Pediatric Fracture Cases: Clinical Presentation, Exam, & Imaging Insights

Key Takeaway
Pediatric fractures, like distal radius, supracondylar humerus, and Salter-Harris type II, are assessed through detailed patient history, mechanism of injury, and thorough clinical examination. This includes vital neurovascular checks, inspection for deformity, palpation for tenderness, and range of motion. Orthogonal radiographs are crucial for diagnosis and classification.
Patient Presentation & History
Case 1: 7-Year-Old with Distal Radius Greenstick Fracture
A 7-year-old male presented to the emergency department after falling off a bicycle onto an outstretched hand. The mechanism was a low-energy direct impact, consistent with an axial load and hyperextension force to the wrist. There were no reported comorbidities. The patient's parents reported immediate pain and visible deformity of the left wrist.
Case 2: 6-Year-Old with Displaced Supracondylar Humerus Fracture
A 6-year-old female presented after falling from monkey bars at a playground, landing on an outstretched hand with an extended elbow. The incident occurred approximately 30 minutes prior to presentation. No significant past medical history. She complained of severe pain in the left elbow and had obvious swelling and deformity.
Case 3: 4-Year-Old with Tibial Shaft Fracture
A 4-year-old male presented with a limp and refusal to bear weight on the right lower extremity after a fall during playful activity. The exact mechanism was unclear, but parents described a twisting injury. No significant comorbidities. He exhibited guarding and crying upon any attempted movement of the leg.
Case 4: 10-Year-Old with Complete Distal Forearm Fracture
A 10-year-old female sustained a direct fall onto her outstretched right hand from a significant height while climbing a tree. She reported immediate, excruciating pain in her right forearm and wrist, with a visible "dinner fork" deformity. She denied any other injuries or significant medical history.
Case 5: 12-Year-Old with Salter-Harris Type II Distal Tibia Fracture
A 12-year-old male presented after a sporting injury during a soccer game, where another player fell on his leg while his foot was planted. He experienced immediate pain and inability to bear weight on the left ankle. He had no known allergies or previous orthopedic injuries.
Clinical Examination
General Principles
Upon initial assessment, all patients were hemodynamically stable. The priority in pediatric trauma is a thorough neurovascular examination prior to any manipulation. This includes assessment of skin color, temperature, capillary refill time, distal pulses (radial, ulnar, dorsalis pedis, posterior tibial), and motor/sensory function of all distal nerves (median, ulnar, radial for upper extremity; peroneal, tibial for lower extremity).
Case 1: Distal Radius Greenstick Fracture
- Inspection: Mild swelling over the dorsal aspect of the left distal forearm and wrist. A subtle apex volar angulation was noted. No open wounds or skin compromise.
- Palpation: Localized tenderness directly over the distal radius metaphysis. No crepitus with gentle motion.
- Range of Motion (ROM): Markedly limited due to pain, especially with wrist flexion and extension.
- Neurological/Vascular: Intact radial pulse, normal capillary refill, and full sensation/motor function in all median, ulnar, and radial nerve distributions.
Case 2: Displaced Supracondylar Humerus Fracture
- Inspection: Significant swelling of the left elbow with a visible S-shaped deformity and posterior displacement of the olecranon. Skin was intact without ecchymosis, but taught due to swelling.
- Palpation: Diffuse tenderness around the distal humerus. No palpable radial pulse initially; capillary refill was sluggish at 3 seconds.
- ROM: Severely restricted and painful. Any attempt at passive motion was met with resistance and guarding.
- Neurological/Vascular: Absent radial pulse. Capillary refill >3 seconds. Initial assessment revealed intact sensation in median, ulnar, and radial distributions, but motor function could not be reliably assessed due to pain. A comprehensive assessment was immediately documented to track potential deterioration.
Case 3: Tibial Shaft Fracture
- Inspection: Mild swelling of the right lower leg, no gross deformity was immediately evident. No open wounds or ecchymosis.
- Palpation: Localized tenderness along the anterior aspect of the mid-diaphysis of the tibia. No crepitus elicited.
- ROM: Pain with attempted ankle and knee motion, reluctance to bear weight.
