Shoulder Osteoarthritis: A Comprehensive Academic Review of Etiology, Epidemiology & Anatomy
Key Takeaway
Shoulder osteoarthritis (OA) is a degenerative joint disease involving cartilage breakdown, subchondral bone remodeling, and osteophyte formation, leading to pain and stiffness. It primarily affects individuals over 50. Causes include idiopathic factors, post-traumatic injury, rotator cuff arthropathy, avascular necrosis, and inflammatory conditions, impacting both glenohumeral and acromioclavicular joints.
Understand Descriptionshoulder Osteoarthritis: Full Details Here
Introduction & Epidemiology
Shoulder osteoarthritis (OA) is a degenerative joint disease characterized by the progressive destruction of articular cartilage, subchondral bone remodeling, osteophyte formation, and capsular thickening, ultimately leading to pain, stiffness, and functional impairment. While five major types of arthritis can affect the shoulder, osteoarthritis, often termed "wear-and-tear" arthritis, represents a significant proportion of degenerative shoulder pathologies requiring surgical intervention.
The pathology of osteoarthritis involves a complex interplay of mechanical stress, biochemical changes, and genetic predisposition. It initiates with the breakdown of the smooth, resilient articular cartilage, particularly its collagen network and proteoglycan content. As the cartilage degenerates, it becomes frayed, fissured, and rough, losing its ability to absorb shock and provide a low-friction surface for joint movement. This leads to a reduction in the protective joint space. With advanced cartilage loss, the subchondral bone is exposed, resulting in "bone-on-bone" articulation. This direct bone-to-bone contact during movement is a primary source of severe pain and accelerates the degenerative process. The subchondral bone reacts to increased stress by sclerosis, cyst formation, and the development of peripheral osteophytes, which further restrict joint motion. Concurrently, the joint capsule often thickens and contracts, contributing to loss of range of motion, particularly external rotation.

Epidemiologically, shoulder osteoarthritis predominantly affects individuals over 50 years of age, with its incidence increasing significantly with advancing age. While often described as idiopathic primary osteoarthritis, secondary forms are common and arise from identifiable etiologies such as:
*
Post-traumatic arthritis:
Following fractures of the humeral head or glenoid, dislocations, or chronic instability.
*
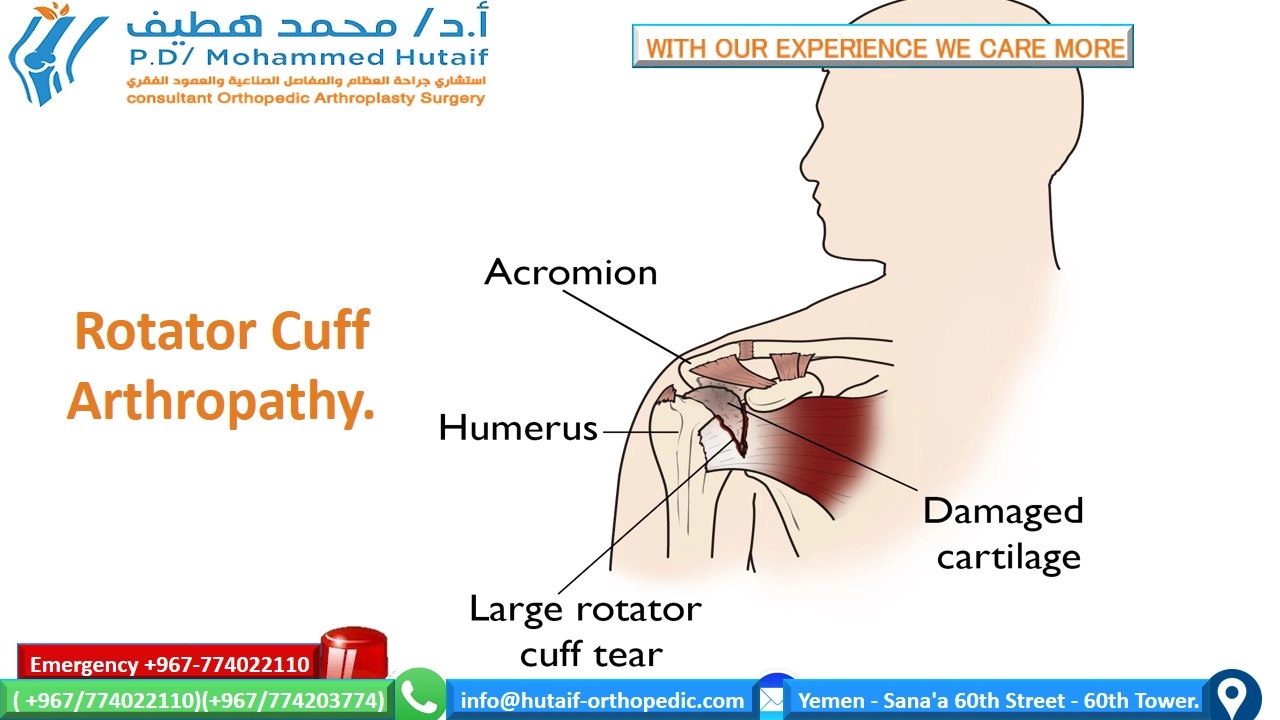
Rotator cuff arthropathy (Cuff Tear Arthropathy - CTA):
Chronic, massive rotator cuff tears lead to superior migration of the humeral head, erosion of the acromion and glenoid, and incongruity, often with associated articular cartilage loss. This represents a distinct and severe form of shoulder arthritis.
*
Avascular necrosis (AVN):
Interruption of blood supply to the humeral head, leading to collapse of the articular surface. Etiologies include corticosteroid use, alcohol abuse, trauma, sickle cell disease, and idiopathic causes.
