Pediatric Glenohumeral Instability: Diagnosis, Anatomy & Management
Key Takeaway
Pediatric glenohumeral instability is symptomatic shoulder laxity or dislocation in skeletally immature patients, particularly adolescents. It's a complex challenge with high recurrence rates due to factors like ligamentous laxity and specific lesions. Diagnosis requires a thorough physical exam, focusing on apprehension signs, and understanding the unique developing anatomy and biomechanics.
Introduction & Epidemiology
Pediatric shoulder pain presents a complex diagnostic and therapeutic challenge for the orthopedic surgeon. Unlike adult presentations, pediatric shoulder pathologies are diverse, ranging from physeal injuries and inflammatory conditions to traumatic instability. A precise diagnosis hinges upon a thorough history, a meticulous physical examination – particularly focusing on specific diagnostic signs elicited by arm maneuvers – and appropriate imaging modalities. Among the various etiologies, traumatic glenohumeral instability in the adolescent population warrants particular attention due to its high incidence, significant recurrence rates, and potential for long-term functional deficits if inadequately managed.
The epidemiology of shoulder instability in the skeletally immature patient population reveals distinct characteristics. While rare in pre-adolescents, the incidence of glenohumeral instability significantly increases during adolescence, particularly in the 10-20 year age group. Contact and collision sports, as well as overhead throwing activities, are major risk factors. Studies consistently report higher recurrence rates following a primary traumatic anterior glenohumeral dislocation in adolescents compared to adults. Recurrence rates can exceed 70% in individuals under 20 years of age, especially males involved in high-risk sports. This elevated recurrence is attributed to a combination of factors, including greater generalized ligamentous laxity, higher activity levels, and potentially less robust healing potential of the capsulolabral complex in the immature skeleton. The "vital diagnostic sign with the arm" often manifests as an apprehension response during external rotation and abduction, a crucial indicator of glenohumeral laxity or instability.
Surgical Anatomy & Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the pediatric shoulder is paramount for effective management of instability. The developing skeletal architecture and unique soft tissue properties dictate distinct considerations.
Skeletal Anatomy
The pediatric shoulder girdle comprises the scapula, clavicle, and proximal humerus.
*
Proximal Humerus
: The developing proximal humeral physis is a critical consideration. Salter-Harris type I or II physeal fractures are common traumatic injuries, and their healing potential generally excellent. However, significant displacements can lead to angular deformities or growth arrest. The greater and lesser tuberosities, sites of rotator cuff attachment, ossify separately and merge.
*
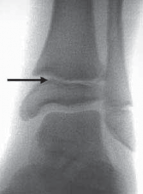
Glenoid
: The glenoid fossa is relatively shallow, with its depth primarily augmented by the labrum. Glenoid retroversion or hypoplasia can predispose to instability. The scapular physis, located around the glenoid, closes in late adolescence, and avulsion fractures (bony Bankart) can involve this physis.
*
Clavicle
: Provides a strut for shoulder stability and muscle attachment. Clavicle fractures are common in childhood but typically managed non-operatively.
Soft Tissue Anatomy
The static and dynamic stabilizers of the glenohumeral joint are critical for maintaining stability.
*
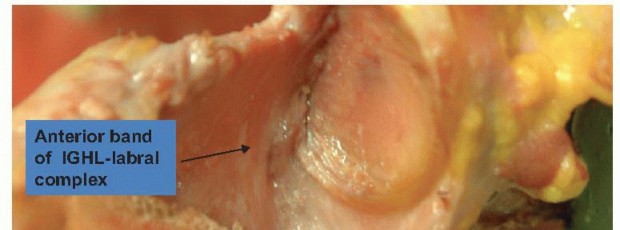
Capsulolabral Complex
: The glenoid labrum is a fibrocartilaginous ring that deepens the glenoid fossa. Its attachment to the glenoid rim is crucial. Traumatic anterior dislocation frequently results in a
Bankart lesion
, an avulsion of the anteroinferior labrum and capsule from the glenoid rim. Other lesions include
Perthes lesion
(an anterior labral avulsion with an intact scapular periosteal sleeve),
ALPSA (Anterior Labral Periosteal Sleeve Avulsion)
lesion, and
HAGL (Humeral Avulsion of the Glenohumeral Ligament)
lesion.
*
Glenohumeral Ligaments (GHLs)
: These capsular thickenings are primary static stabilizers.