- Neurological/Vascular: Intact dorsalis pedis and posterior tibial pulses. Capillary refill <2 seconds. Full sensation and motor function in peroneal and tibial nerve distributions.
Case 4: Complete Distal Forearm Fracture
- Inspection: Gross "dinner fork" deformity of the right distal forearm and wrist, characterized by dorsal displacement and apex volar angulation of the distal fragment. Significant swelling and early ecchymosis were present. Skin integrity was maintained.
- Palpation: Exquisite tenderness over the distal radius and ulna. Palpable crepitus with any gentle attempt at manipulation.
- ROM: Severely restricted and painful.
- Neurological/Vascular: Radial pulse was diminished but present. Capillary refill was 2-3 seconds. Sensation was intact, and motor function in median, ulnar, and radial distributions was subjectively intact but difficult to assess due to pain and guarding.
Case 5: Salter-Harris Type II Distal Tibia Fracture
- Inspection: Moderate swelling around the left ankle joint, particularly medially. Mild valgus deformity of the ankle was noted. Skin was intact.
- Palpation: Point tenderness over the distal medial tibia metaphysis and physis. Palpable crepitus with gentle ankle motion.
- ROM: Painful and restricted ankle dorsiflexion and plantarflexion.
- Neurological/Vascular: Intact dorsalis pedis and posterior tibial pulses. Capillary refill <2 seconds. Full sensation and motor function in peroneal and tibial nerve distributions.
Imaging & Diagnostics
General Principles
Standard orthogonal radiographs (AP and lateral views) are the cornerstone of pediatric fracture diagnosis. Oblique views are often helpful for complex fractures or to better delineate fracture patterns. For physeal injuries, comparison views of the contralateral limb may be considered, though often unnecessary if the diagnosis is clear. CT or MRI is rarely indicated for initial diagnosis of uncomplicated pediatric fractures but may be necessary for complex articular involvement, suspected physeal bar formation, or occult injuries.
Imaging for Case 1: Distal Radius Greenstick
-
Radiographic Findings:
AP and lateral radiographs of the left wrist demonstrated a transverse greenstick fracture of the distal metaphysis of the radius, approximately 2 cm proximal to the physis. The fracture involved the dorsal cortex, with an intact volar cortex, resulting in approximately 10 degrees of apex volar angulation. There was no significant displacement or rotational deformity. The distal ulna and its physis were unremarkable.
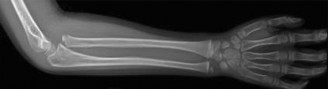
- Classification: Greenstick fracture of the distal radius.
Imaging for Case 2: Displaced Supracondylar Humerus Fracture
-
Radiographic Findings:
AP and lateral radiographs of the left elbow revealed a significantly displaced supracondylar humerus fracture. On the lateral view, the anterior humeral line passed anterior to the capitellum, and Baumann's angle was significantly decreased (less than 45 degrees), indicating severe extension-type displacement with posterior and medial angulation of the distal fragment relative to the proximal shaft. The fracture line was oblique, originating from the olecranon fossa posteriorly and extending anteriorly through the coronoid fossa.

- Classification: Gartland Type III supracondylar humerus fracture (completely displaced). Given the neurovascular compromise (absent radial pulse), this also qualifies as a pulseless supracondylar fracture.
Imaging for Case 3: Tibial Shaft Fracture
-
Radiographic Findings:
AP and lateral radiographs of the right tibia and fibula demonstrated a non-displaced, spiral oblique fracture of the mid-diaphysis of the tibia. The fracture pattern was stable, with no significant angulation or rotational deformity. The fibula was intact.

- Classification: Spiral oblique tibial shaft fracture. Often seen as a "toddler's fracture" in this age group, though the mechanism here was more direct.
Imaging for Case 4: Complete Distal Forearm Fracture
-
Radiographic Findings:
AP and lateral radiographs of the right forearm and wrist revealed a complete, significantly displaced, and angulated transverse fracture of the distal metaphysis of the radius, approximately 2.5 cm proximal to the physis. There was substantial dorsal displacement of the distal fragment, with approximately 35 degrees of apex volar angulation. The distal ulna also demonstrated a transverse fracture through its metaphysis, with minimal displacement but significant shortening relative to the radius.