*
Inflammatory arthropathies:
Rheumatoid arthritis, psoriatic arthritis, ankylosing spondylitis, though these typically present with symmetric joint involvement and specific serological markers.
*
Dysplasia or congenital abnormalities:
Such as glenoid dysplasia.
*
Infection:
Septic arthritis can lead to rapid cartilage destruction and secondary OA.
The shoulder encompasses two primary articulations commonly affected by OA: the glenohumeral (GH) joint and the acromioclavicular (AC) joint. While AC joint osteoarthritis is more prevalent radiographically, affecting up to 50% of individuals over 60, it is often asymptomatic. Symptomatic AC OA typically presents with localized pain, especially with overhead activities or cross-body adduction. Glenohumeral OA, though less common than AC OA, is generally more debilitating and is the primary focus for reconstructive surgical interventions like arthroplasty. The incidence of symptomatic GH OA is estimated to be around 10-15% in the elderly population, with a significant proportion eventually requiring surgical management. Risk factors include advanced age, genetic predisposition, previous trauma or surgery, obesity, and occupational or athletic activities involving repetitive overhead movements.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the shoulder joint is paramount for successful arthroplasty.
Glenohumeral Joint
The glenohumeral joint is a multiaxial ball-and-socket synovial joint, providing the greatest range of motion of any joint in the body, albeit at the cost of inherent stability.
-
Articular Surfaces:
- Humeral Head: Approximately one-third of a sphere, covered by articular cartilage. Its retroversion (typically 30-40 degrees relative to the epicondylar axis) and inclination (130-140 degrees relative to the humeral shaft) are critical considerations during prosthetic implantation. In OA, the humeral head may lose its sphericity and develop osteophytes inferiorly and posteriorly.
- Glenoid: A shallow, pear-shaped fossa on the lateral aspect of the scapula. It is significantly smaller than the humeral head, covering only about 25-30% of the humeral head's surface, which contributes to its mobility. The glenoid normally has a retroversion of 0-10 degrees and an inclination of 0-5 degrees superiorly. In primary GH OA, eccentric posterior wear of the glenoid is common due to the dominance of posterior-directed forces and relatively weaker posterior cuff muscles. This can lead to increased glenoid retroversion and posterior humeral head subluxation.
- Glenoid Labrum: A fibrocartilaginous ring attached to the rim of the glenoid, deepening the socket and providing attachment for the glenohumeral ligaments. While important for stability in healthy joints, in advanced OA, it may be degenerate or completely absent.
- Joint Capsule: A fibrous sac surrounding the joint, thickened anteriorly by the superior, middle, and inferior glenohumeral ligaments, which act as primary static stabilizers. In OA, the capsule often becomes thickened and contracted, limiting motion.
-
Rotator Cuff:
Composed of four muscles: supraspinatus, infraspinatus, teres minor (posterior cuff), and subscapularis (anterior cuff). These muscles dynamically stabilize the GH joint and are crucial for shoulder elevation and rotation.
- Supraspinatus: Initiates abduction.
- Infraspinatus & Teres Minor: External rotation.
-
Subscapularis:
Internal rotation.
Integrity and function of the rotator cuff are critical for the success of anatomical total shoulder arthroplasty (TSA). In cuff tear arthropathy (CTA), the rotator cuff is deficient, leading to superior migration of the humeral head and necessitating reverse total shoulder arthroplasty (rTSA).
- Long Head of Biceps Tendon: Originates from the supraglenoid tubercle and superior labrum, courses through the bicipital groove, and acts as a humeral head depressor and weak elbow flexor/forearm supinator. Its status (tendinopathy, rupture) often accompanies GH OA.
- Scapulothoracic Joint: A physiological joint between the scapula and the posterior thoracic cage, providing a stable base for glenohumeral motion and contributing significantly to the overall range of motion (scapulohumeral rhythm).
Neurovascular Structures
Understanding the proximity of neurovascular structures is critical to prevent iatrogenic injury during surgical approaches.
- Axillary Nerve: The most commonly injured nerve in shoulder surgery. It courses inferiorly from the quadrangular space, deep to the deltoid, supplying the deltoid and teres minor muscles. It lies approximately 5-7 cm distal to the acromion on the lateral aspect of the humerus.
- Suprascapular Nerve: Originates from the upper trunk of the brachial plexus, passes through the suprascapular notch (under the transverse scapular ligament) to innervate the supraspinatus, and then through the spinoglenoid notch to innervate the infraspinatus. It is at risk during glenoid preparation, especially with eccentric reaming or screw placement, and during extensive posterior capsular release.
- Brachial Plexus: Lies medial to the coracoid process, making it vulnerable during deep anterior dissection, particularly with excessive retraction.
- Axillary Artery and Vein: Located deep to the pectoralis minor, medial to the humeral head. Extensive medial retraction or deep dissection can put these structures at risk.
- Cephalic Vein: A superficial vein within the deltopectoral groove, serving as a key landmark for the deltopectoral surgical approach.
Biomechanics of Osteoarthritis
In GH OA, the altered biomechanics are characterized by:
*
Loss of Concavity-Compression:
The primary stabilizing mechanism of the GH joint, where compressive forces across the joint create stability due to the glenoid's concave surface. Cartilage loss and incongruity diminish this effect.
*
Altered Rotator Cuff Function:
Pain and stiffness lead to muscle weakness and dysfunction, further destabilizing the joint.
*
Posterior Glenoid Wear:
Commonly seen in primary OA, leading to progressive posterior humeral head subluxation and increased retroversion, placing abnormal stress on the remaining cartilage and promoting further degradation. This often requires specialized glenoid component placement or augmented glenoids in arthroplasty.
