Distal Humerus Lateral Approach: Surgical Anatomy, Indications, and Technique
Key Takeaway
The distal humerus lateral approach provides essential access to the lateral epicondyle and capitellum. Key anatomical considerations include careful elevation of the common extensor origin and meticulous identification and protection of the radial nerve and its posterior interosseous branch, vital for preventing iatrogenic injury during surgical exposure.
Distal Humerus Lateral Approach: An Essential Surgical Guide
Introduction & Epidemiology
The lateral approach to the distal humerus is a fundamental exposure in orthopedic elbow surgery, providing direct access to the lateral epicondyle, the origin of the wrist extensors, and the underlying osseous and ligamentous structures. While less extensive than a posterior or posterolateral approach in terms of broad articular visualization, it is invaluable for specific pathologies primarily affecting the lateral column and soft tissues of the elbow. Its judicious application is critical for achieving optimal outcomes while minimizing iatrogenic injury.
Epidemiologically, the conditions treated via the lateral approach are varied. Lateral condyle fractures of the distal humerus, particularly in pediatric populations, constitute a significant proportion of elbow fractures and frequently necessitate open reduction and internal fixation through this approach. Adult unicondylar and capitellum fractures may also be managed laterally. Lateral epicondylitis, or "tennis elbow," is a common musculoskeletal affliction, with an estimated prevalence of 1-3% in the general population, and a subset of refractory cases warrant surgical intervention via a lateral approach. Injuries to the lateral ulnar collateral ligament (LUCL) complex, often associated with posterolateral rotatory instability (PLRI), are less common but represent a critical indication for lateral exposure to facilitate repair or reconstruction.
The approach's utility lies in its directness to key anatomical landmarks and pathological sites while preserving the medial column and ulnar nerve integrity. However, its limitations regarding direct access to the intra-articular space of the elbow joint without extension must be understood to select the appropriate surgical corridor. This guide provides a comprehensive review for the academic orthopedic surgeon, resident, and medical student.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for safe and effective utilization of the lateral approach to the distal humerus.
Osteology
The
distal humerus
presents two distinct columns, medial and lateral, converging to form the articular surface. The
lateral column
consists of the lateral supracondylar ridge, lateral epicondyle, and capitellum.
* The
lateral epicondyle
is the smaller of the two epicondyles, serving as the common origin for the superficial group of extensor muscles of the forearm.
* The
lateral supracondylar ridge of the humerus
is a prominent bony landmark, extending proximally from the lateral epicondyle almost to the deltoid tuberosity. It provides attachment for the brachioradialis and the lateral head of the triceps.
* The
capitellum
is the spherical articular surface on the lateral aspect of the distal humerus, articulating with the radial head. Its integrity is critical for elbow motion and stability.
Ligamentous Structures
The
lateral collateral ligament (LCL) complex
is crucial for posterolateral rotatory stability (PLRI) and varus stability of the elbow. It originates from the lateral epicondyle and consists of:
*
Radial collateral ligament (RCL)
: Blends with the annular ligament.
*
Lateral ulnar collateral ligament (LUCL)
: The primary stabilizer against posterolateral rotation, inserting onto the supinator crest of the ulna.
*
Accessory collateral ligament
: Variable.
*
Annular ligament
: Encircles the radial head, maintaining its articulation with the ulna.
Musculature
The
common extensor origin
comprises several muscles originating from the lateral epicondyle:
*
Extensor carpi radialis brevis (ECRB)
: Most commonly implicated in lateral epicondylitis.
*
Extensor digitorum (ED)
*
Extensor digiti minimi (EDM)
*
Extensor carpi ulnaris (ECU)
* More proximally, the
brachioradialis
originates from the lateral supracondylar ridge and the
lateral head of the triceps
provides a muscular envelope posteriorly.
Neurovascular Structures
The
radial nerve
and its branches are the primary neurovascular structures of concern.
* The
radial nerve
courses anterior to the lateral epicondylar region, typically dividing into its superficial (sensory) and deep (motor, forming the posterior interosseous nerve, PIN) branches anterior to the capitellum, within the supinator muscle or distally.