*
Inferior Glenohumeral Ligament (IGHL)
: The most important static stabilizer, particularly when the arm is abducted and externally rotated. It consists of anterior and posterior bands.
*
Middle Glenohumeral Ligament (MGHL)
: Variable in presence and size, contributes to anterior stability in mid-ranges of motion.
*
Superior Glenohumeral Ligament (SGHL)
: Prevents inferior translation of the humeral head when the arm is adducted.
*
Rotator Cuff
: The dynamic stabilizers include the supraspinatus, infraspinatus, teres minor, and subscapularis muscles. These muscles dynamically compress the humeral head into the glenoid, particularly during overhead activities. While rotator cuff tears are rare in skeletally immature patients, tendinopathy or musculotendinous injuries can occur.
*
Long Head of Biceps Tendon
: Contributes to superior and anterior stability and humeral head depression.
Biomechanics of Stability
Glenohumeral stability is achieved through a delicate balance of static and dynamic factors.
*
Static Stabilizers
: Include the articular congruity (glenoid depth and version), glenoid labrum, joint capsule, and glenohumeral ligaments. The vacuum effect of the joint also contributes.
*
Dynamic Stabilizers
: Primarily the rotator cuff muscles, which create a concavity-compression effect, and the scapular periscapular muscles, which orient the glenoid to optimize humeral head centration.
Pathoanatomic lesions, such as a Bankart lesion (soft tissue) or a bony Bankart lesion (osseous avulsion from the glenoid rim), directly compromise the static anterior stabilizers, leading to recurrent instability. Similarly, a
Hill-Sachs lesion
, an impaction fracture on the posterior-superior aspect of the humeral head, can engage the anterior glenoid rim during abduction and external rotation, further contributing to recurrent dislocation.
Indications & Contraindications
The decision-making process for operative versus non-operative management of pediatric shoulder instability is multifaceted, influenced by patient age, activity level, number of dislocation episodes, presence of bony lesions, and overall ligamentous laxity.
Non-Operative Indications
- First-time traumatic dislocation : Particularly in patients with lower activity demands or without significant associated bony or soft tissue lesions. Immobilization in a sling for 3-4 weeks, followed by a structured physical therapy program focusing on rotator cuff and scapular stabilization.
- Pre-adolescent age : Younger children generally have higher healing potential for capsulolabral structures, and their lower activity levels often lead to less shear stress.
- Generalized ligamentous laxity : In some cases, primary management focuses on strengthening periscapular and rotator cuff musculature.
- Minimal or no glenoid bone loss : Less than 15% glenoid bone loss without an engaging Hill-Sachs lesion.
- Patient or family preference : After a thorough discussion of the high recurrence rates in the pediatric population.
Operative Indications
- Recurrent instability : Two or more documented dislocations or subluxations, despite adequate non-operative management. This is the most common indication.
- Significant glenoid bone loss : Typically >15-20% of the inferior glenoid width, predisposing to recurrent instability and often requiring osseous augmentation procedures.
- Engaging Hill-Sachs lesion : A humeral head defect that engages the anterior glenoid rim during range of motion, particularly in abduction and external rotation, which can be identified by dynamic testing or on imaging.
- Failure of conservative management : Persistent symptoms of apprehension, pain, or functional limitation despite a dedicated rehabilitation program.
- High-demand athletes : Competitive athletes, particularly those involved in collision or overhead sports, where the risk of recurrence and re-injury is high and can impact career longevity.
- Specific lesion types : Large labral tears that are clearly displaced, HAGL lesions, or significant bony Bankart lesions.
- Skeletally mature adolescents : As they approach skeletal maturity, their recurrence rates align more closely with young adults, favoring early surgical intervention to prevent further episodes and potential cumulative damage.
Contraindications
- Active infection : Local or systemic infection must be controlled prior to elective surgery.
- Severe medical comorbidities : Conditions that preclude safe anesthesia and surgical intervention.
- Non-compliance : Patients unwilling or unable to adhere to rigorous post-operative rehabilitation protocols, which are critical for successful outcomes.
