Scapula Fractures: Epidemiology, Classification, Anatomy, and Management
Key Takeaway
Scapula fractures are rare, high-energy injuries requiring careful evaluation for associated life-threatening conditions. Classification systems like AO/OTA and Ideberg guide treatment. A deep understanding of surgical anatomy, including muscle attachments and neurovascular structures, is crucial for effective management and optimal patient outcomes, minimizing long-term morbidity.
Introduction & Epidemiology
Scapula fractures, though relatively uncommon, represent a significant injury often indicative of high-energy trauma. They comprise less than 1% of all bone fractures and approximately 3-5% of shoulder girdle injuries. However, their infrequent occurrence belies the potential for severe associated injuries and significant long-term morbidity if not managed appropriately. These fractures are typically observed in the context of high-impact events such as motor vehicle collisions (50-80%), high-level falls, direct blows to the shoulder, or high-velocity athletic injuries, particularly in contact sports. The substantial force required to fracture the scapula suggests a protective effect of the surrounding musculature and the mobile scapulothoracic articulation.
The mean age of affected individuals is typically in the fourth to fifth decade, with a male predominance. Given the mechanism of injury, associated injuries are prevalent and critical to identify. These can include rib fractures (25-50%), pneumothorax/hemothorax (10-30%), pulmonary contusion, brachial plexus injury (5-10%), subclavian or axillary artery injury, ipsilateral clavicle fracture (often termed "floating shoulder" if associated with a scapular neck fracture, occurring in 20-40% of cases), rotator cuff tears, glenohumeral dislocations, and spinal injuries. The presence of a scapula fracture mandates a thorough secondary survey for these potentially life-threatening or limb-threatening co-pathologies.
Scapula fractures can be broadly classified based on their anatomical location, which guides treatment strategies and prognostic implications. The original seed content categorizes them into neck/body, glenoid cavity, and processes. More detailed classifications used in clinical practice include the AO/OTA classification, which provides a comprehensive system for all scapular elements, and the Ideberg classification, specifically for glenoid fractures.
AO/OTA Classification (Examples):
*
14-A:
Scapular body fractures
*
14-B:
Glenoid fractures
*
14-C:
Scapular neck fractures
*
14-D:
Acromial and coracoid fractures (processes)
Ideberg Classification for Glenoid Fractures:
*
Type I:
Anterior or posterior rim fractures (bony Bankart equivalent)
*
Type II:
Transglenoid fracture with inferior fragment involving the articular surface and the body of the scapula
*
Type III:
Transglenoid fracture with superior fragment involving the articular surface and the coracoid process
*
Type IV:
Transglenoid fracture involving the articular surface and extending into the scapular neck and body, often with a sagittal split
*
Type V:
Type IV fracture with an additional inferior fragment
*
Type VI:
Comminuted (newer addition)
The complexity and variability of scapula fractures necessitate a deep understanding of surgical anatomy, biomechanics, precise imaging, and judicious decision-making regarding operative versus non-operative management.

Surgical Anatomy & Biomechanics
The scapula is a unique, flat, triangular bone forming the posterior component of the shoulder girdle. Its complex three-dimensional shape, surrounded by a multitude of muscle attachments, plays a pivotal role in shoulder kinematics, providing a stable base for glenohumeral joint motion while allowing significant scapulothoracic mobility.
Key Anatomical Features:
- Body: The broad, flat portion, featuring a prominent dorsal spine that divides it into supraspinous and infraspinous fossae.
- Neck: The constricted portion connecting the body to the glenoid, coracoid, and acromion. Fractures here often have significant implications for glenohumeral stability.
- Glenoid Cavity: The shallow, pyriform-shaped articular surface that articulates with the humeral head. Its orientation and integrity are crucial for shoulder joint function. The glenoid labrum further deepens this socket.
- Spine: A prominent ridge on the posterior surface, terminating laterally in the acromion.
- Acromion: A large, flattened process that projects laterally and anteriorly from the spine, forming the highest point of the shoulder and articulating with the clavicle at the acromioclavicular (AC) joint. It serves as an important attachment for the deltoid and trapezius muscles.
- Coracoid Process: A hook-like projection anteriorly and superiorly, providing attachment for the pectoralis minor, coracobrachialis, and short head of the biceps, as well as the coracoclavicular (trapezoid and conoid) and coracoacromial ligaments.
Muscle Attachments and Internervous Planes:
The scapula is enveloped by 17 muscles, providing both mobility and protection. These include the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis), which originate from the scapular fossae, and other periscapular muscles (trapezius, deltoid, levator scapulae, rhomboids, serratus anterior, teres major, latissimus dorsi, pectoralis minor, coracobrachialis, biceps). Understanding these muscle attachments is vital for surgical approaches, as their pull can cause significant fracture displacement.
The
posterior Judet approach
(for scapular body, neck, and spine fractures) typically utilizes the interval between the deltoid and the infraspinatus/teres minor muscles.
*
Deltoid:
Innervated by the axillary nerve (C5-C6).
*
Infraspinatus/Teres Minor:
Innervated by the suprascapular nerve (C5-C6) and axillary nerve (C5-C6), respectively.