*
Loss of Scapulohumeral Rhythm:
Due to pain and stiffness, the coordinated movement between the scapula and humerus is disrupted, leading to compensatory movements and often scapular dyskinesis.
Indications & Contraindications
The decision-making process for surgical intervention in shoulder osteoarthritis is multifaceted, balancing patient factors, disease severity, and potential surgical outcomes. Surgical options primarily include glenohumeral arthroplasty (hemiarthroplasty, anatomical total shoulder arthroplasty, reverse total shoulder arthroplasty) or less commonly, débridement/arthroscopy for very early stages.
Indications for Operative Management
The overarching indication for surgical intervention is unrelenting shoulder pain and functional disability that has failed a comprehensive course of non-operative management. Specific criteria include:
- Pain: Severe, constant, intractable pain at rest or with activity, unresponsive to analgesics and other conservative treatments. Night pain is a hallmark of advanced disease.
- Functional Limitation: Significant loss of active and passive range of motion, impacting activities of daily living (ADLs), self-care, sleep, and occupational/recreational activities.
- Radiographic Evidence: Advanced degenerative changes, typically Grades 3-4 on the Samilson-Prieto or modified Hamada classification for GH OA, or Grade III-IV on the Hamada classification for CTA. Features include joint space narrowing (<2mm), subchondral sclerosis, osteophyte formation, subchondral cysts, and often humeral head superior migration (in CTA) or posterior subluxation (in primary OA). CT scans provide detailed assessment of glenoid bone loss and version.
- Failed Non-Operative Treatment: A minimum of 3-6 months of non-operative measures, including physical therapy, activity modification, NSAIDs, and corticosteroid injections, without significant improvement in symptoms.
- Patient Expectations: Realistic understanding of surgical goals, potential risks, and post-operative rehabilitation requirements.
Choice of Arthroplasty:
- Anatomical Total Shoulder Arthroplasty (TSA): Indicated for primary glenohumeral OA with an intact rotator cuff and sufficient glenoid bone stock to accommodate a prosthetic glenoid component. Requires a functional deltoid muscle.
- Hemiarthroplasty (HA): May be considered for younger, active patients with primary GH OA where glenoid cartilage is preserved or in cases of severe humeral head pathology (e.g., AVN) with an intact glenoid and rotator cuff, where concerns exist regarding glenoid component longevity. Often a salvage procedure or for proximal humerus fractures in older patients with some arthritis.
-
Reverse Total Shoulder Arthroplasty (rTSA):
Indicated for:
- Cuff Tear Arthropathy (CTA): Patients with massive, irreparable rotator cuff tears and symptomatic GH OA.
- Failed Anatomical TSA: Due to rotator cuff failure or glenoid loosening.
- Proximal Humerus Fractures: In elderly patients with osteoporotic bone, particularly fracture-dislocations, where reconstruction is challenging and rotator cuff integrity is compromised.
- Complex Primary OA: With significant glenoid bone loss or severe retroversion where anatomical TSA is challenging, especially in older patients.
-
Revision of previous shoulder arthroplasty.
The rTSA relies on the deltoid muscle for elevation and requires a functional deltoid.
Contraindications for Operative Management
-
Absolute Contraindications:
- Active Local or Systemic Infection: Underscores the critical importance of infection screening and eradication prior to elective arthroplasty.
- Significant Deltoid Dysfunction/Deficiency (for rTSA): The rTSA relies heavily on deltoid function; absence precludes its use.
- Brachial Plexus Palsy or Paralysis: Compromises neural control of the shoulder, making functional recovery unlikely.
- Inadequate Bone Stock: Severe bone loss in the humerus or glenoid that cannot be reconstructed with available implants or bone grafting.
- Severe Medical Comorbidities: Uncontrolled cardiac, pulmonary, renal, or metabolic diseases that significantly increase anesthetic and surgical risks, making the patient medically unfit for surgery.
- Patient Non-Compliance: Unwillingness or inability to adhere to post-operative rehabilitation protocols.
-
Relative Contraindications:
- Prior Shoulder Arthrodesis: While not an absolute contraindication, it complicates subsequent arthroplasty.
- Neuropathic Arthropathy (Charcot Joint): High risk of implant loosening and failure.
- Young Age: Generally a relative contraindication for arthroplasty due to concerns regarding implant longevity and the potential for revision surgery. For younger patients, non-operative measures or arthroscopic débridement/microfracture may be explored first.
- Smoking: Increases risk of complications (infection, wound healing, periprosthetic fracture). Smoking cessation is strongly encouraged pre-operatively.
- Obesity: Increased surgical difficulty, higher infection risk, and potential for altered biomechanics.
- Unrealistic Patient Expectations: Poor understanding of surgical limitations or expected outcomes.
Table: Operative vs. Non-Operative Indications
| Feature/Treatment | Non-Operative Management | Operative Management |
|---|---|---|
| Pain | Mild to moderate, intermittent, tolerable | Severe, constant, intractable, night pain, functional limitation |
| Function | Mild to moderate limitation, manageable with adaptations | Significant loss of active and passive ROM, impacting ADLs/work |
| Radiographs | Early degenerative changes (Grade 1-2 Samilson-Prieto/Hamada) | Advanced degenerative changes (Grade 3-4 Samilson-Prieto/Hamada) |
| Failure of Cons. | No prior extensive non-operative trials | Failed minimum 3-6 months of comprehensive non-operative management |
| Patient Age | Generally younger or medically unfit | Older, medically fit (often >50-60, though variable) |
| Rotator Cuff | Intact or minor tears (not typically an isolated decision pt) | Intact (for TSA/HA) or irreparable massive tear (for rTSA) |
| Glenoid Bone | Adequate (not severely eroded) | Adequate for implantation (TSA), or severe loss manageable with rTSA/aug |
| Surgical Options | NSAIDs, PT, injections, activity modification, viscosuppl. | Hemiarthroplasty, Anatomical TSA, Reverse TSA |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and precise patient positioning are critical for optimizing surgical outcomes and minimizing complications in shoulder arthroplasty.