- Poor bone quality : May affect anchor fixation, though less common in this population.
| Indication Category | Operative Management | Non-Operative Management |
|---|---|---|
| Recurrence | Two or more documented dislocations/subluxations | First-time dislocation (consideration for observation) |
| Bone Loss | Significant glenoid bone loss (>15-20%) or engaging Hill-Sachs | Minimal glenoid bone loss (<15%) |
| Activity Level | High-demand, competitive athletes (collision, overhead) | Low-demand individuals |
| Lesion Type | Large, displaced Bankart; Bony Bankart; HAGL lesions | Small, non-displaced labral injury |
| Response to PT | Failure of comprehensive rehabilitation | Resolution of symptoms with rehabilitation |
| Skeletal Maturity | Skeletally mature or nearing maturity | Pre-adolescent (often higher threshold for surgery) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to ensure optimal outcomes and minimize complications in pediatric shoulder instability surgery.
Pre-Operative Planning
-
Comprehensive History and Physical Examination
:
- History : Detailed account of the injury mechanism (e.g., forced abduction-external rotation), number and frequency of dislocation/subluxation events, associated pain, numbness, weakness, and previous treatments. Ascertain activity level and athletic aspirations. Inquire about generalized ligamentous laxity (e.g., Beighton score).
-
Physical Examination
:
- Inspection : Swelling, ecchymosis, muscle atrophy.
- Palpation : Tenderness over the glenohumeral joint or surrounding structures.
- Range of Motion : Active and passive ROM, noting any limitations or apprehension.
-
Stability Testing
:
- Apprehension Test : The "vital diagnostic sign with the arm" for anterior instability. Arm abducted to 90 degrees, elbow flexed to 90 degrees, and slowly externally rotated. A positive test elicits a sensation of impending dislocation or muscle guarding.
- Relocation Test (Jobe's Test) : Performed immediately after a positive apprehension test. A posterior force is applied to the humeral head, alleviating apprehension.
- Load and Shift Test : Performed with the patient supine, applying axial compression (load) and then translating the humeral head anteriorly and posteriorly (shift) to assess glenohumeral translation.
- Sulcus Sign : Assesses inferior laxity by applying inferior traction to the arm.
- Neurological Examination : Crucial to assess axillary nerve function (deltoid contraction, sensation over lateral arm), musculocutaneous nerve, and brachial plexus integrity.
-
This image depicts a typical physical examination maneuver for shoulder instability, such as the apprehension test, where the examiner is applying an external rotation force to the abducted arm, eliciting an apprehension response from the patient.
-
Imaging Studies
:
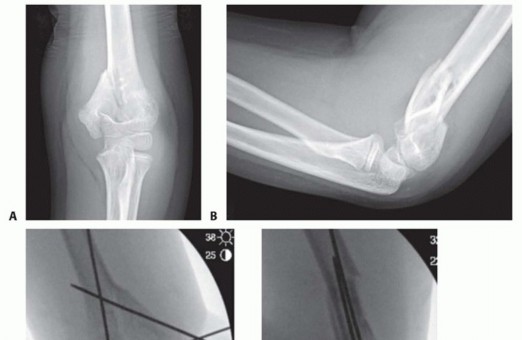
- Plain Radiographs : Standard series includes AP, scapular Y, and axillary views. These help identify bony Bankart lesions, glenoid rim fractures, Hill-Sachs lesions, and rule out other pathologies like physeal fractures. An acute anterior dislocation will show the humeral head displaced anteriorly and inferiorly relative to the glenoid.
- Magnetic Resonance Imaging (MRI) / Magnetic Resonance Arthrography (MRA) : The gold standard for evaluating soft tissue pathology. MRA provides enhanced visualization of the labrum, capsule, and glenohumeral ligaments, identifying Bankart, ALPSA, Perthes, or HAGL lesions. It also detects rotator cuff pathology and assesses for Hill-Sachs lesions.
- Computed Tomography (CT) / 3D CT Reconstruction : Essential for precise quantification of glenoid bone loss and evaluation of the size and engagement of Hill-Sachs lesions. This information is critical for determining if a bone augmentation procedure (e.g., Latarjet or glenoid reconstruction) is necessary.
Patient Positioning
The choice between beach chair and lateral decubitus positioning depends on surgeon preference and the anticipated scope of the procedure.
-
Beach Chair Position
:
- Advantages : More anatomical orientation for arthroscopic portals, easier conversion to an open procedure if needed, comfortable for the patient, and allows for simultaneous evaluation of the shoulder and ipsilateral elbow/wrist if indicated.