Neurovascular Structures at Risk:
- Suprascapular Nerve and Artery: Pass through the suprascapular notch (inferior to the superior transverse scapular ligament) and then through the spinoglenoid notch (inferior to the inferior transverse scapular ligament) to innervate the supraspinatus and infraspinatus muscles. They are at risk during superior or posterior approaches, particularly during screw placement in the scapular spine or neck.
- Axillary Nerve and Posterior Humeral Circumflex Artery: Wrap around the surgical neck of the humerus, but are also closely associated with the inferior glenoid and teres minor. At risk with inferior glenoid fractures or excessively distal dissection in the quadrangular space.
- Long Thoracic Nerve: Runs along the serratus anterior muscle on the medial border of the scapula. At risk during medial dissection.
- Dorsal Scapular Nerve: Supplies the rhomboids and levator scapulae. Less frequently encountered in standard posterior approaches.
- Circumflex Scapular Artery: A branch of the subscapular artery, running through the triangular space (bounded by teres major, teres minor, long head of triceps), provides blood supply to the infraspinatus and posterior deltoid.
Biomechanics:
The scapula acts as a mobile platform for the glenohumeral joint, enhancing range of motion and optimizing rotator cuff function. Scapulothoracic motion is approximately 2:1 ratio to glenohumeral motion during abduction. Fractures can disrupt this delicate balance, leading to pain, stiffness, instability, and rotator cuff dysfunction.
*
Glenoid fractures:
Directly compromise articular congruity and stability, often leading to post-traumatic arthritis or recurrent instability.
*
Scapular neck fractures:
Can alter the orientation of the glenoid, affecting joint mechanics. Displacement can lead to malunion and altered glenohumeral biomechanics.
*
Acromial/Coracoid fractures:
Can affect muscle origins/insertions, leading to weakness, pain, or impingement. Coracoid fractures can also disrupt coracoclavicular ligament integrity, leading to AC joint instability (with associated clavicle fracture).
Understanding the forces acting on the scapula—from direct impact to muscle pull and ligamentous tension—is fundamental to appreciating fracture patterns and designing effective fixation strategies.
Indications & Contraindications
The management of scapula fractures is predominantly non-operative, reflecting the broad muscular envelope, inherent stability from surrounding soft tissues, and the complexity of surgical access. However, specific fracture patterns and patient factors necessitate surgical intervention to restore function and prevent long-term disability. The decision-making process is guided by fracture morphology, displacement, associated injuries, and patient comorbidities.
Indications for Operative Management:
The primary goal of operative fixation is to restore articular congruity, maintain glenoid orientation, and prevent mechanical impingement or instability, especially in the context of high-demand patients or significant displacement.
-
Glenoid Fractures (Ideberg Types II-V):
- Articular Step-off/Gap: > 2-3 mm displacement of the articular surface. This is a critical threshold to prevent post-traumatic arthrosis.
- Glenoid Instability: Often associated with rim fractures (Ideberg Type I) or larger fragments leading to recurrent glenohumeral subluxation or dislocation.
- Fracture involving > 25% of the glenoid articular surface leading to instability.
-
Scapular Neck Fractures:
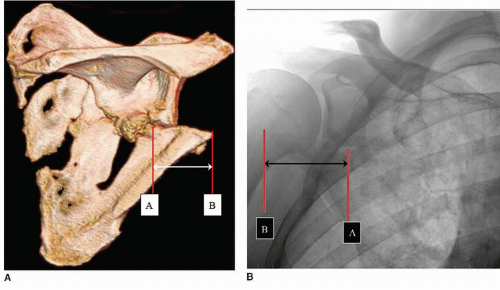
- Angulation: > 30 degrees of angulation relative to the scapular body.
- Medial/Lateral Displacement: > 1 cm of displacement (translation).
- Glenoid Neck Malalignment: Significant displacement or angulation of the glenoid neck fragment relative to the scapular body, leading to malorientation of the glenoid fossa.
-
Floating Shoulder (Ipsilateral Scapular Neck and Clavicle Fracture):
- Traditionally considered an absolute indication, particularly if both are displaced.
- Displacement Criteria: Scapular neck angulation > 40 degrees or lateral translation > 1 cm, in combination with a displaced clavicle fracture.
- Fixation of the clavicle alone may be sufficient in some cases to restore the stability of the shoulder girdle. However, if the scapular component remains unstable or significantly displaced, it warrants direct fixation.
-
Acromial Fractures:
- Displaced Acromial Fractures: Resulting in impingement on the rotator cuff or significant loss of deltoid origin, particularly if displaced > 1 cm or angulated > 40 degrees.
- Significantly displaced fractures involving the base of the acromion (often associated with spinoglenoid notch stenosis and suprascapular nerve compression).
-
Coracoid Fractures:
- Displaced Coracoid Fractures: Affecting the coracoclavicular ligament insertion, leading to significant AC joint instability (often in combination with clavicle fracture).
- Fractures involving the base of the coracoid with significant displacement (e.g., > 1 cm).
-
Scapular Body Fractures:
- Generally treated non-operatively, but may be considered for fixation if severely comminuted, significantly displaced, or part of a floating shoulder injury requiring reconstruction of the scapular platform.