Pre-Operative Planning
-
Clinical Assessment:
- Detailed History: Pain characteristics (location, quality, intensity, aggravating/alleviating factors), duration of symptoms, impact on ADLs, previous treatments, and patient expectations.
- Physical Examination: Assessment of active and passive range of motion, strength of rotator cuff and deltoid, stability, palpation for tenderness (e.g., AC joint, biceps groove), and neurovascular status.
-
Imaging Studies:
- Radiographs: Essential initial workup. Standard series includes true AP (Grashey view), scapular Y lateral, and axillary lateral views. These provide information on joint space narrowing, osteophyte formation, subchondral sclerosis, cyst formation, superior humeral head migration (CTA), and glenoid morphology.
- Computed Tomography (CT) Scan: The gold standard for assessing glenoid bone loss, version, and inclination. A dedicated shoulder CT with 1-2 mm cuts, including true axial and coronal oblique views, is vital for precise glenoid component planning, particularly in cases of posterior eccentric wear (Walch classification). 3D reconstruction helps visualize the true extent of deformities. CT is also useful for assessing humeral head AVN and bone quality.
- Magnetic Resonance Imaging (MRI): Primarily indicated for assessing rotator cuff integrity, particularly in cases where TSA is considered. It can also evaluate the extent of AVN, labral pathology, and other soft tissue abnormalities. However, it is less reliable than CT for bone morphology.
-
Templating and Implant Selection:
- Utilizing specialized software or radiographic overlays, the surgeon templates for the appropriate size and type of humeral stem and head, and glenoid component.
- Considerations include: humeral head size, offset, neck-shaft angle, stem length and diameter (cemented vs. press-fit), glenoid component type (keeled vs. pegged, standard vs. augmented, metal-backed vs. all-polyethylene), and overall system (anatomical vs. reverse).
- For rTSA, planning includes glenosphere diameter, lateralization, and inferior overhang to optimize stability and prevent scapular notching.
- Patient-specific instrumentation (PSI) and 3D printing of glenoid guides derived from CT data are increasingly utilized for complex glenoid deformities to improve accuracy of component placement.
- Medical Optimization: Comprehensive medical clearance, including cardiac and pulmonary evaluations. Optimization of comorbidities (diabetes, anemia, nutritional status). Smoking cessation counseling is mandatory. Pre-operative antibiotics protocol is established.
Patient Positioning
Two primary positions are utilized for shoulder arthroplasty: the beach chair position and the lateral decubitus position. Each has distinct advantages and disadvantages.
-
Beach Chair Position:
-
Advantages:
- Familiar to many orthopedic surgeons, especially those performing arthroscopy.
- Allows for easy access to the entire shoulder girdle, including the AC joint, and facilitates range of motion assessment intra-operatively.
- Better anesthetic control of the airway.
- Lower risk of brachial plexus traction injury compared to lateral decubitus.
- Gravity-assisted visualization of the surgical field and blood control.
-
Disadvantages:
- Risk of cerebral hypoperfusion, especially in hypotensive patients, requiring careful monitoring of mean arterial pressure.
- Potential for nerve palsies (e.g., ulnar nerve at the elbow, peroneal nerve if legs are crossed).
- Requires a specialized shoulder chair and often more complex draping.
-
Technique:
- Patient is placed on a radiolucent operating table, with the torso elevated 30-70 degrees from horizontal, resembling a semi-sitting position.
- Head is supported in a neutral position to avoid cervical extension or flexion, secured in a headrest (e.g., gel donut or Mayfield clamps).
- The ipsilateral arm is draped free, allowing full manipulation during surgery. A hand table may be used for support when not being actively manipulated.
- Careful padding of bony prominences (heels, elbows, sacrum) is essential.
- The scapula is allowed to move freely off the table to facilitate glenoid exposure.
- Blood pressure monitoring at heart level, and consideration of non-invasive cerebral oximetry, are crucial to prevent cerebral ischemia.
-
Advantages:
-
Lateral Decubitus Position:
-
Advantages:
- Maintains better hemodynamic stability.
- Can provide excellent exposure, especially for posterior approaches or difficult glenoid access.
- Easier to achieve traction, which can aid in joint distraction and exposure.
-
Disadvantages:
- More challenging to assess intra-operative range of motion.
- Risk of brachial plexus stretch injury due to traction, requiring careful weight application and duration.
- Risk of suprascapular nerve injury due to traction.
- Requires specialized setup, including an axillary roll, beanbag positioner, and traction tower.
-
Technique:
- Patient is positioned on their unaffected side, secured with a beanbag or kidney rests.
- An axillary roll is placed in the contralateral axilla to protect the brachial plexus from compression.
- The operative arm is typically suspended from a traction tower, allowing controlled distraction.
- Careful padding of bony prominences (fibular head, olecranon, iliac crest) is paramount.
- Head and neck are maintained in a neutral position.
-
Advantages:
Skin Preparation and Draping:
After positioning, the entire shoulder, including the clavicle, scapula, and upper arm down to the elbow, is prepared with an antiseptic solution (e.g., chlorhexidine or povidone-iodine). The limb is draped free using sterile impervious drapes, ensuring a wide sterile field to accommodate instrumentation and manipulation.
Detailed Surgical Approach / Technique
The primary surgical treatment for advanced glenohumeral osteoarthritis is arthroplasty. The choice between anatomical total shoulder arthroplasty (TSA) and reverse total shoulder arthroplasty (rTSA) depends on rotator cuff integrity and glenoid bone stock. Hemiarthroplasty is less common but still has specific indications. The standard approach for shoulder arthroplasty is the deltopectoral approach.
