defect with suture anchors. This effectively fills the defect and prevents it from engaging the glenoid rim, while also tightening the posterior capsule.
- Bone Grafting : For larger defects, a structural autograft (e.g., iliac crest) or allograft can be placed into the defect and secured with headless screws or bioabsorbable pins to restore the articular contour. This is technically demanding and less common than remplissage for moderate defects.
-
Large (>40%, unstable)
:
- Allograft/Autograft Reconstruction : Large structural grafts (e.g., femoral head allograft, iliac crest autograft) are typically required to reconstruct the humeral head articular surface.
- Rotational Humeral Osteotomy : Rarely used, typically for very large defects in younger patients to reorient the articular surface.
- Arthroplasty (Hemiarthroplasty or Total Shoulder Arthroplasty) : For chronic dislocations with significant humeral head destruction or avascular necrosis, especially in older, low-demand patients, arthroplasty may be the only viable option.
-
Posterior Glenoid Bone Loss (Reverse Bankart Lesion) :
- Repair : For avulsions of the posterior labrum with minimal bone loss, the labrum and capsule are reattached to the posterior glenoid rim using suture anchors (arthroscopic or open).
- Bone Block Augmentation : For significant bony defects of the posterior glenoid (>25% of glenoid width), an autogenous bone block (e.g., iliac crest) or allograft can be harvested and secured to the posterior glenoid rim to restore the glenoid arc and prevent recurrent posterior instability. Techniques include open Latarjet-type procedures adapted for posterior glenoid or tricortical iliac crest grafts.
4. Capsular Repair/Plication
After addressing osseous lesions and ensuring reduction, the posterior capsule may be plicated or tightened to enhance stability, particularly if laxity is noted. The subscapularis tendon is then repaired if it was released.
5. Wound Closure
Routine layered closure. The arm is typically immobilized in a sling, often with a specific brace that holds the arm in slight external rotation and abduction to protect the repair and prevent re-dislocation.
Complications & Management
Posterior glenohumeral dislocations, especially when chronic or associated with significant bone loss, carry a high risk of complications. Vigilance and prompt management are critical.
| Complication | Incidence | Salvage Strategies / Management |
|---|---|---|
| Avascular Necrosis (AVN) of Humeral Head | 5-40% (higher in chronic dislocations, esp. >6 weeks) | Prevention by prompt, gentle reduction. If symptomatic and progressive: core decompression (early stages), humeral head resurfacing, hemiarthroplasty, or total shoulder arthroplasty (for advanced stages or elderly). |
| Recurrent Instability / Dislocation | 10-30% (variable depending on associated lesions) | Identification and addressing underlying pathology: Remplissage for engaging reverse Hill-Sachs, bone grafting for large reverse Hill-Sachs or glenoid defects, capsular plication , revision labral repair. Consider open stabilization for failed arthroscopic. |
| Stiffness / Loss of Range of Motion (ROM) | Common, especially after prolonged immobilization or chronic dislocation | Aggressive, structured physiotherapy with close monitoring. For persistent, recalcitrant stiffness: manipulation under anesthesia (MUA), arthroscopic capsular release. Prevention includes early, protected motion. |
| Nerve Injury (Axillary Nerve Most Common) | <5% (can be higher with traction injuries or iatrogenic during surgery) | Observation and supportive care for neuropraxia. EMG/NCS for diagnosis and follow-up. Surgical exploration and repair/grafting for complete transection or non-recovering deficits after 3-6 months. |
| Rotator Cuff Tear | 10-20% (often subscapularis) | Acute repair if diagnosed and indicated (large, symptomatic). If chronic and symptomatic: surgical repair, débridement, or management based on tear pattern and patient factors. |
| Infection (Superficial/Deep) | <1% | Superficial: wound care, oral antibiotics. Deep: surgical débridement, irrigation, retention/exchange of hardware (if present), prolonged intravenous antibiotics, potentially removal of implants and re-implantation. |
| Hardware-related Issues | Variable (e.g., screw loosening, anchor pull-out) | Symptomatic hardware may require removal. Revision surgery for anchor pull-out with re-repair. |
| Pain (Chronic) | Variable | Multimodal pain management, physical therapy. Identification and treatment of residual instability, stiffness, or degenerative changes. Psychological support. |
| Iatrogenic Fracture | Rare (during reduction attempt or hardware insertion) | Management depends on fracture type and location; may require internal fixation, revision surgery, or further immobilization. |
| Degenerative Arthritis | Long-term complication, especially with chronic dislocations or large bone defects | Conservative management (NSAIDs, injections, PT) in early stages. Arthroscopy for débridement in select cases. Arthroplasty (hemiarthroplasty or TSA) for end-stage arthritis with significant pain and dysfunction. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful outcomes following reduction and/or surgical stabilization of posterior glenohumeral dislocations. Protocols are typically phased and individualized based on the specific surgical procedure, quality of fixation, and patient factors. The primary goals are to protect the repair, restore range of motion, regain strength, and facilitate a safe return to activity.
Phase I: Protection & Early Motion (Weeks 0-6)
- Immobilization : Sling for 4-6 weeks, often in a position of slight external rotation (0-15 degrees) and 10-20 degrees abduction, to prevent re-dislocation, especially for defects requiring remplissage or posterior stabilization. Strict avoidance of internal rotation and adduction combined with forward flexion.
- Pain & Edema Management : Cryotherapy, NSAIDs, analgesics.
-
Passive Range of Motion (PROM)
:
- Pendulum exercises : Gentle, gravity-assisted movements.