- Rarely fixed in isolation unless extreme displacement, but severe pain and loss of scapulothoracic motion can be an indication.
Contraindications for Operative Management:
- Non-displaced or Minimally Displaced Fractures: Most scapular body, acromial, and coracoid fractures, and some minimally displaced glenoid rim fractures, fall into this category.
- Significant Medical Comorbidities: Patients unable to tolerate general anesthesia or extensive surgery.
- Severe Open Fractures or Contaminated Wounds: May require staged management.
- Local Infection: Active infection at the surgical site.
- Severe Comminution with Small Fragments: Where stable fixation is unlikely to be achieved.
- Patient-specific factors: Non-compliance, severe osteoporosis precluding stable fixation.
Operative vs. Non-Operative Indications Summary Table:
| Fracture Type | Indication for Operative Management | Indication for Non-Operative Management |
|---|---|---|
| Glenoid Fractures |
- Articular step-off/gap > 2-3 mm
- Instability (recurrent subluxation/dislocation) - Fracture involving > 25% articular surface - Associated with floating shoulder (complex cases) - Impingement from displaced fragment (e.g., Type I posterior rim fragment) |
- Minimally displaced articular fractures (< 2 mm step-off)
- Small, stable rim avulsions (e.g., bony Bankart fragments without instability) - Non-displaced Ideberg Type I fractures |
| Scapular Neck Fractures |
- Angulation > 30 degrees
- Medial/lateral displacement > 1 cm - Glenoid malorientation - Part of a floating shoulder with significant displacement criteria (angulation > 40 degrees or lateral translation > 1 cm of scapular neck) |
- Minimally angulated (< 30 degrees) and displaced (< 1 cm) fractures
- Isolated stable neck fractures without significant glenoid malorientation |
| Scapular Body Fractures |
- Severe comminution/displacement leading to significant mechanical symptoms or chronic pain (rarely isolated)
- Part of a floating shoulder requiring restoration of scapular platform (e.g., if associated with severe glenoid or neck displacement) - Significant shortening or rotational deformity |
- Most isolated body fractures are treated non-operatively due to ample muscle coverage and indirect stabilization
- Minimally displaced or non-displaced body fractures - Patients with high surgical risk |
| Acromial Fractures |
- Displaced > 1 cm or angulated > 40 degrees causing mechanical impingement (rotator cuff)
- Significant loss of deltoid origin - Associated with spinoglenoid notch stenosis and suprascapular nerve compression - Failed non-operative treatment with persistent pain/dysfunction |
- Non-displaced or minimally displaced (< 1 cm) fractures
- Fractures not causing significant impingement or loss of deltoid function |
| Coracoid Fractures |
- Displaced > 1 cm with significant loss of coracoclavicular ligament integrity (leading to AC joint instability, often with clavicle fracture)
- Fractures involving the base of the coracoid with significant displacement - Bony impingement on adjacent structures |
- Non-displaced or minimally displaced fractures
- Isolated coracoid tip avulsions without AC joint instability - Fractures not disrupting coracoclavicular ligament attachments significantly - Fractures that are not causing impingement or compromise to other structures like the brachial plexus. |
| Floating Shoulder Injuries | - Combined scapular neck and clavicle fracture with significant displacement (e.g., scapular neck angulation > 40 degrees or lateral translation > 1 cm) - Often clavicle fixation alone may be sufficient, but scapular fixation is considered if the scapular component remains unstable. | - Stable floating shoulder injuries, where clavicle fixation alone effectively reduces the scapular component, or where both components are minimally displaced. Decision-making is nuanced and often relies on the overall stability of the shoulder girdle rather than individual displacement criteria in isolation. |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is paramount for successful scapula fracture management, especially given the complex anatomy, typical high-energy injury mechanism, and high rate of associated injuries.
Pre-Operative Imaging and Assessment:
- Standard Radiographs: Anteroposterior (AP), Y-view (scapular lateral), and axillary views are initial requirements. These provide an overview of the fracture pattern and displacement. Y-view is crucial for assessing glenoid displacement and scapular body angulation. Axillary view best demonstrates glenoid rim fractures.
-
Computed Tomography (CT) Scan with 3D Reconstructions:
This is indispensable. CT provides detailed information regarding:
- Fracture Morphology: Precise delineation of articular step-off/gap, fragment size, comminution, and displacement.
- Glenoid Orientation: Accurate measurement of glenoid version and inclination.
- Associated Injuries: Identification of intra-articular fragments, rotator cuff tears, or labral injuries.
- Surgical Approach Planning: Visualizing the relationship of the fracture to neurovascular structures and planning optimal plate placement and screw trajectories. 3D reconstructions are particularly helpful for understanding the complex anatomy and spatial relationships of fragments.
- Angiography (if vascular injury suspected): For brachial plexus or subclavian/axillary artery injury.
- Neurological Examination: Thorough pre-operative assessment of brachial plexus and peripheral nerve function is critical to detect and document any baseline deficits.
Pre-Operative Templating:
Using images or 3D models, surgeons can pre-bend plates to match the scapular anatomy. This saves considerable time intra-operatively and improves contouring precision, especially for the lateral border, spine, and glenoid neck. Consideration should be given to specific scapular plating systems which often have pre-contoured plates.
