Pediatric Lateral Condyle Fracture: The Critical Role of Internal Oblique Radiographs
Key Takeaway
The internal oblique radiograph is crucial for diagnosing pediatric lateral condyle fractures because standard AP/lateral views often obscure subtle displacement or articular involvement due to developing ossification centers. This specialized view clearly delineates the fracture line, extent of displacement, rotation, and articular surface involvement, enabling accurate Salter-Harris classification and guiding optimal management decisions.
Patient Presentation & History
A 7-year-old male presented to the emergency department following a fall from a monkey bar apparatus at school. He reports falling directly onto his outstretched right hand with his elbow in extension. The patient immediately experienced acute pain, swelling, and refusal to move the right elbow. There was no reported loss of consciousness or associated head, neck, or other limb injuries. His parents reported no significant past medical history, no known allergies, and he was up-to-date on immunizations. No history of bleeding disorders or bone fragility was noted. He is right-hand dominant.
Clinical Examination
Upon initial assessment, the patient was alert, cooperative, and in moderate distress due to pain.
- Inspection: Marked diffuse swelling was evident over the right elbow, predominantly on the lateral aspect, with subtle ecchymosis. There was no obvious gross deformity, skin tenting, or open wounds. The elbow was held in a position of slight flexion (approximately 30 degrees).
- Palpation: Significant tenderness was elicited over the lateral epicondyle and supracondylar region of the distal humerus. Palpation of the radial head and olecranon was also painful but less localized. No crepitus was appreciated without causing undue discomfort.
- Range of Motion (ROM): Active ROM was severely restricted and painful. Passive ROM was attempted gently, revealing an arc of flexion from approximately 30 degrees to 80 degrees, with significant pain at the end ranges. Supination and pronation were similarly painful and limited.
- Neurological Assessment: A thorough neurological examination revealed intact motor and sensory function in the radial, ulnar, and median nerve distributions. Specifically, the patient could extend the wrist and fingers (radial nerve), abduct and adduct the fingers (ulnar nerve), and oppose the thumb and flex the wrist/fingers (median nerve). No paresthesias or dysesthesias were reported.
- Vascular Assessment: The radial and ulnar pulses were bilaterally palpable, strong, and symmetrical. Capillary refill was brisk (<2 seconds) in all digits of the right hand. The limb was warm and well-perfused. No compartment syndrome signs were present.
Imaging & Diagnostics
Initial radiographic evaluation of the right elbow consisted of standard anterior-posterior (AP) and lateral views.
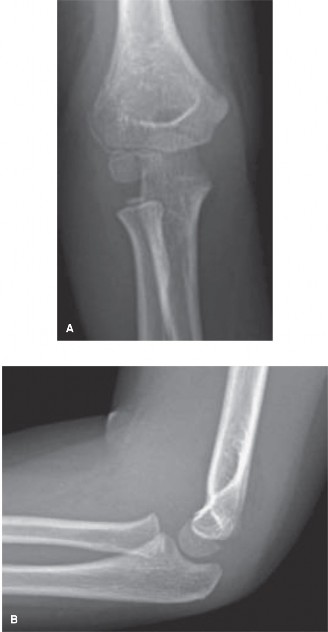
- AP View: The AP radiograph demonstrated diffuse soft tissue swelling and a subtle lucency suggesting a fracture line originating from the lateral metaphysis of the distal humerus. However, the extent of displacement and articular involvement, particularly the physeal extension, was not clearly delineated due to superimposition of the distal humeral epiphysis and the developing ossification centers. The lucency appeared to extend towards the capitellum.
- Lateral View: The lateral view revealed an anterior fat pad sign, indicating an intra-articular effusion. The fracture line was difficult to discern precisely on this view, but the capitellum and lateral condyle appeared to be slightly displaced posteriorly relative to the humeral shaft. However, the true degree of displacement, rotation, and articular fragment size remained equivocal.
Given the clinical suspicion of a lateral condyle fracture and the ambiguous findings on standard views, an internal oblique radiograph of the elbow was obtained. This view is crucial in pediatric elbow trauma, particularly for assessing lateral condyle fractures, as it projects the capitellum and trochlea more clearly, revealing the true extent of the fracture line and any subtle displacement or rotation that might be missed on standard projections.