Deltopectoral Approach (General Principles)
The deltopectoral approach utilizes the interval between the deltoid and pectoralis major muscles, an internervous plane, minimizing muscle damage.
- Incision: A curvilinear incision approximately 10-15 cm long, starting from the inferior border of the clavicle, just medial to the coracoid process, extending distally in the deltopectoral groove toward the deltoid insertion.
-
Dissection to Interval:
- Skin and subcutaneous tissue are incised. The cephalic vein is identified within the deltopectoral groove. It can be retracted laterally with the deltoid or medially with the pectoralis major. Often, it is ligated and divided if it interferes with exposure.
- The interval between the deltoid (lateral) and pectoralis major (medial) is developed. The deltoid receives innervation from the axillary nerve, while the pectoralis major receives innervation from the lateral and medial pectoral nerves. This internervous plane ensures minimal neurological compromise to these muscles.
- Subdeltoid Space: The interval is developed distally, and the deltoid is gently elevated from the underlying structures. The clavipectoral fascia is incised longitudinally to expose the coracoid process and its attached muscles (coracobrachialis, short head of biceps, pectoralis minor).
- Coracoid & Humeral Retraction: The deltoid and pectoralis major are retracted laterally and medially, respectively. A self-retaining retractor is carefully placed. The coracoid can be a significant impediment to exposure; in some cases, a small portion of the pectoralis major tendon may be released from the inferior clavicle, or the conjoined tendon may be mobilized inferiorly.
-
Subscapularis Management:
The anterior capsule and subscapularis tendon are exposed. The musculotendinous junction of the subscapularis is identified. The subscapularis can be managed in one of two ways:
- Subscapularis Tenotomy: The tendon is sharply released from its insertion on the lesser tuberosity along its superior and inferior borders. Stay sutures are placed for later repair. This is the most common technique for anatomical TSA.
- Lesser Tuberosity Osteotomy: A small bone block of the lesser tuberosity with the subscapularis insertion is osteotomized. This offers a stronger repair, especially in revision cases or for patients with poor tendon quality, but carries a small risk of non-union. This technique is more commonly used in rTSA or revision TSA.
- Note: In rTSA, the subscapularis can be repaired, partially repaired, or not repaired depending on the surgeon's preference and tendon quality. Some surgeons prefer to preserve the subscapularis completely in rTSA for stability if possible, using a specific "subscapularis-sparing" approach.
- Capsulotomy: After subscapularis management, the underlying capsule is incised. The choice is typically an anterior capsulotomy, either longitudinally or in a T-shape.
- Humeral Head Dislocation: The arm is externally rotated and extended to dislocate the humeral head anteriorly.
Anatomical Total Shoulder Arthroplasty (TSA) Technique
For patients with an intact rotator cuff and adequate glenoid bone stock.
-
Humeral Head Osteotomy:
- Using specialized cutting guides or freehand, the humeral head is resected at the anatomical neck. The cut angle (typically 130-140 degrees) and retroversion (30-40 degrees relative to epicondylar axis) are crucial for restoring normal anatomy and preventing overstuffing or impingement.
- Bone quality, especially in the metaphysis, is assessed for stem fit.
-
Humeral Preparation:
- The humeral canal is progressively reamed and broached to prepare for the humeral stem.
- Trial components are inserted to confirm proper fit and alignment.
- Cemented or cementless stems can be used, depending on bone quality and surgeon preference.
-
Glenoid Preparation:
- Exposure of the glenoid typically requires careful posterior retraction of the humeral shaft, protection of the axillary nerve inferiorly, and avoidance of excessive tension on the brachial plexus.
- All remaining articular cartilage and osteophytes are meticulously removed from the glenoid surface.
- The central peg or keel hole is drilled, and the glenoid surface is reamed to a spherical contour, correcting any posterior eccentric wear or retroversion using eccentric reaming or augmented glenoids.
- Trial glenoid components are inserted to ensure full seating and optimal version/inclination.
- Proper reaming is crucial to avoid "rocker-bottoming" or uneven stress distribution on the glenoid component.
-
Component Implantation:
- The definitive glenoid component (typically all-polyethylene, cemented) is implanted. Care is taken to ensure complete seating and remove all extruded cement.
- The definitive humeral stem is implanted (cemented or press-fit), followed by the humeral head component (metal or ceramic).
-
Reduction & Stability:
- The shoulder joint is reduced.
- Range of motion (ROM) is assessed in all planes to ensure adequate motion, stability, and absence of impingement. Soft tissue balancing is critical.
-
Closure:
- The subscapularis tendon is meticulously repaired to its insertion point on the lesser tuberosity using strong non-absorbable sutures (e.g., #2 FiberWire in a modified Mason-Allen or Krackow fashion). This is a critical step for anterior stability and strength.
- Capsular repair, if performed, further enhances stability.
- The deltopectoral interval is loosely reapproximated.
- Subcutaneous layers and skin are closed. A drain may be placed temporarily.
Reverse Total Shoulder Arthroplasty (rTSA) Technique
For patients with cuff tear arthropathy, failed TSA, or other indications requiring deltoid reliance.
-
Humeral Head Osteotomy:
- Similar to TSA, the humeral head is resected, but often with a less aggressive osteotomy or a more vertical cut to allow for proper sizing and tensioning.
-
Glenoid Preparation & Baseplate Fixation:
- The glenoid is exposed as in TSA.
- All osteophytes and remaining cartilage are removed.
- The central point for the glenoid baseplate is identified and drilled.