- Scapular stabilization exercises : Begin early to maintain mobility and activate periscapular muscles.
- Assisted ROM : External rotation (limited to 0-15 degrees), abduction (limited to 45-60 degrees), forward flexion (limited to 90 degrees). Strict avoidance of internal rotation past neutral and combined adduction/forward flexion.
- Goals : Control pain, protect repair, prevent stiffness, initiate early muscle activation.
Phase II: Gradual Restoration of Motion & Early Strengthening (Weeks 6-12)
- Discontinue Sling : Gradually wean off sling, allowing use for activities of daily living (ADLs) as tolerated.
-
Active-Assisted Range of Motion (AAROM) & Active Range of Motion (AROM)
:
- Progress to full passive and active-assisted ROM.
- Gradually increase active ROM, always respecting pain and tissue healing.
- Continue to limit combined internal rotation, adduction, and forward flexion, particularly if a posterior stabilization was performed.
-
Isometrics
:
- Gentle isometric exercises for rotator cuff and deltoid muscles, starting in neutral positions.
- Avoid resisted internal rotation and adduction in the early stages if a posterior repair or remplissage was performed.
- Scapular Strengthening : Continue and advance exercises for scapular retractors and stabilizers (rhomboids, middle/lower trapezius, serratus anterior).
- Goals : Achieve functional AROM, begin gentle strengthening, improve neuromuscular control.
Phase III: Progressive Strengthening & Advanced Mobility (Weeks 12-24)
- Full Range of Motion : Aim for near-normal, pain-free ROM in all planes.
-
Progressive Resistance Exercises (PREs)
:
- Introduce light resistance for rotator cuff (internal/external rotation with resistance bands) and deltoid muscles.
- Progress open and closed kinetic chain exercises.
- Focus on eccentric strengthening.
-
Proprioception & Neuromuscular Control
:
- Balance and coordination drills (e.g., using a stability ball or wobble board).
- Dynamic stabilization exercises.
- Functional Training : Begin incorporating sport-specific or work-specific movements.
- Goals : Maximize strength, power, endurance, and proprioception.
Phase IV: Return to Activity (Months 6+)
- Advanced Strengthening : Continue strengthening with increased resistance and intensity.
- Plyometrics & Agility : For athletes, introduce sport-specific plyometric and agility drills under controlled conditions.
-
Gradual Return to Sport/Work
:
- Phased return, initially with modified activities, then progressing to full participation.
- Emphasis on proper technique and injury prevention strategies.
- A return to contact sports or overhead activities may take 9-12 months or longer, depending on the individual and surgical findings.
- Goals : Safely return to desired activities without pain or recurrence.
Throughout rehabilitation, close communication between the surgeon, physical therapist, and patient is essential. Modifications to the protocol may be necessary based on individual patient progress and findings at follow-up.
Summary of Key Literature / Guidelines
The literature on posterior glenohumeral dislocation emphasizes early diagnosis and appropriate management to prevent complications.
- Diagnosis : The critical role of axial radiographs (axillary view) and CT scans is consistently highlighted. CT scans are superior for quantifying bone loss (reverse Hill-Sachs and glenoid defects), which directly influences surgical planning. The "Lightbulb Sign" on AP radiographs is a classic indicator, but its presence often indicates a need for further specialized views or CT to confirm.
- Timing of Reduction : Acute dislocations (within 3 weeks) should be managed with prompt, gentle closed reduction under adequate sedation. Delay in reduction significantly increases the risk of avascular necrosis and complicates management.
- Chronic Dislocations : For dislocations presenting >3 weeks, closed reduction attempts carry higher risks of humeral head fracture or AVN. Open reduction is often indicated, and the management algorithm must account for potential humeral head ischemia.
-
Management of Bone Defects
:
- Reverse Hill-Sachs Lesion : Literature supports conservative management for defects <20-25% of the articular surface. For engaging lesions between 25-40%, remplissage (infraspinatus tenodesis into the defect) or bone grafting (autograft or allograft) are recognized techniques to restore stability. For defects >40%, options include osteochondral allograft reconstruction, humeral rotational osteotomy (rare), or arthroplasty (hemiarthroplasty/TSA), particularly in older patients or those with pre-existing arthritis or AVN.
- Posterior Glenoid Bone Loss : Defects exceeding 20-25% of the glenoid width are strongly associated with recurrent instability. Similar to anterior glenoid defects, posterior glenoid bone block procedures (e.g., autogenous iliac crest or allograft) are indicated to restore the glenoid arc and provide mechanical stability.
- Immobilization Post-Reduction : Post-reduction immobilization in slight external rotation (0-15 degrees) is often recommended to prevent re-dislocation, especially for defects that could engage in internal rotation. The duration typically ranges from 3-6 weeks, followed by a structured rehabilitation program.
- Outcomes : Long-term outcomes are generally favorable with timely and appropriate treatment. However, chronic dislocations, large bone defects, and associated AVN significantly worsen prognosis, often leading to poorer functional outcomes and increased rates of arthroplasty.
- Arthroscopic vs. Open : While many stabilization procedures (e.g., posterior labral repair, remplissage) can be performed arthroscopically, complex reductions, large bone grafting procedures, or addressing severe capsular contracture often necessitate an open approach. The choice depends on surgeon experience, lesion complexity, and equipment availability.
These guidelines underscore the importance of a comprehensive diagnostic workup, a tailored surgical strategy based on the specific pathology, and a meticulous post-operative rehabilitation program to optimize outcomes for patients with posterior glenohumeral dislocations.