* The
posterior interosseous nerve (PIN)
pierces the supinator muscle (arcade of Frohse) approximately 2-5 cm distal to the radiohumeral joint. Deep dissection in this region requires meticulous attention to avoid iatrogenic injury.
* The
radial recurrent artery
and its branches are often encountered.
Internervous Planes
The internervous plane for the lateral approach to the distal humerus can be variably utilized depending on the depth and extent of exposure required:
*
Superficial plane
: Between the
brachioradialis
(radial nerve innervation) and the
common extensor origin
(radial nerve innervation). This allows elevation of the common extensor origin from the lateral epicondyle.
*
Deeper plane
: Between the
common extensor origin
(or brachioradialis) and the
triceps
(radial nerve innervation).
Both muscles are innervated by the radial nerve, making this an internervous interval that can be developed without denervation, though careful identification and retraction are crucial. The interval between the common extensor origin and the anconeus (radial nerve) can also be used. For specific pathologies such as lateral condyle fractures or LCL repair, the common extensor origin is often elevated subperiosteally from the lateral epicondyle, exposing the joint capsule directly.
Biomechanics
The lateral column of the distal humerus, in conjunction with the radial head and the LCL complex, provides critical stability to the elbow, particularly against varus stress and posterolateral rotatory forces. Fractures of the lateral condyle or disruption of the LCL complex can lead to instability, impaired motion, and long-term dysfunction. Surgical restoration of anatomical alignment and ligamentous integrity is essential for preserving elbow function.
Indications & Contraindications
The lateral approach to the distal humerus is indicated for a range of conditions primarily affecting the lateral column, its articular surface, and the soft tissue attachments.
Indications
-
Fractures of the Lateral Condyle
:
- Displaced Kocher-Lorenz type fractures (Salter-Harris type IV in skeletally immature patients).
- Milch Type I or II lateral condyle fractures requiring anatomical reduction and stable fixation.
- Selected unicondylar distal humerus fractures with primary lateral column involvement.
-
Fractures of the Capitellum
:
- Hahn-Steinthal (Coronary) and K-T (Kocher-Lorenz) Type I/II fractures requiring open reduction and internal fixation.
- Displaced osteochondral fractures of the capitellum.
-
Lateral Epicondylitis (Tennis Elbow)
:
- Refractory cases failing extensive conservative management (typically 6-12 months).
- Persistent debilitating pain and functional impairment.
- Surgical goals include debridement of pathological tissue (ECRB origin), decortication of the lateral epicondyle.
-
Lateral Collateral Ligament Complex Injuries
:
- Repair or reconstruction of the Lateral Ulnar Collateral Ligament (LUCL) for symptomatic posterolateral rotatory instability (PLRI).
- Chronic, symptomatic LCL insufficiency following elbow dislocation or trauma.
-
Other Indications
:
- Excision of osteochondral fragments or loose bodies from the lateral compartment.
- Removal of prominent hardware from previous lateral elbow surgery.
- Debridement for localized osteoarthrosis of the radiohumeral joint.
Contraindications
- Extensive Medial Column Pathology : Fractures or conditions predominantly involving the medial epicondyle, trochlea, or medial supracondylar ridge, which are better accessed via a medial or posterior approach.
- Communited Intra-articular Fractures : Distal humerus fractures with extensive articular comminution (e.g., C-type fractures) that require broad visualization of the trochlea and both columns for anatomical reduction. These typically necessitate a posterior or posterolateral approach with olecranon osteotomy.
- Active Infection : Any active local or systemic infection is a contraindication to elective surgery.
- Severe Soft Tissue Compromise : Compromised skin integrity, severe scarring, or vascular insufficiency that would preclude safe incision and wound healing.
- Limited Skin Mobility/Contracture : May hinder adequate exposure.