- The glenoid surface is minimally reamed to ensure a flat, stable platform for the baseplate.
- The glenoid baseplate is implanted, typically with a central screw and multiple peripheral locking screws. Screw length and trajectory are crucial to avoid scapular notching and protect neurovascular structures (especially the suprascapular nerve).
- Bone grafting may be necessary for significant glenoid bone loss.
- The glenosphere (a metal hemisphere) is then attached to the baseplate. The size of the glenosphere and its offset (lateralization, inferior overhang) are critical for optimizing deltoid tension and preventing scapular notching.
-
Humeral Preparation:
- The humeral canal is reamed and broached.
- The humeral tray (meta-diaphyseal component) is implanted, either cemented or press-fit, ensuring proper retroversion (often less retroversion than anatomical TSA, sometimes 0-20 degrees).
- The polyethylene liner is then secured to the humeral tray.
-
Reduction & Stability:
- The joint is reduced.
- Range of motion, stability, and soft tissue tension are carefully assessed. The rTSA aims to restore deltoid tension and lever arm to compensate for rotator cuff deficiency.
-
Closure:
- The subscapularis is typically not repaired or only partially repaired in rTSA, particularly if it was irreparable pre-operatively. Some surgeons advocating a "subscapularis-sparing" approach in rTSA for specific indications will repair it.
- The deltopectoral interval is reapproximated.
- Subcutaneous layers and skin are closed, often with a drain.
Hemiarthroplasty (HA) Technique
Less common for primary OA, usually for younger patients with intact glenoid cartilage or AVN.
- Humeral Head Osteotomy: Similar to TSA.
- Humeral Preparation: Similar to TSA.
- Component Implantation: Only the humeral stem and head components are implanted. The glenoid is left untouched if cartilage is pristine, or débrided if necessary.
- Reduction & Stability: Joint is reduced, ROM and stability assessed.
- Closure: Subscapularis repair and standard layered closure.
Complications & Management
Shoulder arthroplasty, while highly effective, is associated with a range of potential complications. A thorough understanding of their incidence and management strategies is crucial for all orthopedic surgeons.
Common Complications and Management
| Complication | Incidence (%)* (General Range) | Management Strategy |
|---|---|---|
| Infection | 0.5 - 2% | Acute (<4-6 weeks): Irrigation and débridement (I&D), polyethylene exchange, IV antibiotics, implant retention if stable. Chronic (>4-6 weeks): Two-stage revision arthroplasty (excision arthroplasty with antibiotic spacer, followed by reimplantation), long-term suppressive antibiotics if patient unfit for revision, or arthrodesis. Prophylaxis is key. |
| Neurovascular Injury | 1 - 5% | Axillary Nerve: Most common. Immediate post-op clinical assessment. If deficit, observation initially, EMG studies at 3 weeks. If no recovery, consider neurolysis or nerve grafting. Brachial Plexus: Rare, usually traction-related. Avoid excessive traction/retraction. Management similar to axillary nerve. |
| Periprosthetic Fracture | 1 - 3% | Intra-operative: Depends on location and stability. Cerclage wiring, open reduction internal fixation (ORIF), or revision to a longer, cemented stem. Post-operative: ORIF, revision arthroplasty (longer stem, cement), or non-operative for non-displaced stable fractures. |
| Instability/Dislocation | 1 - 5% (Higher in rTSA) | Anatomical TSA: Often due to subscapularis failure/non-union, glenoid malposition, or soft tissue imbalance. Management: closed reduction, sling. If recurrent: revision of subscapularis, component revision, or revision to rTSA. rTSA: Often due to insufficient tension, component malposition, or trauma. Management: closed reduction, sling. If recurrent: revision with larger glenosphere, lateralization, or revision of humeral component. |
| Glenoid Loosening | 5 - 10% (TSA, long-term) | Aseptic: Symptomatic loosening requires revision of the glenoid component, potentially with bone grafting or conversion to rTSA, especially in cases of significant bone loss or rotator cuff deficiency. Asymptomatic loosening may be observed. Septic: Managed as per infection protocol (two-stage revision). |
| Rotator Cuff Failure (TSA) | 5 - 15% | Tears of the remaining rotator cuff (often subscapularis or supraspinatus) can lead to pain and instability. Management: repair if reparable, otherwise often leads to conversion to rTSA, particularly if glenoid is loose or humeral head migration occurs. |
| Scapular Notching (rTSA) | 5 - 50% (Radiographic) | Inferior erosion of the scapular neck by the humeral polyethylene liner. Risk factors: medialized glenosphere, insufficient inferior overhang. Often asymptomatic. Symptomatic notching can lead to pain, loosening, or reduced ROM. Management: observation if asymptomatic. If symptomatic: revision with increased inferior overhang or lateralization. |
| Stiffness/Arthrofibrosis | 5 - 10% | Early, aggressive but controlled physical therapy is key. Manipulation under anesthesia (MUA) if unresponsive to therapy. If severe and recalcitrant, arthroscopic or open capsular release may be necessary. |
| Heterotopic Ossification (HO) | 10 - 20% (Radiographic) | Ectopic bone formation around the joint. Often asymptomatic. Prophylaxis: NSAIDs (Indomethacin) or radiation for high-risk patients. Symptomatic HO (pain, stiffness) may require surgical excision, but recurrence is common. |
| Component Malposition | Varies (Surgeon experience) | Leads to impingement, instability, early wear, or restricted ROM. Management: often requires revision arthroplasty to correct alignment. |
| Deltoid Failure (rTSA) | <1 - 5% | Loss of deltoid integrity (e.g., nerve injury, avulsion from acromion) leading to functional loss. Management: deltoid repair or transfer if possible, otherwise functional outcome severely compromised. |
| Hematoma | 1 - 3% | Requires drainage if tense or expanding, to prevent pressure on nerves and infection. |
*Incidence varies widely based on study design, surgical volume, patient population, and follow-up duration.