- Setup : Patient is semi-recumbent (30-70 degrees of trunk elevation). The head is secured and slightly rotated away from the operative shoulder. The operative arm is free-draped, allowing full range of motion. A beanbag or specialized shoulder chair is used for stabilization. Pressure points (occiput, sacrum, heels) must be padded. The ipsilateral leg should be slightly flexed. Ensure the entire shoulder girdle is visible and accessible.
- Anesthesia : General endotracheal anesthesia is typical. An interscalene brachial plexus block can be added pre-operatively for post-operative pain control.
-
Lateral Decubitus Position
:
- Advantages : Provides greater traction, potentially easier for posterior capsule work, and can be advantageous for obese patients.
- Setup : Patient is positioned laterally with the operative shoulder superior. The torso is secured with chest and hip restraints. An axillary roll is placed under the contralateral axilla to prevent brachial plexus compression. The operative arm is suspended in balanced suspension with approximately 10-15 pounds of traction, typically abducted to 70 degrees and forward flexed to 30 degrees. This provides distraction for arthroscopic visualization.
- Anesthesia : Similar to beach chair, general anesthesia with or without an interscalene block.
Prior to incision, a final time-out confirming patient identity, procedure, and site is performed. The operative field is prepared with antiseptic solution (e.g., chlorhexidine gluconate) and sterile draped to include the entire shoulder, upper arm, and axilla.
Detailed Surgical Approach / Technique
The primary surgical technique for recurrent traumatic anterior glenohumeral instability in adolescents is arthroscopic Bankart repair, aiming to re-establish the anterior capsulolabral bumper. In cases with significant bone loss, open bone augmentation procedures (e.g., Latarjet) may be indicated.
Arthroscopic Bankart Repair (Capsulolabral Repair)
The goal is to anatomically reattach the avulsed anteroinferior labrum and capsule to the glenoid rim.
-
Diagnostic Arthroscopy and Portal Placement
:
- Posterior Portal : Typically the initial viewing portal. Located 2 cm inferior and 1 cm medial to the posterior-lateral acromial corner. A standard 30-degree arthroscope is inserted to perform a systematic diagnostic evaluation of the glenohumeral joint (rotator cuff, biceps tendon, glenoid cartilage, humeral head, and labral pathology).
- Anterior-Superior Portal : Located at the rotator interval. Used for instrumentation and anchor placement. Often established using an outside-in technique, approximately 1-2 cm medial to the anterolateral acromial corner.
- Anterior-Inferior Working Portal : Often established via an outside-in technique, approximately 1-2 cm lateral to the coracoid process, for optimal access to the anteroinferior glenoid and labrum. This portal is crucial for anchor placement and suture retrieval.
-
Labral Preparation and Glenoid Decortication
:
- The avulsed anteroinferior labrum and capsule are identified. A shaver or electrocautery device is used to debride any frayed tissue from the labrum and to mobilize it adequately, ensuring it can be anatomically reduced to the glenoid rim without tension.
- The anterior glenoid rim, where the labrum has avulsed, is lightly decorticated using a burr or shaver. This exposes cancellous bone, promoting a "bleeding bed" for enhanced capsulolabral healing to the glenoid. Care must be taken to avoid over-resection of the glenoid rim.
-
Anchor Placement
:
- The number and type of suture anchors (bioabsorbable, PEEK, all-suture) depend on surgeon preference and the extent of the lesion. Typically, 3 to 5 anchors are placed along the anterior glenoid rim.
- The first anchor is usually placed at the 5 o'clock position (right shoulder) or 7 o'clock position (left shoulder), inferior to the bare area of the glenoid. Subsequent anchors are placed superiorly, spaced approximately 1 cm apart, extending to the 3 o'clock or 9 o'clock position.
- A drill guide or cannulated obturator is used to create pilot holes for the anchors. The anchors are then inserted, ensuring adequate purchase in the glenoid bone.
-
Suture Management and Capsulolabral Repair
:
- Each anchor contains one or two high-strength sutures. A suture passer (e.g., birdbeak, SutureLasso) is used to retrieve the sutures.
- The suture passer is introduced through a working portal, passed through the anteroinferior labrum and capsule, and the suture is retrieved. The goal is to capture sufficient tissue (labrum, capsule, and ideally, the medialized periosteal sleeve) to create a robust repair.