Operative vs. Non-Operative Indications
| Condition | Operative Indications (Lateral Approach) | Non-Operative Indications |
|---|---|---|
| Lateral Condyle Fractures | Displaced (>2mm), unstable, or incarcerated fractures (especially in children). | Minimally displaced (<2mm), stable fractures, often managed with casting/splinting and close radiographic follow-up. |
| Capitellum Fractures | Displaced (>1mm), rotated, or comminuted fractures. | Non-displaced, stable fractures; typically rare for capitellum alone due to articular nature. |
| Lateral Epicondylitis | Refractory cases after 6-12 months of conservative treatment (physiotherapy, NSAIDs, steroid injections). | Initial and primary management strategy: rest, activity modification, NSAIDs, physical therapy, bracing, corticosteroid/PRP injections. |
| Lateral Collateral Ligament Injuries | Symptomatic chronic posterolateral rotatory instability (PLRI), acute complete tears in athletes. | Acute partial tears, mild instability (manage with bracing, PT), non-symptomatic LCL laxity. |
| Loose Bodies | Symptomatic, mechanically blocking motion, or causing pain. | Asymptomatic. |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential to anticipate potential challenges, determine optimal implant selection, and minimize intraoperative complications.
Pre-Operative Planning
-
Imaging Review
:
- Standard Radiographs : AP, lateral, and oblique views of the elbow are crucial for initial assessment of bony pathology.
- Computed Tomography (CT) Scan : Highly recommended for complex fractures (e.g., lateral condyle, capitellum) to define fragment size, displacement, comminution, and articular involvement. 3D reconstructions are invaluable for understanding fracture morphology and planning reduction.
- Magnetic Resonance Imaging (MRI) : Indicated for suspected soft tissue pathology, such as LCL complex tears, chronic lateral epicondylitis (to confirm ECRB pathology), or osteochondral lesions.
-
Implant Selection
:
- Fractures : Small fragment plates (e.g., 2.0 or 2.7 mm, ideally pre-contoured for the lateral column), lag screws (partially threaded, fully threaded), K-wires (for temporary fixation or pediatric fractures), tension band wiring. Variable angle locking plates may be beneficial.
- LCL Reconstruction : Suture anchors, appropriate graft material (autograft: palmaris longus, gracilis; allograft: Achilles tendon, tibialis anterior).
- Lateral Epicondylitis : Suture anchors (for repair/reattachment of ECRB) or debridement tools.
- Contingency Planning : Be prepared for unexpected findings, such as greater comminution than anticipated or difficulty with reduction. Discuss potential need for alternative approaches or extended incisions with the patient pre-operatively.
Patient Positioning
The choice of patient position depends on surgeon preference, the specific pathology, and the need for intraoperative fluoroscopy.
1.
Supine Position
: The patient is placed supine with the arm abducted on a hand table. This is often suitable for straightforward cases or when bilateral access is desired. The elbow is flexed to 90 degrees, allowing gravity to assist with exposure.
2.
Lateral Decubitus Position
: The patient is positioned laterally, allowing the affected arm to hang freely, supported by a padded arm rest or directly on the operating table, with the elbow flexed. This position provides excellent stability for the limb and can facilitate fluoroscopic imaging in multiple planes without repositioning the arm.
3.
Prone Position
: Less commonly used for a pure lateral approach, but can be considered if a posterior or posterolateral extension is anticipated, or for specific challenges.
4.
Tourniquet
: A pneumatic tourniquet is routinely applied to the proximal arm to provide a bloodless field, enhancing visualization and precision during dissection.
5.
Preparation and Draping
: The arm is prepped circumferentially from the hand to the shoulder, and draped to allow full range of motion of the elbow and access to the lateral aspect of the distal humerus. Fluoroscopy should be readily available and checked for adequate views prior to incision.
Detailed Surgical Approach / Technique
Anesthesia and Pre-Incision Steps
General anesthesia is typically administered, often supplemented with a regional nerve block (e.g., supraclavicular or interscalene block) for post-operative analgesia. After positioning and sterile draping, intravenous antibiotics are administered according to institutional protocols. The skin is marked to delineate key anatomical landmarks and the proposed incision line.
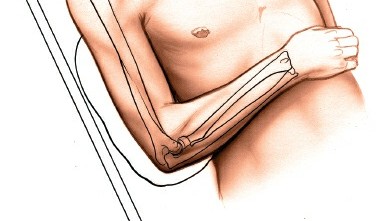
Landmarks and Incision
Palpate the following bony landmarks:
* The
lateral epicondyle
: The most prominent bony projection on the lateral aspect of the distal humerus. It serves as the primary reference point.
* The
lateral supracondylar ridge
: Extends proximally from the lateral epicondyle, feeling distinct and longer than the medial supracondylar ridge.