General Principles of Complication Management
- Prevention: Meticulous surgical technique, proper patient selection, pre-operative optimization, appropriate antibiotic prophylaxis, and early, supervised rehabilitation are the cornerstones of complication prevention.
- Early Recognition: Prompt identification of complications through vigilant post-operative monitoring (clinical examination, imaging, lab studies) allows for timely intervention.
- Multidisciplinary Approach: Management of complex complications often requires collaboration with infectious disease specialists, neurologists, physical therapists, and other medical professionals.
- Revision Surgery: Many complications, particularly those involving implant failure or severe instability, necessitate revision arthroplasty, which is technically more demanding and often associated with higher complication rates than primary surgery. Conversion from anatomical TSA to rTSA is a common revision pathway.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral and critical component of successful shoulder arthroplasty, aimed at restoring range of motion, strength, and function while protecting the surgical repair. Protocols vary slightly depending on the type of arthroplasty (TSA vs. rTSA) and surgeon preference, but generally follow a phased approach.
General Principles
- Pain Management: Adequate pain control is essential to allow for patient participation in therapy.
- Protection: Initial phases emphasize protecting the surgical repairs (e.g., subscapularis in TSA, deltoid in rTSA) from excessive stress.
- Gradual Progression: Exercises are advanced incrementally based on healing, pain levels, and functional milestones.
- Patient Education & Compliance: Patients must understand the importance of adherence to the protocol and activity restrictions.
- Supervised Therapy: Regular sessions with a qualified physical therapist are crucial for proper technique and progression.
Phase I: Maximum Protection Phase (Weeks 0-6)
- Goal: Protect surgical repair, minimize pain, reduce inflammation, promote passive range of motion.
- Immobilization: Sling use is mandatory, typically for 4-6 weeks, removing only for exercises and hygiene. For rTSA, sometimes a brace with an abduction pillow is preferred.
- Pain & Edema Control: Ice, oral analgesics, muscle relaxants.
-
Exercise Focus (TSA):
- Passive Range of Motion (PROM): Initiated immediately (often within 24-48 hours post-op). Pendulum exercises. Supine passive forward elevation (to tolerance, typically 90-120 degrees). External rotation to neutral or slightly past neutral (0-30 degrees) if subscapularis was repaired, or to tolerance if not. Internal rotation is typically avoided initially.
- Scapular Mobility: Gentle scapular retraction and protraction exercises.
- Elbow, Wrist, Hand AROM: To prevent stiffness in uninvolved joints.
-
Exercise Focus (rTSA):
- PROM: Emphasis on passive forward elevation (often greater than TSA, 90-140 degrees) and external rotation in the plane of the scapula. Internal rotation is often more restricted and may be limited initially. Avoidance of combined adduction and internal rotation.
- Scapular Mobility: Crucial for deltoid function.
- Elbow, Wrist, Hand AROM:
- Activity Restrictions: No active elevation or external rotation (TSA). No lifting, pushing, pulling. Avoid supporting body weight with the operative arm. Avoid reaching behind the back.
Phase II: Moderate Protection / Early Active Motion Phase (Weeks 6-12)
- Goal: Gradually restore active range of motion, initiate gentle strengthening, improve neuromuscular control.
- Sling Use: Typically discontinued around week 6, as tolerated.
- Pain Management: Continued as needed.
-
Exercise Focus (TSA):
- Active-Assisted Range of Motion (AAROM): Pulleys, wand exercises, therapist assistance for forward elevation, external and internal rotation.
- Active Range of Motion (AROM): Gradually initiate AROM as pain allows, particularly forward elevation and external rotation.
- Light Isometrics: Gentle isometric contractions for rotator cuff and deltoid, with arm at side.
- Scapular Stabilization: Progress scapular strengthening exercises.
-
Exercise Focus (rTSA):
- AAROM/AROM: Continue progressive forward elevation. Emphasis on deltoid activation and scapular rotation for elevation. External rotation may be more limited than in TSA due to altered biomechanics.
- Deltoid Strengthening: Gentle isometric and isotonic exercises for the deltoid muscle.
- Scapular Stabilization: Critical for effective deltoid function.
- Activity Restrictions: No lifting objects heavier than 1-2 kg. Continue to avoid sudden movements or activities that stress the repairs.
Phase III: Minimal Protection / Strengthening Phase (Weeks 12-24)
- Goal: Achieve near-full range of motion, progressively increase strength and endurance, improve proprioception.
-
Exercise Focus:
- Progressive Strengthening: Use resistance bands, light weights, and body weight exercises. Focus on rotator cuff (if applicable), deltoid, and scapular stabilizers.
- Eccentric Training: Gradual introduction of eccentric exercises.
- Proprioception & Neuromuscular Control: Balance exercises, closed-chain activities.
- Functional Training: Incorporate movements related to ADLs, work, or recreational activities.
- Activity Restrictions: Gradual return to light functional activities. Avoid heavy lifting, impact activities, and repetitive overhead motions initially.
Phase IV: Return to Activity / Advanced Strengthening Phase (Months 6+)
- Goal: Return to full functional activities, including recreational sports, with maintenance of strength and mobility.
-
Exercise Focus:
- Advanced Strengthening: Sport-specific or work-specific training. High-level resistance exercises.
- Plyometrics: For athletes, if appropriate and cleared by surgeon.
- Maintenance Program: Long-term home exercise program to maintain gains and prevent recurrence of stiffness or weakness.