- Classification: Complete, displaced distal radius and ulna metaphyseal fractures.
Imaging for Case 5: Salter-Harris Type II Distal Tibia Fracture
-
Radiographic Findings:
AP and lateral radiographs of the left ankle showed a Salter-Harris Type II fracture of the distal tibia. The fracture line extended transversely through the physis (growth plate) and then obliquely proximally through the metaphysis, creating a triangular metaphyseal fragment, known as the "Thurston Holland" fragment, on the medial aspect. There was approximately 5 mm of medial displacement and mild valgus angulation of the epiphysis relative to the tibial shaft. The fibula was intact.
- Classification: Salter-Harris Type II fracture of the distal tibia.
Differential Diagnosis
A comprehensive differential diagnosis is crucial in pediatric orthopedics, particularly given the varying presentation of injuries and the unique properties of the pediatric skeleton.
| Feature / Condition | Acute Fracture | Physeal Injury (e.g., Salter-Harris) | Sprain/Ligamentous Injury | Stress Fracture | Non-Accidental Trauma (NAT) |
|---|---|---|---|---|---|
| Pain Onset | Acute, immediate, often severe | Acute, immediate, often severe, localized to physis | Acute, immediate, often localized to joint/ligament | Gradual, insidious, worse with activity | Variable, often inconsistent with reported mechanism |
| Deformity | Common, especially with displaced fractures | May have subtle deformity or swelling | Rare, gross deformity suggests dislocation/avulsion | Rare | May have multiple injuries in various stages of healing, inconsistent with age/development |
| Swelling | Common, localized to fracture site | Common, localized to physeal region | Common, localized to joint capsule | Localized, often subtle | Multiple sites, disproportionate to history |
| Crepitus | Often palpable with displaced fractures | May be present with displacement | Absent | Absent | Absent, but may reveal other signs like bruising patterns |
| Weight-bearing/ROM | Refusal to bear weight; painful, limited ROM | Refusal to bear weight; painful, limited ROM | Painful ROM, especially specific ligament tests | Pain with activity, relieved by rest; full ROM at rest | Avoidance of movement, guarding, unusual pain response |
| X-ray Findings | Fracture line, cortical disruption, displacement | Fracture line through physis, metaphyseal/epiphyseal involvement (Salter-Harris types) | Normal bone architecture; possibly soft tissue swelling | Periosteal reaction, cortical thickening, faint lucency | Metaphyseal corner fractures, rib fractures, long bone shaft fractures, varying ages of healing |
| Mechanism | Clear, often high-energy trauma | Clear, often high-energy trauma | Twisting, hyperextension, direct impact | Repetitive microtrauma, sudden increase in activity | Inconsistent, implausible, or vague history for injury severity |
| Associated Injuries | May have soft tissue, neurovascular | May have soft tissue, neurovascular | May have associated avulsion fracture | Rare | Multiple injuries, head trauma, abdominal trauma, burns |
| Special Considerations | High remodeling potential, growth plate concerns | High risk for growth disturbance (e.g., physeal arrest) | May mask physeal injury ("ligamentous injury" in child is often physeal) | Common in young athletes, activity modification | Mandatory reporting, comprehensive social work/child protection services involvement |
Surgical Decision Making & Classification
General Principles in Pediatric Fracture Management
Pediatric fracture management prioritizes non-operative approaches whenever possible, capitalizing on the immense remodeling potential of the growing skeleton. However, specific criteria for acceptable angulation, rotation, and translation exist, which vary by age, fracture location, and proximity to physes. The overriding goals are to achieve a stable reduction, prevent growth disturbance, avoid complications (e.g., compartment syndrome, neurovascular compromise), and restore function. Operative intervention is reserved for irreducible fractures, open fractures, unstable reductions, neurovascular compromise, polytrauma, or articular involvement that necessitates anatomical reduction.
Case 1: Distal Radius Greenstick Fracture
- Decision: Non-operative management with closed reduction and casting.