* The
olecranon
and
radial head
are also palpable and assist in orienting the approach.
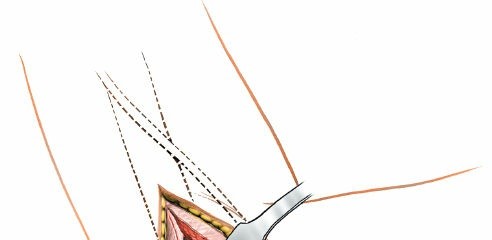
Figure 1: Palpation of bony landmarks, including the lateral epicondyle and supracondylar ridge.
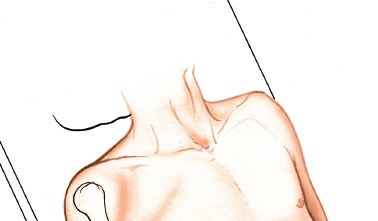
The incision is typically a longitudinal or slightly curvilinear skin incision centered over the lateral epicondyle and extending proximally along the supracondylar ridge and distally towards the radial head. Its length is tailored to the required exposure, usually 4-8 cm. For lateral epicondylitis, a shorter, more precise incision may be used.
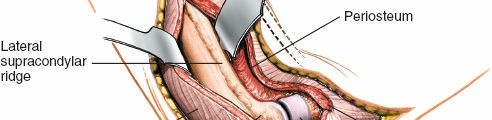
Figure 2: Placement of a curvilinear skin incision centered over the lateral epicondyle.
Subcutaneous Dissection
- The incision is carried through the skin and subcutaneous tissue.
- Careful hemostasis is maintained.
- The superficial radial nerve branch, while typically anterior to this approach, should be identified and protected if more anterior dissection is required. Generally, it courses distally within the fascial plane of the brachioradialis and radial wrist extensors, away from the direct line of exposure for the lateral epicondyle.
Deep Dissection and Internervous Planes
The deep dissection aims to expose the lateral epicondyle and the underlying structures while protecting the radial nerve and its branches.
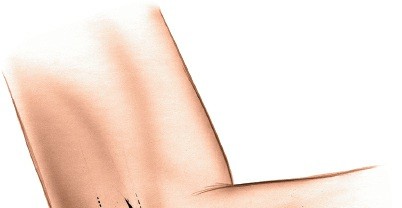
-
Identification of Common Extensor Origin : The fascia overlying the common extensor origin (ECRB, ED, EDM, ECU) is identified originating from the lateral epicondyle.
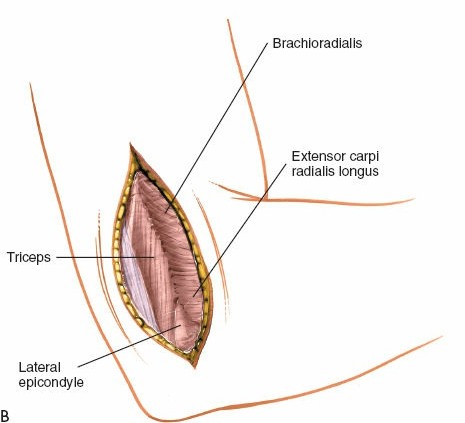
Figure 3: Identification of the common extensor origin. -
Developing the Interval :
- For Lateral Epicondylitis or LCL repair : The common extensor origin is typically elevated subperiosteally from the lateral epicondyle. An incision is made along the anterior margin of the common extensor origin, reflecting it anteriorly and distally. This exposes the underlying capsule and bone.
-
For Fractures (Lateral Condyle, Capitellum)
: The interval between the brachioradialis (anteriorly) and the triceps or anconeus (posteriorly) can be developed. Alternatively, a longitudinal incision through the common extensor mass and capsule can provide direct access to the lateral condyle. The common extensor origin can also be sharply incised and elevated from the lateral epicondyle with a periosteal elevator, providing wide exposure to the lateral column.

Figure 4: Retraction of the common extensor origin to expose the lateral epicondyle and underlying capsule.