Internal Oblique View: The internal oblique view unequivocally demonstrated a Salter-Harris Type IV fracture of the lateral condyle of the humerus. The fracture line was clearly visible, extending from the lateral metaphysis, through the physis, and into the articular surface of the capitellum. There was an estimated 3-4 mm of displacement of the articular fragment relative to the metaphysis, accompanied by subtle but definite rotation of the fragment. The fragment included a significant portion of the capitellum, indicating articular involvement. The internal oblique view was paramount in confirming the diagnosis, classifying the fracture, and guiding surgical decision-making.
Figure 1: Initial AP/Lateral radiographs demonstrating subtle findings. Note the joint effusion (positive fat pad sign on lateral view) and an indistinct lucency on the AP view suggestive of a lateral condyle injury, but the true extent of displacement and articular involvement remains unclear.

Figure 2: Internal oblique view of the elbow clearly delineating a Salter-Harris Type IV lateral condyle fracture with approximately 4mm of displacement and rotation. The fracture line extends through the physis and into the articular surface of the capitellum.
- Further Imaging: While the internal oblique view provided sufficient detail for this case, in more complex or equivocal situations, a computed tomography (CT) scan with 3D reconstructions might be considered to further delineate articular involvement, fragment size, and displacement, particularly for pre-operative planning. Magnetic resonance imaging (MRI) is rarely indicated acutely but could be considered for suspected ligamentous injuries, physeal bar formation, or avascular necrosis concerns post-operatively. For this patient, the clarity offered by the internal oblique view rendered advanced imaging unnecessary.
- Templating: Given the nature of a pediatric lateral condyle fracture, detailed templating for fixation implants is generally not performed in the same manner as adult periarticular fractures. The primary goal is anatomical reduction and stable fixation with K-wires. Pre-operative planning focuses on the approach, expected reduction maneuvers, and appropriate K-wire sizes (typically 1.6 mm or 2.0 mm).
Differential Diagnosis
The acute presentation of elbow pain and swelling in a child following trauma warrants a broad differential diagnosis. Key considerations include:
| Feature | Lateral Condyle Fracture (Salter-Harris IV) - Our Case | Supracondylar Humeral Fracture | Medial Epicondyle Avulsion Fracture |
|---|---|---|---|
| Etiology/MOI | Varus stress or direct trauma (fall onto outstretched hand with elbow in extension and forearm supination). Fragment avulsed by common extensor origin. | Fall onto outstretched hand (FOOSH) with elbow hyperextended (extension type - ~95%), or direct blow to posterior elbow (flexion type - ~5%). | Valgus stress with elbow extension (fall or traction injury), often associated with elbow dislocation. Avulsion by common flexor origin or medial collateral ligament. |
| Clinical Features | Localized tenderness over lateral condyle. Swelling, ecchymosis lateral aspect. Pain with forearm pronation/supination. Elbow often held in flexion. | Diffuse swelling, S-shaped deformity (extension type). Potential for neurovascular compromise (median, radial nerve, brachial artery). Pallor, pulselessness, paresthesias (Volkmann's ischemia risk). | Tenderness over medial epicondyle. Swelling, ecchymosis medial aspect. Pain with valgus stress. Often significant pain with wrist flexion against resistance. Ulnar nerve symptoms possible. |
| Radiographic Features (Standard Views) | Subtle fracture line often obscured. Fat pad sign present. AP: Lateral metaphyseal lucency possibly extending to capitellum. Lateral: Posterior displacement of capitellum may be seen, but difficult to assess true displacement/rotation. | AP: Transverse fracture line across supracondylar region. Lateral: Displaced distal fragment, loss of Baumann's angle (extension type), posterior displacement of proximal fragment (flexion type). | AP: Avulsed fragment seen medial to humeral metaphysis, often displaced distally. Lateral: Fragment displaced anteriorly/inferiorly. May be entrapped in joint. |
| Radiographic Features (Special Views) | Internal oblique view is KEY. Clearly delineates physeal involvement, articular extension, true displacement, and rotation of the fragment. Crucial for classification (Milch I vs. II, Salter-Harris type). | Oblique views may aid in identifying subtle fracture lines or displacement. Stress views are not typically indicated. | May require AP/Lateral with gentle stress or comparison views if dislocation spontaneously reduced. Oblique views may show better displacement. |
| Management Principles | <2mm displacement: Non-operative (long arm cast). >2mm displacement/rotation/articular involvement: ORIF with K-wires. Aim for anatomical reduction. | Gartland I: Non-operative (long arm cast). Gartland II: Closed reduction & percutaneous pinning (CRPP). Gartland III/IV: CRPP vs. ORIF for irreducible fractures. Urgent neurovascular assessment. | Minimally displaced (<5mm): Non-operative (long arm cast). Displaced (>5-10mm), entrapped in joint, elbow instability, or ulnar nerve symptoms: ORIF with K-wires or screws. |
Surgical Decision Making & Classification
The patient's internal oblique radiograph confirmed a Salter-Harris Type IV lateral condyle fracture with 3-4 mm of displacement and rotation involving the articular surface.