Patient Positioning:
The choice of patient position depends heavily on the fracture location and the selected surgical approach.
-
Prone Position:
- Indications: Most common for posterior approaches (e.g., Judet approach) to access the scapular body, spine, neck, and posterior glenoid.
- Setup: Patient is placed prone on a radiolucent table. The ipsilateral arm is draped free or rested on an arm board, allowing full range of motion. Chest rolls or a beanbag are used to elevate the trunk and allow the scapula to fall anteriorly, providing easier posterior access. Ensure adequate padding of pressure points (chest, iliac crests, knees, feet).
- Advantages: Excellent exposure of the posterior scapula, gravity helps reduce some fracture fragments, allows for intra-operative fluoroscopy without repositioning.
- Disadvantages: Challenges with airway management, potential for brachial plexus stretch with arm manipulation, difficulty accessing anterior structures.
-
Lateral Decubitus Position:
- Indications: Can be used for posterior approaches, particularly when a floating shoulder requires concomitant clavicle fixation, or when concurrent arthroscopic assessment or rotator cuff repair is anticipated. Also suitable for anteroinferior glenoid approaches (e.g., Deltopectoral).
- Setup: Patient is placed lateral, affected side up. A beanbag secures the patient. The arm is often prepped and draped free. Axillary roll for neural protection.
- Advantages: Allows for access to both posterior and superior aspects of the shoulder, easier for anesthesia, can accommodate arthroscopy.
- Disadvantages: Requires careful positioning to prevent traction injuries, less ideal for posterior glenoid and extensive body fractures compared to prone.
-
Beach Chair Position:
- Indications: Less common for extensive scapula fractures, but can be used for superior approaches (e.g., acromial or superior glenoid fractures), or for cases requiring anterior approach to the coracoid or glenoid rim.
- Setup: Patient is placed semi-recumbent. Head secured, arm draped free.
- Advantages: Familiar position for shoulder surgeons, good for anterior/superior access.
- Disadvantages: Limited posterior access, potential for hypotensive bradycardia (vasovagal syncope).
Anesthesia and Monitoring:
- General anesthesia is standard.
- Regional anesthesia (interscalene block) can be considered for post-operative pain control, but care must be taken to not mask neurological deficits.
- Neuromonitoring (SSEP, EMG) may be considered if brachial plexus injury is a high risk or for prolonged cases with significant neurovascular dissection.
- Type and crossmatch for blood products, especially in polytrauma patients.
Detailed Surgical Approach / Technique
Surgical treatment of scapula fractures requires precise anatomical knowledge and meticulous technique to restore function while protecting vital neurovascular structures. The specific approach and fixation strategy are dictated by the fracture pattern, displacement, and surgeon's preference.
General Principles of Scapula Fracture Fixation:
- Anatomical Reduction: Especially critical for articular surfaces (glenoid) and the glenoid neck/fossa relationship.
- Stable Fixation: Achieved with plates and screws, providing sufficient rigidity to allow early mobilization.
- Preservation of Soft Tissues: Minimize devascularization of fragments and extensive muscle stripping.
- Protection of Neurovascular Structures: Meticulous dissection and identification of nerves and vessels.
Common Surgical Approaches:
1. Posterior Judet Approach (for Scapular Body, Neck, Spine, and Posterior Glenoid)
- Indications: Most scapular body, neck, spine, and posterior glenoid fractures (Ideberg Type II, IV, V, VI).
- Patient Positioning: Prone position, ipsilateral arm draped free, chest rolls to elevate the trunk.
-
Incision & Dissection:
- A curvilinear incision is made starting from the superior aspect of the scapular spine, curving laterally and inferiorly along the posterior border of the acromion, and then extending inferiorly along the lateral border of the scapula. The length is tailored to the fracture extent.
- The skin and subcutaneous tissues are incised. Subcutaneous flaps are elevated to expose the deep fascia.
- The deltoid muscle is identified. The interval between the deltoid and the infraspinatus/teres minor muscles is developed. This is the primary internervous plane.
- The deltoid origin from the scapular spine and acromion can be partially released if more superior exposure is needed, but minimize this to preserve deltoid function.
- The infraspinatus (superiorly) and teres minor (inferiorly) are identified. These muscles are often elevated from the scapular body to expose the fracture. An L-shaped or Z-shaped release of the infraspinatus origin can be performed from the posterior aspect of the scapula, leaving a cuff of tissue for later repair.
-
Neurovascular Structures at Risk:
- Suprascapular Nerve and Artery: Most vulnerable in the spinoglenoid notch and suprascapular notch. The spinoglenoid notch is located at the junction of the scapular spine and the glenoid neck. Avoid aggressive dissection or screw placement medial to this notch when targeting the scapular spine or neck. When elevating infraspinatus, elevate subperiosteally to protect.
- Axillary Nerve and Posterior Humeral Circumflex Artery: Located inferiorly, exiting the quadrangular space. Protection typically involves staying superior to the inferior border of the teres minor.
-
Fracture Reduction Techniques:
- Direct visualization of fracture fragments.