-
Radial Nerve Protection : As dissection proceeds deeper and more proximally along the supracondylar ridge, the radial nerve is at risk. It courses anterior to the capitellum and lateral epicondyle. If extending the exposure proximally, dissect posterior to the brachioradialis to avoid injury. If extending distally and anteriorly, be mindful of the radial nerve's division into its superficial and deep branches; the PIN dives into the supinator. Careful palpation and blunt dissection are critical.
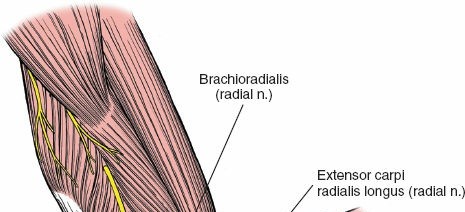
Figure 5: Highlighting the trajectory of the radial nerve and its branches in relation to the surgical field, emphasizing the need for meticulous protection. -
Capsular Incision : Once the lateral epicondyle and, if necessary, the radial head are exposed, an arthrotomy can be performed if direct intra-articular access is required (e.g., for capitellum fractures, loose bodies, or LCL repair). The joint capsule is incised longitudinally, often anterior to the origin of the LUCL to preserve it if possible, or directly through it if reconstruction is planned.
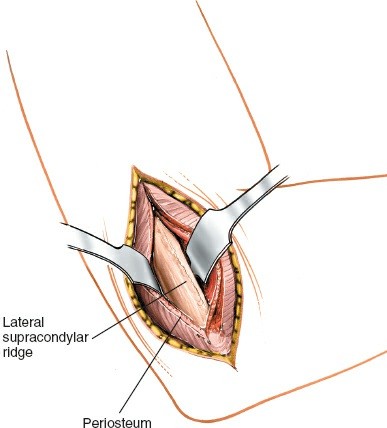
Figure 6: Arthrotomy of the elbow joint capsule, providing direct access to the lateral articular structures.
Specific Procedures
Open Reduction and Internal Fixation (ORIF) of Lateral Condyle Fractures
- After exposing the fracture fragments, the hematoma is evacuated.
- Anatomical reduction is paramount, often aided by gentle traction and manipulation. K-wires can be used for temporary stabilization.
- Fluoroscopy confirms reduction in AP and lateral planes.
-
Fixation typically involves two diverging lag screws, ideally inserted from the lateral epicondyle across the fracture site into the metaphyseal bone of the distal humerus. For larger fragments or comminution, a small fragment plate (e.g., 2.0 mm or 2.7 mm pre-contoured lateral column plate) may be applied. Ensure hardware does not impinge on the articular surface.
Figure 7: Intraoperative image demonstrating fracture reduction and initial K-wire stabilization.
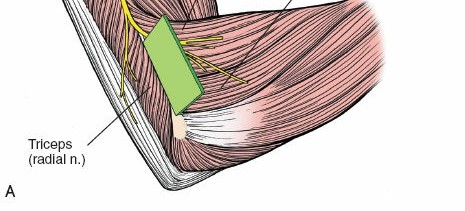
Figure 8: Application of a small fragment plate and screws for stable internal fixation of a lateral condyle fracture.
Surgical Treatment of Lateral Epicondylitis
- After elevating the common extensor origin, the pathological, degenerative tissue (primarily ECRB) at its origin on the lateral epicondyle is identified.
- A localized debridement of this abnormal tissue is performed, typically with sharp dissection or a burr, down to healthy, bleeding bone.
- Decortication of the lateral epicondyle is performed to promote revascularization.
-
The healthy portion of the common extensor origin is either reattached with suture anchors or simply allowed to heal over the decorticated surface. Some surgeons advocate for drilling through the lateral epicondyle (fenestration) to further enhance healing.
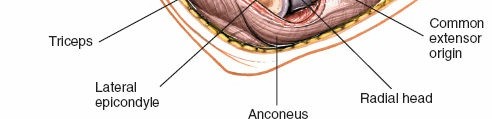
Figure 9: Debridement of degenerative tissue from the ECRB origin in lateral epicondylitis.
Repair/Reconstruction of Lateral Supporting Structures (LCL)
- The LUCL tear is identified, often avulsed from the lateral epicondyle or off its ulnar insertion.
- For acute tears, direct repair with suture anchors into the epicondyle or reattachment to the supinator crest may be feasible.