- Rationale: Greenstick fractures, by definition, involve an intact cortex, which often provides inherent stability. The apex volar angulation of 10 degrees is well within acceptable limits for a 7-year-old distal radius fracture, which has excellent remodeling potential. Surgical intervention is rarely indicated unless angulation exceeds acceptable thresholds (typically 20-25 degrees in this age group, depending on skeletal maturity) or if there is significant rotational deformity.
Case 2: Displaced Supracondylar Humerus Fracture
- Decision: Urgent closed reduction and percutaneous pinning (CRPP) followed by a long arm cast.
- Classification: Gartland Type III (completely displaced) with neurovascular compromise (absent radial pulse).
- Rationale: Gartland Type III supracondylar fractures are unstable and carry a high risk of neurovascular injury and compartment syndrome. The presence of a pulseless limb, even if initially warm and well-perfused (pink pulseless hand), mandates immediate reduction to restore perfusion. If pulse does not return after closed reduction, further intervention such as open reduction and exploration of the brachial artery may be necessary. Definitive surgical fixation with K-wires provides stable immobilization, allowing for early pain control and preventing further displacement or complications.
Case 3: Tibial Shaft Fracture
- Decision: Non-operative management with closed reduction and long leg cast application.
- Rationale: The spiral oblique fracture of the mid-diaphysis of the tibia was non-displaced and stable. In a 4-year-old, the remodeling potential of the tibia is excellent. Acceptable angulation is generally up to 10-15 degrees and 10-15 degrees of rotational malunion can also remodel. Given the stability and lack of significant displacement, closed reduction was not strictly required to correct deformity, but a cast was necessary for immobilization. Surgical intervention (e.g., intramedullary nailing) would be considered for unstable, highly displaced, or open fractures, or in older, heavier children where casting alone may not maintain reduction.
Case 4: Complete Distal Forearm Fracture
- Decision: Closed reduction and long arm casting.
- Rationale: The significant dorsal displacement and apex volar angulation (35 degrees) exceeded acceptable limits for a 10-year-old. While remodeling potential exists, a malunion of this magnitude could lead to functional deficits and cosmetic deformity. A stable closed reduction, followed by immobilization in a long arm cast, was indicated to correct the deformity and allow for healing in an acceptable position. Unstable reductions, inability to achieve acceptable alignment, or persistent neurovascular compromise after reduction would necessitate operative intervention (e.g., CRPP or ORIF).
Case 5: Salter-Harris Type II Distal Tibia Fracture
- Decision: Closed reduction and long leg casting.
- Rationale: Salter-Harris Type II fractures, particularly of the distal tibia, require anatomical or near-anatomical reduction to minimize the risk of physeal bar formation and subsequent growth disturbance. The 5 mm of displacement and valgus angulation exceeded acceptable limits. While the Thurston Holland fragment helps prevent direct compression of the physis, persistent displacement can lead to complications. Surgical intervention (CRPP) would be considered if closed reduction failed or if the fracture was persistently unstable after reduction.
Surgical Technique / Intervention
General Principles of Pediatric Fracture Reduction
Effective pediatric fracture reduction requires adequate analgesia, muscle relaxation, and often sedation or general anesthesia. The principles involve applying sustained traction, disimpacting the fracture fragments, exaggerating the deformity, and then reversing the deforming forces to achieve reduction. Careful, controlled maneuvers are paramount to avoid further injury, particularly to adjacent physes or neurovascular structures. Post-reduction radiographs are essential to confirm adequate alignment and assess for any iatrogenic displacement during cast application.
Closed Reduction Technique: Distal Forearm Fractures (Cases 1 & 4)
- Anesthesia: Intravenous sedation (e.g., ketamine, propofol) or regional block (hematoma block with lidocaine) is often sufficient. General anesthesia may be preferred for more complex or highly displaced fractures in younger, uncooperative children.
- Positioning: Supine position with the affected arm abducted, elbow flexed to 90 degrees. An assistant provides counter-traction at the elbow.
-
Reduction Maneuver:
- Traction: Sustained longitudinal traction is applied to the hand (often using finger traps) to disimpact the fracture fragments and restore length. This traction is maintained for several minutes to achieve muscle relaxation.