- Activity Restrictions: Gradual and supervised return to desired activities. High-impact sports or heavy overhead lifting may be permanently restricted or modified depending on the implant type and patient factors. For rTSA, activities requiring internal rotation with extension (e.g., tucking in a shirt) may remain challenging or restricted.
Key Differences Between TSA and rTSA Rehabilitation:
- TSA: Primary focus is protecting the subscapularis repair and restoring anatomical kinematics. External rotation often returns well.
- rTSA: Primary focus is protecting the deltoid and maximizing its function for elevation. Internal rotation and adduction combined are often restricted due to dislocation risk. External rotation is often limited but functional.
Regular communication between the surgeon and physical therapist is vital to customize and optimize rehabilitation based on individual patient progress and intra-operative findings.
Summary of Key Literature / Guidelines
The landscape of shoulder arthroplasty for osteoarthritis has evolved significantly over the past decades, with a robust body of literature guiding current practice. Key themes include evidence supporting the efficacy of arthroplasty, advancements in implant design and surgical techniques, and ongoing research into long-term outcomes and revision strategies.
Efficacy and Outcomes
-
Anatomical Total Shoulder Arthroplasty (TSA):
Long considered the gold standard for glenohumeral osteoarthritis with an intact rotator cuff.
- Long-term survivorship: Studies consistently report excellent pain relief and functional improvement with 10-year implant survivorship rates for anatomical TSA ranging from 85% to 95%, with further reductions at 15-20 years, primarily due to glenoid loosening.
- Glenoid Component: Aseptic glenoid loosening remains the most common reason for revision in TSA. The shift from metal-backed to all-polyethylene, cemented glenoid components has been driven by evidence demonstrating lower loosening rates and improved longevity with the latter.
- Humeral Component: Both cemented and cementless humeral stems show comparable functional outcomes, with stemless designs gaining popularity due to bone-preserving benefits and potential for easier revision, though long-term data is still accumulating.
-
Reverse Total Shoulder Arthroplasty (rTSA):
Revolutionary for managing rotator cuff arthropathy and complex cases.
- Clinical Success: rTSA has demonstrated significant improvements in pain and active elevation in patients with massive, irreparable rotator cuff tears and glenohumeral arthritis, a patient population previously with limited surgical options.
- Complication Profile: While highly effective, rTSA has a distinct complication profile, with higher rates of dislocation, scapular notching, and infection in early series compared to TSA. However, advancements in surgical technique, implant design (e.g., lateralized glenospheres, larger glenospheres, increased inferior overhang), and patient selection have steadily improved outcomes and reduced complication rates.
- Survivorship: 10-year survivorship rates for rTSA are now often comparable to TSA, typically in the 85-90% range, with aseptic loosening and instability being primary modes of failure.
Advancements and Current Trends
- Imaging and Pre-operative Planning: High-resolution CT scans and 3D modeling have revolutionized glenoid planning, particularly for correcting significant retroversion or bone loss. Patient-specific instrumentation (PSI) and 3D-printed guides are becoming more common to improve accuracy of glenoid component placement.
- Glenoid Augmentation: For severe glenoid bone defects and eccentric wear (Walch B2/B3 glenoids), augmented glenoid components (wedge-shaped or stepped designs) or autologous bone grafting are used to restore appropriate glenoid version and inclination, reducing the risk of early loosening and improving clinical outcomes.
- Stemless Humeral Components: These bone-preserving implants are increasingly used in both TSA and rTSA, especially in younger patients with good bone quality. They offer advantages in revision surgery by preserving diaphyseal bone. Long-term data is still being compiled, but early and mid-term results are promising.
- Revision Arthroplasty: The increasing number of primary arthroplasties has led to a rise in revision procedures. The conversion of failed anatomical TSA to rTSA has become a common and effective salvage procedure, particularly for rotator cuff failure or glenoid loosening with compromised soft tissues.
- Dual-Mobility Implants: Emerging in shoulder arthroplasty, these designs aim to improve stability and reduce dislocation rates, particularly in rTSA, by incorporating a polyethylene liner that articulates with both the glenosphere and a larger outer shell that articulates with the humeral component.
- Non-Arthroplasty Options: For younger patients or those with early-stage disease, biological solutions such as osteochondral allografts or autologous chondrocyte implantation for focal defects are being investigated, though their role in widespread OA remains limited. Arthroscopic débridement and capsular release offer symptomatic relief but do not halt disease progression.
Key Guidelines and Recommendations
Professional organizations such as the American Academy of Orthopaedic Surgeons (AAOS) , the American Shoulder and Elbow Surgeons (ASES) , and the Arthroscopy Association of North America (AANA) regularly publish guidelines and position statements based on systematic reviews of the literature. General recommendations include:
- Evidence-Based Decision Making: Surgical decisions should be guided by patient-specific factors, clinical presentation, and radiographic findings, in conjunction with the best available evidence.
- Standardized Outcomes Measures: Consistent use of validated outcome scores (e.g., ASES score, Constant score, UCLA score, visual analog scale for pain) is encouraged for accurate comparison of surgical results across studies and institutions.
- Surgeon Experience: Higher surgeon volume and experience are generally associated with lower complication rates and improved outcomes in shoulder arthroplasty.
- Multidisciplinary Approach: Emphasizing a team approach involving surgeons, anesthesiologists, physical therapists, and medical consultants to optimize patient care from pre-operative planning through post-operative rehabilitation.
In conclusion, shoulder osteoarthritis represents a significant cause of pain and disability, with arthroplasty offering highly effective treatment options. Continued advancements in understanding the biomechanics of the joint, coupled with innovative implant designs and surgical techniques, are consistently improving outcomes and expanding the indications for these complex procedures. Rigorous adherence to evidence-based guidelines and meticulous surgical execution remain paramount for successful patient care.
Clinical & Radiographic Imaging