-
For chronic insufficiency, reconstruction with a tendon graft (e.g., palmaris longus) is performed. The graft is typically woven through bone tunnels created in the lateral epicondyle, humeral condyle (isometric point), and the supinator crest of the ulna to recreate the LUCL's anatomy and restore stability.
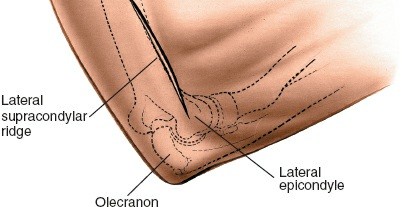
Figure 10: Suture anchor placement for reattachment of the common extensor origin or ligamentous repair.
Closure
- Copious irrigation of the wound.
- The joint capsule (if incised) and common extensor origin are repaired securely with absorbable sutures.
- The subcutaneous tissues are closed in layers.
- The skin is closed with sutures or staples.
- A sterile dressing is applied, and often a well-padded posterior splint or hinged elbow brace is placed, typically in approximately 90 degrees of flexion with the forearm in neutral to slight supination, to protect the repair.
Complications & Management
While generally safe, the lateral approach to the distal humerus carries potential risks. Awareness of these and proactive management strategies are crucial for optimizing patient outcomes.
| Complication | Incidence (Approximate) | Salvage/Management Strategy |
|---|---|---|
| Radial Nerve/PIN Injury | 1-5% | Prevention : Meticulous surgical technique, clear identification of anatomy, careful retraction, avoidance of excessive cautery. Management : Intraoperative recognition allows for immediate repair or neurolysis. Post-operative neuropraxia (most common) is managed with observation, splinting, and physiotherapy; recovery typically occurs within 3-6 months. Persistent deficits or transection may require nerve grafting or tendon transfers. |
| Infection | 1-3% (surgical site) | Prevention : Strict aseptic technique, pre-operative antibiotics, appropriate wound care. Management : Superficial infections often respond to oral antibiotics and local wound care. Deep infections (e.g., osteomyelitis, septic arthritis) require surgical debridement, washout, intravenous antibiotics, and potentially implant removal (especially in hardware-related infections). |
| Heterotopic Ossification (HO) | 5-15% | Prevention : Limited dissection, gentle tissue handling, perioperative NSAIDs (e.g., indomethacin for 3-6 weeks), consideration of radiation therapy for high-risk patients. Management : Early, gentle range of motion. Established symptomatic HO limiting motion may require surgical excision after maturation (usually 6-12 months post-op), followed by prophylaxis. |
| Elbow Stiffness/Loss of Motion | 10-30% | Prevention : Anatomical reduction, stable fixation allowing early motion, rigorous post-operative rehabilitation. Management : Aggressive physical therapy, dynamic splinting. For persistent, severe stiffness after 6-12 months, manipulation under anesthesia or open/arthroscopic arthrolysis (capsular release) may be considered. |
| Nonunion/Malunion (Fractures) | 2-10% | Prevention : Anatomical reduction, rigid internal fixation, careful soft tissue handling. Management : Nonunion typically requires revision surgery with debridement, repeat fixation, and bone grafting (autograft or allograft). Malunion may be treated with osteotomy if symptomatic and functional impairment is significant. |
| Hardware Complications | 5-10% | Prevention : Correct implant sizing and placement, ensuring implants are flush with bone or buried. Management : Symptomatic hardware (prominence causing pain, impingement) often requires removal after fracture healing. Hardware failure (breakage, pullout) necessitates revision surgery. |
| Recurrence (Epicondylitis/LCL) | 5-20% | Prevention : Meticulous surgical technique, appropriate rehabilitation, addressing underlying biomechanical factors. Management : For epicondylitis, further conservative treatment or revision debridement/repair. For LCL instability, revision reconstruction with stronger graft or refined technique may be required. |
| Vascular Injury (Rare) | <0.1% | Prevention : Careful dissection, especially around the anterior capsule and radial neck. Management : Intraoperative repair by a vascular surgeon. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring function, preventing stiffness, and ensuring optimal outcomes following a lateral approach to the distal humerus. Protocols are tailored based on the specific pathology treated and the stability of the surgical repair.
General Principles
- Pain Management : Adequate pain control is essential to facilitate early motion.