- Reduction clamps: Hohmann retractors, pointed reduction clamps, Verbrugge clamps can be used to manipulate and stabilize fragments.
- K-wires or Kirschner wires: Can be used as joysticks or temporary fixation.
- Indirect Reduction: For highly comminuted body fractures, maintaining length and rotation can be achieved by fixing the lateral border to the glenoid neck, then fixing the medial fragments to this construct.
- Glenoid Reduction: For articular fractures, meticulous reduction under direct vision (arthroscopy can also aid) is performed, often starting with the largest articular fragment.
-
Fixation Strategies:
- Plates and Screws: Low-profile locking plates (2.7mm or 3.5mm systems) are commonly used. These are contoured to the complex shape of the scapula.
-
Typical plating constructs:
- Lateral Border Plate: Applied to the lateral border of the scapula, extending onto the glenoid neck. This is a workhorse plate, providing stability to the glenoid-scapular body junction.
- Spine Plate: Applied to the posterior aspect of the scapular spine, often bridging comminuted body fragments.
- Bridge Plating: For comminuted body fractures, plates can span the comminution without directly fixing all fragments, preserving vascularity.
- Glenoid Fractures: Small fragment plates (2.0 or 2.4 mm) or screws alone (cannulated or non-cannulated) are used for glenoid articular fragments. Screws must be strategically placed to avoid violating the articular surface or endangering the suprascapular nerve.
- Screw Lengths: Measured carefully, especially in the glenoid, to avoid cortical penetration into the joint or posterior to the bone (into soft tissues or neurovascular bundles).
- Repair: After fixation, the elevated muscles (infraspinatus, deltoid) are repaired back to their origins or to the surrounding fascia/capsule. Layered closure.
2. Anterolateral / Deltopectoral Approach (for Coracoid, Anterior Glenoid Rim, and Anterior Scapular Neck)
- Indications: Coracoid fractures, anterior glenoid rim fractures (Ideberg Type I anterior), anterior scapular neck fractures.
- Patient Positioning: Beach chair or lateral decubitus.
-
Incision & Dissection:
- A deltopectoral incision is made, starting from the clavicle and extending distally in the deltopectoral groove.
- The deltopectoral interval is developed by retracting the deltoid laterally and the pectoralis major medially.
- The cephalic vein is identified and retracted laterally with the deltoid.
- The clavipectoral fascia is incised inferior to the coracoid.
-
Neurovascular Structures at Risk:
- Musculocutaneous Nerve: Pierces the coracobrachialis muscle. At risk during dissection around the coracoid.
- Axillary Nerve: Located inferior to the glenoid, but can be at risk with extensive inferior dissection.
- Brachial Plexus: Located medial to the coracoid, deep to the pectoralis minor. Avoid deep medial retraction.
-
Fixation Strategies:
- Coracoid Fractures: Lag screws or tension band wiring, depending on the fragment size and fracture pattern.
- Anterior Glenoid Rim Fractures: Small fragment screws, often cannulated, or suture anchors (for concomitant labral repair) are used.
3. Superior Approach (e.g., for Acromion or Superior Glenoid)
- Indications: Displaced acromial fractures, some superior glenoid fractures (Ideberg Type III).
- Patient Positioning: Beach chair or lateral decubitus.
-
Incision & Dissection:
- An incision is made directly over the superior aspect of the acromion or along the superior border of the scapular spine.
- Dissection involves splitting the deltoid fibers or elevating the deltoid origin.
-
Neurovascular Structures at Risk:
- Suprascapular Nerve: At risk in the suprascapular notch and spinoglenoid notch.
-
Fixation Strategies:
- Acromial Fractures: Screws, tension band wiring, or small plate fixation. If comminuted, an acromial hook plate or small fragment plate may be considered.
- Superior Glenoid Fractures: Small screws or plates, carefully considering suprascapular nerve location.
Specific Fracture Type Considerations:
-
Glenoid Fractures (Ideberg Classification):
- Type I (Rim): Often treated non-operatively, but if unstable or >25% articular surface involved, direct screw fixation (anterior or posterior approach depending on rim involved).
- Type II (Inferior): Posterior Judet approach is common. Fixation involves buttress plating from the posterior glenoid to the lateral border.
- Type III (Superior): Can involve the coracoid. Often approached posteriorly or superiorly. Fixation with screws and/or small plates. Be mindful of suprascapular nerve.
- Type IV (Transglenoid/Body split): Posterior Judet approach. Requires reconstruction of the glenoid articular surface and stabilization of the body split.
- Type V (Type IV + inferior fragment): Similar to Type IV, often requiring more extensive plating of the lateral border and glenoid neck.
- Type VI (Comminuted): Very challenging. May require extensive plating, bone grafting, or in rare cases, glenoid arthroplasty if irreparable.
-
Scapular Body and Neck Fractures:
- Primarily treated via the Posterior Judet approach.
- Reconstruction aims to restore the scapular platform and maintain glenoid version.
- Bridge plating for comminuted body fractures. Anatomical plates for the lateral border and spine.
-
Acromial and Coracoid Fractures:
- Acromial fractures often fixed with small plates, screws, or tension band wiring via a superior approach.