Lateral condyle fractures are typically classified by
Milch's classification
based on the relationship of the fracture line to the trochlear groove:
*
Milch Type I:
Fracture line lateral to the trochlear groove, involving only the capitellum. The medial epicondylar ridge remains intact. This is often an intra-articular fracture involving the capitellum alone.
*
Milch Type II:
Fracture line extends into the trochlear groove, involving both the capitellum and a portion of the trochlea. This is also an intra-articular fracture.
A more clinically practical classification for surgical decision-making considers displacement, often using the
Jakob classification
:
*
Stage I:
Non-displaced (<2 mm).
*
Stage II:
Displaced (2 mm to 4 mm) but without significant rotation or distal migration.
*
Stage III:
Severely displaced (>4 mm) or significantly rotated/proximal migration.
Our patient's fracture, with 3-4 mm of displacement and definite rotation, falls into the Jakob Stage II-III equivalent and is clearly a Salter-Harris Type IV , indicating physeal and articular involvement.
Decision for Operative Intervention:
Displaced lateral condyle fractures in children carry significant risks of complications with non-operative management, including:
1.
Nonunion:
The most common serious complication, occurring in up to 30% of displaced fractures treated non-operatively. The synovial fluid acts as a barrier to healing, and shear forces across the fracture site prevent callus formation.
2.
Cubitus Valgus Deformity:
Often resulting from a nonunion where the lateral condyle fails to unite and undergoes growth arrest, leading to overgrowth of the medial side of the distal humerus. This can cause a tardy ulnar nerve palsy years later.
3.
Cubitus Varus Deformity:
Less common, but can result from premature physeal closure or malunion.
4.
Growth Arrest/Deformity:
Due to physeal injury (Salter-Harris Type IV).
5.
Avascular Necrosis (AVN) of the Capitellum:
Though rare, especially with prompt reduction.
Given the 3-4 mm displacement and rotational component, surgical intervention was deemed mandatory to achieve anatomical reduction, stable fixation, and minimize the risk of nonunion and subsequent deformity. The threshold for operative fixation is generally considered to be >2 mm of displacement.
Surgical Technique / Intervention
The goal of surgery was anatomical reduction of the lateral condyle fracture and stable internal fixation to allow for healing and preserve future elbow function and growth.
- Pre-operative Planning: Review of all radiographs, particularly the internal oblique view, to understand fracture morphology, displacement, and articular involvement. Discussion with parents regarding the risks and benefits, including the potential for re-operation for pin removal or complications.
- Anesthesia & Positioning: The patient was placed under general anesthesia. A high arm tourniquet was applied to the right upper extremity. The patient was positioned supine on the operating table with the right arm draped free onto a hand table to allow for full range of motion and sterile preparation.
- Surgical Approach: A standard lateral approach to the distal humerus was utilized. A 5-6 cm curvilinear incision was made centered over the lateral epicondyle, extending proximally along the lateral supracondylar ridge. The incision was deepened through subcutaneous tissue. The common extensor origin was carefully incised or elevated anteriorly, exposing the fracture site. Care was taken to avoid injury to the radial nerve branches laterally.