- Protection : The surgical site and repair must be protected to allow for initial healing.
- Progressive Loading : Gradual increase in stress and range of motion.
- Patient Education : Clear instructions and expectations for rehabilitation.
Specific Protocols
1. Following Open Reduction and Internal Fixation (ORIF) of Fractures (e.g., Lateral Condyle, Capitellum)
-
Phase 1 (Weeks 0-2: Protection and Early Motion)
- Immobilization : Hinged elbow brace or posterior splint, typically in 90 degrees of flexion with the forearm in neutral rotation for comfort and protection. Splint may be removed for gentle therapy.
- Motion : Initiate gentle, passive and active-assisted range of motion (AAROM) within pain-free limits. Focus on flexion-extension and pronation-supination. Avoid varus stress.
- Weight-bearing : Non-weight bearing for the affected arm.
- Goals : Control pain and swelling, protect fixation, initiate early, controlled motion to prevent stiffness.
-
Phase 2 (Weeks 2-6: Progressive Motion)
- Immobilization : Continue with hinged brace, allowing increasing arcs of motion as tolerated and guided by stability of fixation.
- Motion : Progress to active range of motion (AROM) exercises. Gentle, submaximal isometric exercises for elbow flexors and extensors may be introduced.
- Weight-bearing : Continue non-weight bearing.
- Goals : Gradually increase elbow flexion, extension, pronation, and supination.
-
Phase 3 (Weeks 6-12: Strengthening and Functional Return)
- Immobilization : Discontinue brace if radiographs show adequate healing and clinical stability is good.
- Motion : Full, pain-free range of motion.
- Strengthening : Progressive resisted strengthening exercises for elbow, wrist, and hand muscles. Begin with light resistance and gradually increase.
- Weight-bearing : Gradual return to light functional activities, avoiding heavy lifting or impact.
- Goals : Achieve full, functional range of motion and good strength.
-
Phase 4 (Weeks 12+: Advanced Activities)
- Return to sport/activity specific training. Full strength and endurance training.
- Gradual return to impact or high-demand activities as guided by clinical and radiographic healing.
2. Following Surgical Treatment of Lateral Epicondylitis
-
Phase 1 (Weeks 0-2: Protection and Healing)
- Immobilization : Short period of immobilization in an elbow brace with the wrist in slight extension (to offload extensors).
- Motion : Gentle, passive range of motion for elbow flexion/extension and forearm rotation. Avoid active wrist extension or grasping.
- Goals : Minimize pain and inflammation, protect healing tissue.
-
Phase 2 (Weeks 2-6: Progressive Motion and Gentle Strengthening)
- Motion : Active, pain-free elbow and forearm motion. Gentle, submaximal isometric exercises for wrist extensors.
- Strengthening : Begin with very light resistance for wrist flexion/extension, gradually introducing eccentric loading for wrist extensors as tolerated.
- Goals : Improve range of motion, initiate tendon-healing process with controlled stress.
-
Phase 3 (Weeks 6-12+: Advanced Strengthening and Functional Return)
- Strengthening : Progress to moderate resistance for wrist extensors, emphasizing eccentric exercises. Introduce grip strengthening.
- Activity : Gradual return to work, sport, and daily activities, emphasizing proper biomechanics and ergonomic modifications.
- Goals : Restore full strength and endurance, prevent recurrence.
3. Following Lateral Collateral Ligament (LCL) Repair/Reconstruction
-
Phase 1 (Weeks 0-4: Protection and Controlled Motion)
- Immobilization : Hinged elbow brace locked at 30-90 degrees of flexion with the forearm in neutral to slight supination (to minimize varus/posterolateral rotatory stress).
- Motion : Gentle, passive range of motion within the brace's protected arc. Avoid isolated pronation past neutral and varus stress.
- Weight-bearing : Non-weight bearing for the affected arm.
- Goals : Protect the LCL repair, allow initial ligament healing, prevent stiffness.
-
Phase 2 (Weeks 4-8: Progressive Motion and Light Activity)
- Immobilization : Unlock brace to allow gradual increase in range of motion (e.g., 10-120 degrees). Maintain pronation restriction if LUCL was primary repair.