- Coracoid fractures typically fixed with lag screws via anterolateral approach.
-
Floating Shoulder Injuries:
- The current consensus often favors clavicle fixation alone if it adequately reduces the scapular component.
- If scapular displacement persists after clavicle fixation (e.g., >1 cm translation, >40° angulation of the scapular neck), or if the scapular component itself meets criteria for fixation, then both are addressed. The scapular component is typically fixed via a posterior approach.
Complications & Management
Scapula fractures, especially those treated surgically, are associated with a range of potential complications, reflecting the high-energy trauma, complex anatomy, and proximity to vital neurovascular structures. A thorough understanding of these complications and their management strategies is critical for orthopedic surgeons.
Intra-operative Complications:
- Neurovascular Injury: Injury to the suprascapular nerve (most common), axillary nerve, or circumflex scapular artery during dissection or screw placement. Meticulous identification and protection are paramount. Immediate repair or nerve grafting may be necessary.
- Excessive Blood Loss: Due to proximity to large vessels or extensive dissection. Requires careful hemostasis and potentially blood transfusion.
- Incomplete Reduction: Failure to achieve adequate anatomical reduction, particularly of the articular surface. May require revision or accept the compromise depending on severity.
- Intra-articular Screw Placement: Detected by direct visualization, fluoroscopy, or intra-operative arthroscopy. Requires immediate revision.
Early Post-operative Complications:
- Wound Infection: Incidence ranges from 1-5%. Managed with antibiotics, debridement, and potentially hardware removal.
- Hematoma: Due to inadequate hemostasis. May require drainage.
- Nerve Palsy (New or Worsening): Most commonly suprascapular nerve neuropraxia or axillary nerve injury. Often transient due to traction or swelling. Requires observation, electrodiagnostic studies, and potential nerve exploration if no recovery.
- Pneumothorax/Hemothorax: Rare, but possible with medial dissection or chest wall trauma. Requires chest tube insertion.
Late Post-operative Complications:
- Nonunion: Failure of the fracture to heal. More common in comminuted fractures, open fractures, or in patients with poor bone quality. May require revision surgery with bone grafting and more robust fixation.
- Malunion: Healing of the fracture in an anatomically unacceptable position. Can lead to chronic pain, shoulder stiffness, glenohumeral arthritis, impingement, or altered scapulothoracic mechanics. Depending on severity, may require corrective osteotomy.
- Stiffness/Loss of Range of Motion: Common, particularly after glenoid or neck fractures, or prolonged immobilization. Managed with aggressive physical therapy, manipulation under anesthesia, or rarely, arthroscopic capsular release.
- Post-traumatic Arthritis: Especially after articular glenoid fractures with residual step-off or incongruity. Can progress to require glenohumeral arthroplasty (total shoulder or hemiarthroplasty).
- Implant Failure: Plate breakage, screw pullout, or loss of reduction. Due to inadequate fixation, premature loading, or nonunion. Requires revision surgery.
- Painful Hardware: Impingement of plates or screws on soft tissues, especially prominent plates along the scapular spine or lateral border. May require hardware removal after fracture union.
- Chronic Pain: Can result from various factors, including malunion, nerve injury, chronic soft tissue irritation, or psychological factors. Multidisciplinary pain management.
Complications and Management Summary Table:
| Complication | Incidence | Salvage/Management Strategy |
|---|---|---|
| Neurovascular Injury | 2-10% (nerve) |
-
Immediate:
Meticulous identification & protection during surgery. If injury occurs, primary repair (for sharp transection), or observation (for neuropraxia).
- Post-op: Electrodiagnostic studies (EMG/NCS). Nerve exploration & repair/grafting if no recovery after 3-6 months. |
| Wound Infection | 1-5% |
-
Superficial:
Oral/IV antibiotics, local wound care.
- Deep: Surgical debridement, IV antibiotics, hardware retention if fracture stable, or removal if unstable/persistent infection. Muscle flaps for coverage if severe. |
| Hematoma | 2-5% |
-
Small:
Observation, compression.
- Large/Expanding: Surgical drainage, identification & control of bleeding source. |
| Nonunion | 1-5% |
-
Aseptic:
Revision surgery with debridement, rigid fixation, and bone grafting (autograft/allograft).
- Septic: As for deep infection (debridement, antibiotics, staged reconstruction). |
| Malunion | 5-15% |
-
Mild/Asymptomatic:
Observation, physical therapy.
- Symptomatic (pain, stiffness, impingement, arthritis): Corrective osteotomy (scapular body, neck, glenoid), hardware removal, or eventually arthroplasty for post-traumatic arthritis. |
| Stiffness/Loss of ROM | 10-30% |
-
Early:
Aggressive physical therapy, pain management.
- Persistent: Manipulation under anesthesia (MUA), arthroscopic capsular release, open capsulotomy (less common). Rule out hardware impingement or malunion. |
| Post-traumatic Arthritis | 5-20% |
-
Early/Mild:
NSAIDs, injections, physical therapy.