- Exaggeration/Correction of Angulation: For apex volar angulation (common in distal radius fractures), the deformity is initially exaggerated (further dorsiflexion) to unlock the fragments, followed by direct pressure over the dorsal aspect of the distal fragment while simultaneously applying volar pressure to the shaft, correcting the apex volar angulation. Conversely, for apex dorsal angulation, the deformity is exaggerated with volar flexion, followed by dorsal pressure on the distal fragment.
- Rotation: Pronation or supination of the forearm may be required to correct rotational deformities. For distal radius fractures, an initially pronated position is typically used, with reduction completed and cast applied in neutral to slight pronation.
- Casting: A well-molded, three-point fixation cast (long arm for unstable reductions or very young children, short arm for stable fractures) is applied. The cast should extend from just below the axilla (or elbow crease for short arm) to the metacarpal heads, ensuring proper padding over bony prominences. The elbow is typically flexed to 90 degrees for long arm casts, with the forearm in neutral rotation to slight pronation.
- Post-Reduction Imaging: AP and lateral radiographs are immediately obtained to confirm acceptable reduction. Key parameters to assess include angulation, translation, and rotation (e.g., maintaining the distal radial physis parallel to the proximal articular surface).
Closed Reduction Technique: Supracondylar Humerus (Case 2 - Gartland Type III)
- Anesthesia: General anesthesia is mandatory due to pain and the need for complete muscle relaxation.
- Positioning: Supine with the affected arm on a hand table. An assistant provides counter-traction to the upper arm. Image intensifier (fluoroscopy) is essential.
-
Reduction Maneuver (usually performed under fluoroscopy):
- Traction: Sustained longitudinal traction is applied to the forearm with the elbow gently extended to disengage the fragments.
- Correction of Medial/Lateral Displacement: While maintaining traction, varus or valgus force is applied to correct any coronal plane displacement.
- Correction of Rotation: The forearm is typically pronated to derotate the distal fragment, which is often internally rotated. This also tightens the medial soft tissues, aiding stability.
- Flexion & Posterior Push: The elbow is gently flexed while maintaining traction and pronation. Simultaneously, a thumb is placed on the olecranon to push the distal fragment anteriorly, correcting the posterior displacement.
-
Surgical Fixation (Percutaneous Pinning):
-
Pin Placement:
Typically involves two lateral K-wires or a cross-pin configuration (one medial, one lateral).
- Lateral Entry: Two diverging pins are inserted through the lateral epicondylar condyle, crossing the fracture site into the medial and lateral columns of the proximal humerus. Care must be taken to avoid the ulnar nerve.
- Cross-Pinning: A medial pin is inserted proximal to the medial epicondyle, avoiding the ulnar nerve by palpating it and potentially flexing the elbow to 110-120 degrees during insertion. A lateral pin is then inserted similarly. Cross-pinning generally provides greater rotational stability but carries a higher risk of ulnar nerve injury.
- Check for Stability & Neurovascular Status: After pinning, stability is assessed, and neurovascular status is re-checked. Pins are bent and cut beneath the skin or left exposed for later removal.
-
Pin Placement:
Typically involves two lateral K-wires or a cross-pin configuration (one medial, one lateral).
- Casting: A long arm cast is applied with the elbow flexed to approximately 60-90 degrees, forearm neutral to pronated, to further stabilize the reduction.
- Post-Operative Imaging: AP and lateral radiographs are taken to confirm pin placement and fracture alignment.
Closed Reduction Technique: Tibial Shaft (Case 3)
- Anesthesia: Conscious sedation or general anesthesia.
- Positioning: Supine with the knee flexed, or prone. An assistant provides counter-traction at the groin or thigh.
- Reduction Maneuver: Sustained longitudinal traction is applied to the foot or ankle to restore length and correct any overriding. Gentle direct molding over the fracture site can correct angulation. Rotational alignment is crucial and is assessed by comparing the foot position to the patella.
- Casting: A well-molded long leg cast is applied, extending from the proximal thigh to the toes, with the knee flexed to 15-20 degrees and the ankle in neutral dorsiflexion. For stable non-displaced fractures like a toddler's fracture, reduction maneuvers may not be necessary, only immobilization.