- Motion : AAROM and AROM exercises. Gentle isometric exercises for elbow flexors/extensors.
- Weight-bearing : Continued non-weight bearing or very light, protected use.
- Goals : Regain functional arc of motion, maintain muscular integrity.
-
Phase 3 (Weeks 8-16: Strengthening and Advanced Loading)
- Immobilization : Gradually wean from brace if stability is good.
- Strengthening : Progressive strengthening for entire upper extremity. Light resistance, gradually increasing.
- Activity : Gradual return to light functional activities, avoiding heavy lifting or activities that place varus or posterolateral rotatory stress on the elbow.
- Goals : Restore full strength and dynamic stability.
-
Phase 4 (Months 4-6+: Return to Sport/Activity)
- Sport-specific drills, plyometrics, and higher-impact activities.
- Full return to sport often not before 6 months, and sometimes longer for reconstruction.
- Goals : Full, unrestricted return to pre-injury activity level.
Summary of Key Literature / Guidelines
The lateral approach to the distal humerus is supported by a robust body of literature and forms the basis for established surgical guidelines for various elbow pathologies.
Fractures of the Lateral Condyle
- Paediatric Fractures : Displaced lateral condyle fractures in children are a classic indication for ORIF via the lateral approach. Studies by Badalamente and Ghillani (1984) and Flynn et al. (1975) highlighted the high incidence of nonunion and malunion with conservative management of displaced fractures, underscoring the necessity of anatomical reduction and stable fixation. Jakob et al. (1983) detailed the anatomical reduction and K-wire fixation technique that remains a cornerstone. Current guidelines emphasize K-wire fixation or cannulated screw fixation for stability and minimal growth plate disturbance. The risk of delayed union, nonunion, and growth disturbance (e.g., fishtail deformity, cubitus valgus) is significantly reduced with timely and appropriate surgical intervention.
- Adult Fractures : While less common, displaced lateral condyle or capitellum fractures in adults also benefit from ORIF via this approach. Bryan et al. (1994) discussed outcomes of capitellum fractures, noting the challenges of achieving anatomical reduction and the importance of secure fixation. The use of small fragment plates and screws has become standard for achieving rigid stability, particularly for comminuted patterns or in osteoporotic bone.
Lateral Epicondylitis
- Surgical intervention for lateral epicondylitis is reserved for refractory cases. The literature generally supports surgical debridement of the pathological ECRB origin and decortication of the lateral epicondyle. Nirschl and Pettrone (1979) popularized the open debridement technique, demonstrating favorable outcomes. Subsequent studies have explored various modifications, including percutaneous release and arthroscopic debridement. While comparative effectiveness research continues, the open lateral approach remains a reliable standard. Recent interest has focused on augmenting debridement with biological agents (e.g., PRP) or considering alternative targets for treatment (e.g., radial nerve decompression in specific cases).
Lateral Collateral Ligament Complex Injuries
- The lateral approach is fundamental for diagnosing and treating posterolateral rotatory instability (PLRI) due to LUCL insufficiency. O'Driscoll et al. (1992) elucidated the pathomechanics of PLRI and the role of the LUCL, establishing it as a primary stabilizer. Nestor et al. (1995) and subsequent authors detailed techniques for LUCL repair and reconstruction. The literature supports anatomical reconstruction with autograft or allograft for chronic instability, focusing on recreating the isometric origin and insertion of the LUCL. Acute repairs are considered for avulsions from the lateral epicondyle, particularly in younger patients.
General Surgical Principles
- Radial Nerve Protection : The literature consistently emphasizes the critical need for meticulous identification and protection of the radial nerve and its branches, especially the posterior interosseous nerve (PIN). Studies on surgical anatomy (e.g., Spinner, 1968 ) detail the course and variations, guiding safe dissection.
- Early Motion : Current evidence strongly supports early, controlled motion protocols post-operatively across most elbow procedures, including those via the lateral approach. This is aimed at minimizing stiffness, a common and debilitating complication.
The lateral approach to the distal humerus, while specific in its indications, is an indispensable tool for the elbow surgeon. Adherence to sound anatomical principles, meticulous technique, and evidence-based rehabilitation protocols are essential for achieving predictable and successful outcomes.
Clinical & Radiographic Imaging