- Advanced: Glenohumeral arthroplasty (total shoulder arthroplasty or hemiarthroplasty), possibly reverse shoulder arthroplasty if rotator cuff deficient or complex glenoid defect precluding standard TSA. Consider glenoid reconstruction first if feasible for younger patients. |
| Implant Failure | 1-5% |
-
Early:
Revision surgery with more rigid fixation, potentially bone grafting. Address underlying cause (poor bone quality, inadequate fixation).
- Late (after union): Often managed with hardware removal if symptoms are from implant prominence or impingement. |
| Painful Hardware | 5-15% | - Observation initially. If pain persists after fracture union (typically 6-12 months post-op), elective hardware removal. Rule out other causes of pain (nonunion, malunion, nerve entrapment). |
| Chronic Pain Syndrome | Variable | - Multidisciplinary pain management (medications, nerve blocks, physical therapy, psychological counseling). Address underlying mechanical causes (malunion, stiffness, nerve entrapment). |
| Pneumothorax/Hemothorax (Iatrogenic) | < 1% | - Chest X-ray. Chest tube insertion for drainage and lung re-expansion. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following scapula fracture fixation is critical for optimizing functional outcomes, preventing stiffness, and protecting the surgical repair. Protocols are tailored to the fracture type, surgical construct stability, associated injuries, and patient factors. The general principles involve a phased approach progressing from protection and pain control to gradual restoration of range of motion, strength, and functional activities.
Phase I: Immobilization & Early Passive Range of Motion (Weeks 0-6)
- Goals: Protect fixation, control pain and swelling, prevent shoulder stiffness, promote wound healing.
-
Immobilization:
- Sling immobilization (e.g., universal shoulder sling or abduction pillow sling) for comfort and protection. Duration typically 4-6 weeks, but may be shorter for very stable constructs or longer for complex cases.
- Crucial: Encourage proper scapular positioning within the sling to avoid undue tension on surgical repair.
-
Pain and Edema Management:
- Analgesics (opioids, NSAIDs, neuropathic agents as needed).
- Cryotherapy, elevation.
-
Early Motion (within pain limits):
- Pendulum exercises: Gentle, gravity-assisted swings of the arm.
-
Passive Range of Motion (PROM):
In non-painful arcs, guided by a therapist.
- Forward elevation: Typically limited to 90 degrees initially.
- External rotation: Often limited to 0-30 degrees depending on fracture location (e.g., posterior glenoid fractures may have more restriction).
- Internal rotation: Limited to abdomen initially.
- Elbow, Wrist, Hand ROM: Active exercises to prevent stiffness in uninvolved joints.
- Scapular Mobilization: Gentle, passive scapular glides to prevent scapulothoracic adhesions, within comfort.
- Weight-Bearing: No weight-bearing or lifting with the affected arm.
- Precautions: Avoid active shoulder elevation, abduction, and forceful external rotation to prevent stress on the repair. Avoid sudden movements.
Phase II: Active-Assisted & Active Range of Motion (Weeks 6-12)
- Goals: Gradually restore full, non-painful range of motion, begin gentle strengthening.
- Progression based on radiographic union and clinical stability.
-
Active-Assisted Range of Motion (AAROM):
- Pulleys, wall walks, cane exercises to increase forward elevation, abduction, and rotation.
- Continue PROM if AAROM is limited.
-
Active Range of Motion (AROM):
- As tolerance allows, gradually progress to active shoulder movements without assistance.
- Focus on achieving functional range for activities of daily living (ADLs).
-
Gentle Strengthening (Isometric):
- Begin with isometric exercises for rotator cuff and scapular stabilizers (e.g., submaximal contractions without movement).
- Focus on shoulder girdle stabilization (rhomboids, serratus anterior, trapezius).
- Manual Therapy: Soft tissue mobilization to address muscle tightness and scar tissue restrictions.
- Precautions: Avoid heavy lifting, sudden jerking movements, or high-impact activities. Continue to protect the surgical site.
Phase III: Strengthening & Advanced Rehabilitation (Weeks 12-24)
- Goals: Achieve full functional range of motion and significant strength, prepare for return to activity.
-
Progressive Strengthening:
- Isotonic exercises: With light resistance (bands, light weights) for all planes of shoulder motion.
- Rotator cuff strengthening: Internal and external rotation, scapular plane abduction.
- Scapular stabilization exercises: Push-ups (wall, then floor), rows, prone extensions to target serratus anterior, rhomboids, trapezius.
- Core strengthening: To improve overall stability.
-
Proprioception and Neuromuscular Control:
- Balance exercises, rhythmic stabilization exercises.
-
Endurance Training:
- Cycling, elliptical.
-
Activity-Specific Training:
- Gradual introduction of sport-specific or work-specific movements, focusing on proper mechanics.
- Precautions: Continue to avoid overhead heavy lifting or activities that cause pain. Listen to the body.
Phase IV: Return to Activity (Months 6+)
- Goals: Return to full unrestricted activities, including sports or physically demanding occupations.
-
Criteria for Return:
- Full, pain-free range of motion.
- Strength at least 90% of the contralateral side.
- Excellent neuromuscular control and proprioception.
- No pain or instability with activity-specific movements.
-
Gradual Return:
- Progress from light to full activity over several weeks or months.
- Emphasize proper technique and warm-up.
- Continue with a maintenance exercise program.