- Post-Reduction Imaging: AP and lateral radiographs of the tibia (including knee and ankle) confirm reduction and cast fit.
Closed Reduction Technique: Salter-Harris Type II Distal Tibia (Case 5)
- Anesthesia: General anesthesia is typically preferred for optimal muscle relaxation and a single, gentle reduction attempt.
- Positioning: Supine with the knee flexed. An assistant provides counter-traction at the thigh.
-
Reduction Maneuver:
- Traction: Gentle, sustained longitudinal traction is applied to the foot to disengage the fracture fragments.
- Correction of Deformity: For the typical valgus and posterior displacement, the ankle is gently dorsiflexed, and direct medial pressure is applied to the distal fragment while an adduction (varus) force is applied to correct the valgus. The Thurston Holland fragment should remain attached to the periosteum, acting as a hinge. Avoid forceful or repeated manipulations, as this can damage the physis.
- Casting: A well-molded long leg cast is applied, extending from the proximal thigh to the toes, with the knee flexed to 15-20 degrees and the ankle in neutral dorsiflexion. For particularly unstable reductions, the cast may need to incorporate greater molding or be extended above the knee for initial weeks.
- Post-Reduction Imaging: AP and lateral radiographs of the ankle (and potentially tibia for length) are immediately obtained to confirm anatomical or near-anatomical reduction. Any remaining gap or persistent displacement of >2 mm in the physeal region may warrant consideration for repeat reduction or CRPP.
Post-Operative Protocol & Rehabilitation
General Principles
Post-operative or post-reduction care focuses on maintaining reduction, monitoring for complications, and ensuring appropriate healing and return to function. Pediatric patients typically have rapid healing rates.
- Initial Immobilization: Fractures are typically immobilized in casts for 3-6 weeks, depending on age, fracture type, and location. Younger children heal faster.
- Neurovascular Monitoring: Strict vigilance for compartment syndrome, especially in supracondylar humerus and tibial shaft fractures, is critical in the first 24-48 hours. Regular checks of pulses, capillary refill, sensation, and motor function are performed.
- Pain Management: Appropriate analgesia is provided.
- Cast Care: Parents are educated on proper cast care, including elevating the limb, observing for signs of complications (swelling, discoloration, pain, numbness, foul odor), and keeping the cast dry.
-
Follow-up:
- Initial Check (1-2 weeks): Clinical assessment and radiographs to confirm maintained reduction as initial swelling resolves.
- Mid-Course Check (3-4 weeks): Clinical and radiographic assessment to evaluate early callus formation.
- Cast Removal (6-8 weeks): Clinical and radiographic assessment of union.
-
Rehabilitation:
- Post-Cast Removal: Most pediatric patients regain full ROM and strength spontaneously within weeks after cast removal without formal physical therapy, especially with non-articular fractures. Gentle active ROM exercises are encouraged.
- Weight Bearing: Gradual return to weight-bearing as tolerated once union is evident and discomfort subsides.
- Return to Activity: Return to full activity, including sports, is typically allowed once pain-free, full ROM is achieved, and radiographic healing is confirmed, usually 2-3 months post-injury.
- Physeal Monitoring (for Salter-Harris fractures): For all physeal injuries, clinical and radiographic follow-up for 6-12 months (or until skeletal maturity) is crucial to detect any signs of growth disturbance (e.g., physeal arrest, angular deformity, leg length discrepancy).
Case Specific Protocols
- Case 1 (Distal Radius Greenstick): Short arm cast for 4 weeks. Removal, followed by gentle ROM exercises. Return to activity typically 6-8 weeks.
- Case 2 (Supracondylar Humerus): Pins-in-place long arm cast for 3-4 weeks. Pin removal in clinic. Gentle active ROM (flexion/extension, pronation/supination) encouraged, avoiding passive stretching. Return to activity 8-12 weeks. Close monitoring for cubitus varus or valgus and neurological recovery.