- Knot Tying : Non-sliding or sliding knots are tied arthroscopically, sequentially from inferior to superior. Each knot is carefully tensioned to reduce the labrum and capsule anatomically to the glenoid rim, creating a firm anterior bumper. The repair should not overtighten the shoulder, which could restrict external rotation.
-
Assessment of Stability
:
- After all sutures are tied, the stability of the glenohumeral joint is dynamically assessed arthroscopically under direct visualization. The arm is moved through a range of motion, particularly into abduction and external rotation, to ensure the repair is stable and no apprehension is present. The humeral head should remain well-centered on the glenoid.
Management of Bony Lesions
- Glenoid Bone Loss : If pre-operative imaging reveals significant glenoid bone loss (typically >20-25%), an arthroscopic Bankart repair alone may be insufficient. In these cases, open Latarjet procedure (coracoid transfer) or iliac crest bone graft augmentation may be indicated to restore glenoid concavity and stability. The Latarjet procedure involves transferring the coracoid process with the conjoint tendon to the anterior glenoid neck, augmenting the glenoid bone stock and creating a "sling" effect from the conjoint tendon. This is typically an open procedure.
- Engaging Hill-Sachs Lesion : For significant and engaging Hill-Sachs lesions, an arthroscopic remplissage (filling in) procedure may be performed concurrently with Bankart repair. This involves capsulotenodesis of the posterior capsule and infraspinatus tendon into the Hill-Sachs defect, effectively converting an "engaging" lesion to a "non-engaging" one by filling the defect and preventing engagement with the glenoid rim.
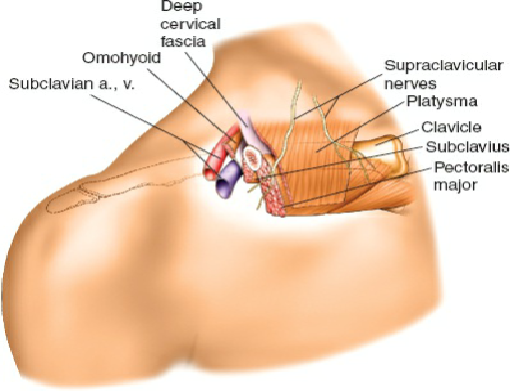
Internervous Planes & Critical Structures
During portal placement and subsequent dissection, careful attention to neurovascular structures is paramount.
*
Axillary Nerve
: Most at risk with inferior portals and during excessive traction. It courses inferior to the glenohumeral joint, approximately 2-3 cm from the glenoid rim.
*
Musculocutaneous Nerve
: At risk with lateral portals and during drilling for Latarjet.
*
Brachial Plexus
: Can be injured by prolonged or excessive traction, particularly in the lateral decubitus position.
*
Subscapular Artery and Nerve
: Can be injured during aggressive inferior capsular releases.
The decision for arthroscopic versus open procedure, and whether to include bone augmentation, is made pre-operatively based on patient-specific factors and imaging findings. For most pediatric/adolescent traumatic anterior instability cases without significant bone loss, arthroscopic Bankart repair remains the workhorse procedure.
Complications & Management
Despite advancements in surgical techniques, complications can occur following operative intervention for pediatric shoulder instability. Understanding their incidence and appropriate salvage strategies is crucial.
Common Complications
-
Recurrence of Instability
:
- Incidence : Still the most common complication, albeit significantly lower than with non-operative management. Rates vary from 5-20% depending on patient demographics (age, activity level), surgical technique, and follow-up duration. Higher rates are seen in younger, male, high-demand athletes.
- Management : Thorough investigation with physical exam and imaging (MRI/CT) to identify the cause (e.g., failure of healing, progressive bone loss, new trauma). Revision surgery, potentially with a more robust open procedure like Latarjet if significant bone loss is present or previous soft tissue repair failed.
-
Stiffness / Loss of Motion
:
- Incidence : 5-15%, often involving loss of external rotation. Can be due to overtightening of the capsule, inadequate rehabilitation, or adhesive capsulitis (rare in children).
- Management : Intensive physical therapy with a focus on regaining lost motion. If persistent and debilitating after 6-12 months, consider arthroscopic capsular release or manipulation under anesthesia. Prevention through appropriate intra-operative capsular tensioning and early, structured rehabilitation is key.