- Fracture Identification & Debridement: The hematoma within the fracture site was meticulously irrigated and debrided to allow clear visualization of the fracture surfaces, the physeal plate, and the articular surface. Any interposed soft tissue (e.g., periosteum, capsule) preventing reduction was removed. The fracture line was identified, extending through the metaphysis, physis, and capitellar articular cartilage.
-
Reduction Techniques:
- Direct Visualization: The displaced lateral condyle fragment was gently manipulated under direct visualization. K-wires were used as joysticks inserted into the fragment to aid in reduction.
- Traction and Rotation: Gentle longitudinal traction was applied to the forearm while simultaneously applying direct pressure to the displaced fragment to correct both the lateral and rotational displacement. The goal was to achieve anatomical alignment of the articular surface and the metaphyseal fracture line.
- Verification: Reduction was confirmed visually by assessing the anatomical restoration of the articular surface and the alignment of the metaphyseal cortical step. Intraoperative fluoroscopy (AP, lateral, and internal oblique views) was used to confirm anatomical reduction and assess stability.
-
Fixation Construct:
- K-wire Placement: Once anatomical reduction was achieved and held manually, two 1.6 mm smooth K-wires were inserted percutaneously. The entry points were planned to ensure adequate purchase in both the fragment and the humeral shaft, avoiding the olecranon fossa.
- Divergent Wires: The first K-wire was typically started from the lateral epicondyle, aiming proximally and medially into the medial column of the humerus, across the physis. The second K-wire was inserted from the lateral epicondyle, aiming proximally and slightly more anterior or posterior, crossing the physis into the humeral shaft, divergent from the first pin. This divergent configuration provides superior rotational stability.
- Physeal Avoidance (Consideration): While crossing the physis is unavoidable in Salter-Harris Type IV fractures, smooth K-wires minimize growth plate damage. The trajectory was carefully controlled to achieve maximum purchase. In older children approaching physeal closure, cannulated screws might be considered for larger fragments. For this 7-year-old, K-wires were the preferred method.
- Stability Check: After pin insertion, the elbow was put through a gentle range of motion under fluoroscopy to confirm stability of the fixation and ensure no impingement of the K-wires. The pin ends were bent and cut approximately 1 cm outside the skin and capped.
- Closure: The common extensor origin was approximated if necessary. The subcutaneous tissue was closed with absorbable sutures, and the skin was closed with sterile adhesive strips or interrupted non-absorbable sutures. A sterile dressing was applied over the pin sites. A well-padded long arm cast was applied with the elbow in 90 degrees of flexion and neutral forearm rotation.
Post-Operative Protocol & Rehabilitation
The post-operative protocol for pediatric lateral condyle fractures managed with K-wire fixation aims to protect the reduction, allow for fracture healing, and facilitate a gradual return to full function while monitoring for complications.
-
Immediately Post-Op (Days 0-7):
- Immobilization: Long arm cast with the elbow in 90 degrees of flexion and neutral forearm rotation. This position minimizes stress on the fracture site.
- Elevation & Ice: Continuous limb elevation and intermittent cryotherapy to reduce swelling.
- Pain Management: Age-appropriate analgesia.
- Neurovascular Monitoring: Close monitoring of neurovascular status (pulses, capillary refill, sensation, motor function) for the first 24-48 hours.
- Pin Site Care: Parents instructed on strict pin site care to prevent infection.
-
Weeks 1-3:
- Cast & Pin Care: Continue long arm cast. Regular monitoring of pin sites for signs of infection (erythema, discharge).
- Radiographic Follow-up: Weekly or bi-weekly radiographs (AP, lateral, oblique views) to confirm maintenance of reduction and assess early callus formation.
-
Weeks 4-6:
- K-wire Removal: Typically, K-wires are removed in the clinic under local anesthesia or light sedation around 4-6 weeks post-operatively, once radiographic evidence of early healing (bridging callus) is observed and the fracture site is clinically non-tender.
- Continued Immobilization (Optional): Depending on the stability post-pin removal and radiographic healing, a removable brace or short arm cast may be applied for another 1-2 weeks, or the patient may transition to gentle range of motion. For this patient, a gentle transition to active ROM was planned.