- Case 3 (Tibial Shaft Fracture): Long leg cast for 6-8 weeks. Non-weight bearing initially, then progressive weight-bearing in the cast as comfort allows. Cast removal, followed by gradual return to full activity.
- Case 4 (Complete Distal Forearm Fracture): Long arm cast for 6 weeks, then potentially a short arm cast for an additional 2-3 weeks depending on healing. Close neurovascular monitoring. Cast removal, followed by active ROM. Return to activity 10-12 weeks.
- Case 5 (Salter-Harris Type II Distal Tibia): Long leg cast for 6 weeks, non-weight bearing for the first 3 weeks, then protected weight-bearing in the cast. Cast removal. Regular clinical and radiographic follow-up for 6-12 months to monitor for physeal growth disturbances.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- Remodeling Potential: Pediatric bones have remarkable remodeling capacity, particularly in younger children (<10 years), fractures distant from the physis, and fractures in the plane of motion. This allows for greater tolerance of angulation than in adults.
- Neurovascular Assessment: Always perform and document a meticulous neurovascular examination before and after any manipulation or cast application. Any changes warrant immediate investigation and potential intervention. Pulselessness is a surgical emergency until proven otherwise.
- Compartment Syndrome: High index of suspicion for compartment syndrome, especially with high-energy injuries, forearm, and tibial fractures. Early recognition and fasciotomy are limb-saving. Clinical signs include pain out of proportion, pain with passive stretch, paresthesia, pallor, paralysis, and pulselessness (late).
- Physeal Injury Awareness: Always evaluate radiographs for physeal involvement. A "sprained ankle" in a child is often a Salter-Harris Type I or II physeal injury. Anatomical reduction is critical for Salter-Harris Type III and IV fractures, and important for Type II, to minimize growth disturbance.
- Acceptable Limits of Deformity: Understand the age- and location-specific acceptable limits for angulation and rotation. Excessive deformity, especially rotation or angulation in the plane of joint motion, may not remodel sufficiently.
- Single Reduction Attempt: For physeal injuries, aim for a single, gentle, and accurate reduction attempt under adequate anesthesia to minimize additional physeal damage.
- Thorough Casting Technique: Apply well-padded, well-molded casts with appropriate three-point fixation. Ensure freedom of adjacent joints (e.g., full elbow extension in a short arm cast, full finger flexion in a wrist cast). Monitor for cast-related complications.
- Non-Accidental Trauma (NAT): Maintain a high index of suspicion for NAT, especially with inconsistent history, multiple fractures in various healing stages, or injuries inappropriate for the child's developmental stage. Specific fracture patterns (e.g., metaphyseal corner fractures, posterior rib fractures) are highly suspicious.
Pitfalls
- Inadequate Reduction: Accepting an unstable or malaligned reduction outside acceptable limits can lead to functional impairment, chronic pain, or re-operation.
- Missed Neurovascular Injury: Failure to recognize or act on neurovascular compromise (e.g., pulseless pink hand after supracondylar fracture).
- Tight Casts: Casts applied too tightly can cause compartment syndrome or pressure sores. Always check for proper padding and fit.
- Missed Physeal Injury: Misdiagnosing a Salter-Harris I or II injury as a "sprain," leading to inadequate treatment and potential growth disturbance.
- Failure to Monitor Growth: Neglecting long-term follow-up for physeal injuries, resulting in delayed diagnosis of growth arrest or angular deformity.
- Poor Parental Education: Inadequate instruction to parents regarding cast care, warning signs of complications, and follow-up importance.
- Over-reliance on Remodeling: Assuming all deformities will remodel, especially in older children or with rotational malunion, can lead to poor outcomes. Rotational deformities remodel poorly.
- Iatrogenic Physeal Damage: Repeated forceful reduction attempts or improper pinning techniques can directly damage the physis, leading to growth arrest or angular deformity.
- Failure to Detect Rotational Malunion: Rotational assessment is clinically challenging but crucial, as it remodels poorly. Always compare to the contralateral limb.
- Incomplete Radiographs: Not obtaining appropriate views (e.g., oblique views for certain fractures) or not including the joint above and below, leading to missed injuries.
Clinical & Radiographic Imaging