Key Considerations:
*
Individualization:
Protocols must be customized for each patient. Age, fracture complexity, bone quality, compliance, and associated injuries all influence progression.
*
Communication:
Close communication between the surgeon, physical therapist, and patient is essential for safe and effective rehabilitation.
*
Pain as a Guide:
While some discomfort is expected, sharp or increasing pain warrants re-evaluation.
*
Delayed Union/Nonunion:
If observed, rehabilitation may be modified or paused, and further surgical intervention considered.
Summary of Key Literature / Guidelines
Scapula fractures, though rare, have garnered increasing attention in orthopedic literature due to advancements in imaging, surgical techniques, and a better understanding of their biomechanical implications. The literature highlights the challenges in diagnosis, the evolving indications for surgery, and the importance of meticulous surgical execution and rehabilitation.
Diagnostic Evolution:
Early literature primarily relied on plain radiographs. The advent of Computed Tomography (CT) with 3D reconstructions has been a game-changer, transforming the ability to accurately characterize fracture patterns, especially for intra-articular glenoid fractures and complex neck/body injuries. Studies by Goss (1989) and subsequent authors emphasized the critical role of CT in surgical planning and identifying "floating shoulder" injuries.
Classification Systems:
The Ideberg Classification (1984) for glenoid fractures remains a cornerstone in guiding treatment decisions for articular injuries, correlating fracture type with prognosis and surgical approach. The more comprehensive AO/OTA Classification provides a universal system for all scapular segments, aiding in research and communication. Recent literature occasionally includes a Type VI (comminuted) to the Ideberg system, acknowledging the complexity of highly fragmented glenoid injuries.
Operative vs. Non-Operative Management:
Historically, the majority of scapula fractures were treated non-operatively due to the difficulty of surgical access and the perception that the surrounding musculature provides adequate stability. However, several landmark studies and reviews have refined the indications for surgery, shifting towards earlier operative intervention for specific unstable fracture patterns.
*
Quadrangular Space/Scapulothoracic Dissociation:
While not a fracture classification, recognition of this highly unstable injury (often associated with extensive soft tissue damage and severe displacement) mandates urgent surgical intervention.
*
Glenoid Fractures:
Consensus now largely supports surgical fixation for articular step-off > 2-3 mm, significant instability, or fractures involving >25% of the articular surface.
Hardy et al. (2009)
and
Kim et al. (2015)
are among many who have demonstrated improved outcomes with surgical fixation of displaced articular fractures.
*
Scapular Neck Fractures:
Displaced (lateral translation > 1 cm) or significantly angulated (> 30 degrees) neck fractures are increasingly managed surgically to prevent malunion and maintain glenoid orientation.
*
Floating Shoulder:
The management of this combined ipsilateral clavicle and scapular neck fracture has evolved. Initial recommendations often favored double fixation (clavicle and scapula). However, more recent literature, including a meta-analysis by
van der Linde et al. (2013)
, suggests that isolated clavicle fixation may be sufficient to reduce the scapular component and restore overall shoulder girdle stability in many cases, provided the scapular fracture is not excessively displaced after clavicle fixation. The decision remains nuanced and depends on the degree of residual scapular displacement.
*
Acromial and Coracoid Fractures:
Generally treated non-operatively, but operative fixation is indicated for significant displacement leading to impingement, loss of deltoid origin, or instability of the coracoclavicular ligaments.
Surgical Approaches and Techniques:
The posterior Judet approach remains the workhorse for scapular body, neck, and posterior glenoid fractures. Detailed anatomical studies have highlighted the importance of protecting the suprascapular nerve in the spinoglenoid notch and the axillary nerve. Advances in plate technology, including pre-contoured locking plates, have improved the stability and ease of fixation.
Outcomes and Complications:
While surgical fixation can yield excellent functional outcomes, complication rates are notable. Neuropraxia of the suprascapular nerve is frequently reported, often transient. Post-traumatic arthritis remains a significant long-term concern, especially for inadequately reduced glenoid fractures. Studies continue to emphasize the importance of early, aggressive, but protected rehabilitation to mitigate stiffness and maximize functional recovery.
Current Guidelines and Future Directions:
There are no universally accepted, level I evidence-based guidelines due to the rarity of these fractures. Most recommendations are based on expert consensus, biomechanical studies, and high-quality retrospective series.
*
Personalized Approach:
The current trend emphasizes a personalized approach, integrating fracture morphology, patient demographics, activity level, and associated injuries into the treatment decision.
*
Minimally Invasive Techniques:
While open reduction is standard, there is ongoing research into minimally invasive techniques and percutaneous fixation for select fracture patterns, particularly to reduce soft tissue dissection.
*
Advanced Imaging and Navigation:
Further integration of 3D printing for pre-operative planning and intra-operative navigation systems may enhance precision and reduce complications in complex cases.
In summary, the literature underscores that while most scapula fractures are managed non-operatively, a subset of displaced articular, neck, or process fractures, as well as complex floating shoulder injuries, benefit from surgical stabilization. Meticulous pre-operative planning, precise surgical technique, careful neurovascular protection, and a structured rehabilitation program are critical for achieving optimal patient outcomes.