-
Weeks 6-12 (Rehabilitation Phase):
- Gradual Range of Motion: Initiate gentle, active-assisted and then active range of motion exercises for flexion, extension, pronation, and supination. Passive stretching is generally avoided initially to prevent undue stress on the healing physis and to minimize the risk of heterotopic ossification or physeal disturbance.
- Activity Restrictions: Avoid weight-bearing, lifting, pushing, pulling, and contact sports. Light activities of daily living are permissible.
- Physical Therapy (as needed): Formal physical therapy may be considered for children with persistent stiffness, though most pediatric patients regain excellent motion spontaneously. Focus on play-based exercises to encourage natural movement.
-
Months 3-6:
- Progression of Activities: Gradual return to full activities, including light sports, once full pain-free range of motion is achieved and radiographs confirm solid union.
- Return to Contact Sports: Typically allowed at 4-6 months, depending on clinical and radiographic healing and muscle strength.
- Follow-up: Clinical and radiographic follow-up at 6 months and 1 year post-injury to monitor for late complications such as cubitus valgus deformity, growth disturbance, or tardy ulnar nerve palsy.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- High Index of Suspicion: Always suspect a pediatric elbow fracture with any fall onto an outstretched hand, even if initial AP/Lateral radiographs are subtle. Positive fat pad signs are a strong indicator of intra-articular injury.
- The Internal Oblique View is Non-Negotiable: For suspected lateral condyle fractures, the internal oblique view is absolutely critical. It provides the most accurate assessment of displacement, rotation, and articular involvement, which are often underestimated or missed on standard AP/Lateral views. It is paramount for correct classification and surgical decision-making.
- Anatomical Reduction is Paramount: For displaced lateral condyle fractures, anatomical reduction, particularly of the articular surface and physis, is crucial to prevent nonunion, growth arrest, and cubitus valgus deformity.
- Smooth K-wires are Standard: Smooth K-wires are the preferred fixation method as they allow for continued physeal growth with minimal impingement. Divergent pinning offers excellent rotational stability.
- Beware of Interposed Soft Tissue: Inability to achieve anatomical reduction often indicates interposed periosteum or capsule within the fracture gap. Open reduction and direct visualization are necessary to remove these impediments.
- Monitor Neurovascular Status Diligently: Although less common than with supracondylar fractures, always perform and document a thorough neurovascular assessment pre- and post-operatively.
- Risk of Nonunion: Synovial fluid present at the fracture site creates an unfavorable environment for healing. Coupled with shear forces, this significantly increases the risk of nonunion for displaced fractures treated non-operatively.
- Late Complications: Even with successful initial management, monitor for late complications such as cubitus valgus (due to nonunion or lateral physeal arrest), cubitus varus (due to medial physeal overgrowth or malunion), and tardy ulnar nerve palsy.
Pitfalls
- Missed Diagnosis: Failing to obtain or correctly interpret the internal oblique view can lead to a missed or underestimated displaced lateral condyle fracture, resulting in delayed treatment and increased risk of nonunion.
- Inadequate Reduction: Accepting anything less than anatomical reduction of the articular surface and metaphyseal cortical step significantly increases the risk of nonunion, malunion, and long-term deformity (e.g., cubitus valgus). Intraoperative fluoroscopy and direct visualization are key.
- Poor Fixation: Inadequate K-wire purchase, parallel rather than divergent wires, or insufficient number of pins can lead to loss of reduction and fixation failure.
- Pin Tract Infection: A common complication if pin site care is suboptimal. Can lead to osteomyelitis if not managed aggressively.
- Premature Pin Removal: Removing pins before adequate radiographic and clinical healing can result in loss of reduction or re-fracture.
- Aggressive Rehabilitation: Overly aggressive passive stretching or forced range of motion in the early post-operative period can disrupt the healing fracture, lead to heterotopic ossification, or cause physeal injury.
- Failure to Follow Up: Loss to follow-up, especially in the long term, means missing late-onset complications like cubitus valgus and tardy ulnar nerve palsy, which can have significant functional consequences if not addressed.
- Ignoring Subtle Rotation: Even seemingly minor rotational displacement can lead to long-term functional deficits and cosmetic deformity, highlighting why the oblique view and anatomical reduction are critical.