-
Nerve Injury
:
- Incidence : Rare (<1-2%). The axillary nerve is most commonly at risk, especially during inferior portal placement, deep drilling for anchors, or excessive traction. Musculocutaneous nerve injury is less common but can occur, particularly with certain open approaches or Latarjet.
- Management : Intraoperative recognition and avoidance are primary. Post-operatively, if a nerve injury is suspected (e.g., deltoid weakness, lateral arm numbness for axillary nerve), careful neurological exam, EMG/NCS studies. Most neurapraxias resolve spontaneously. Persistent deficits may warrant nerve exploration and repair.
-
Infection
:
- Incidence : Very low (<1%), similar to other arthroscopic procedures.
- Management : Superficial infections may respond to oral antibiotics. Deep glenohumeral joint infection requires emergent surgical irrigation and debridement, along with intravenous antibiotics tailored to culture results.
-
Hardware-Related Issues
:
- Incidence : Varies with anchor type. Bioabsorbable anchors can sometimes cause synovitis, sterile effusions, or osteolysis, although current generations are less problematic. Prominent metal anchors can cause pain or chondral damage.
- Management : Symptomatic hardware may require arthroscopic or open removal. Sterile effusions from bioabsorbable anchors usually resolve spontaneously but may require aspiration.
-
Chondral or Articular Cartilage Damage
:
- Incidence : Can occur during anchor placement, suture passage, or from instrument scuffing. Less common but significant in the long term.
- Management : Minor defects are typically observed. Larger defects, if symptomatic, may require microfracture or cartilage restoration procedures, though these are rarely indicated acutely for this etiology.
-
Pain
:
- Incidence : Varied. Persistent pain can be due to residual instability, stiffness, hardware irritation, or other unidentified pathology.
- Management : Address the underlying cause. Rule out nerve irritation, tendinopathy, or residual instability. Targeted physical therapy, anti-inflammatory medication, or in select cases, hardware removal.
| Complication | Incidence (%) | Salvage Strategy |
|---|---|---|
| Recurrence of Instability | 5-20 | Revision Bankart, Latarjet, Glenoid Augmentation |
| Stiffness/Loss of Motion | 5-15 | Intensive PT, MUA, Arthroscopic Capsular Release |
| Axillary Nerve Injury | <1-2 | Observation (neurapraxia), EMG/NCS, Nerve Exploration |
| Infection (Deep GHJ) | <1 | I&D, IV Antibiotics |
| Hardware Irritation/Synovitis | 1-5 | Observation, NSAIDs, Hardware Removal (if symptomatic) |
| Chondral Damage | <1 | Observation, Symptomatic Management, Cartilage Procedures |
| Persistent Pain (Unexplained) | Varies | Rule out other pathologies, targeted PT, Hardware Removal |
Post-Operative Rehabilitation Protocols
A well-structured and compliant post-operative rehabilitation protocol is paramount for optimizing outcomes and minimizing recurrence after shoulder stabilization surgery in pediatric patients. The protocol is typically divided into three phases, progressing from protection to full return to sport.
Phase I: Protection and Early Motion (Weeks 0-6)
- Goals : Protect the surgical repair, minimize pain and swelling, prevent stiffness, and initiate early passive motion.
- Immobilization : Arm placed in a sling for 4-6 weeks, with or without an abduction pillow, depending on surgeon preference and the extent of the repair. The sling is typically removed for hygiene and exercises only.
-
Exercises
:
- Pendulum exercises : Gentle, gravity-assisted swings of the arm.
-
Passive Range of Motion (PROM)
:
- Forward flexion : To 90-120 degrees (avoiding excessive abduction).
- External rotation : Limited to neutral or 0-15 degrees with the arm adducted at the side, to protect the anterior repair.
- Internal rotation : To the abdomen.
- Scapular stabilization : Gentle isometric exercises for the scapular protractors and retractors (e.g., scapular squeezes).
- Elbow, wrist, hand exercises : Maintain range of motion and strength in the distal limb.
- Restrictions : No active range of motion of the shoulder. No lifting, pushing, pulling, or sudden movements. Avoid resisted internal and external rotation. Avoid external rotation past neutral.
Phase II: Gradual Return to Motion and Strengthening (Weeks 6-12)
- Goals : Gradually restore full range of motion, initiate active strengthening, and improve neuromuscular control.
- Discontinuation of Sling : Typically around 6 weeks, as guided by clinical progress.
-
Exercises
:
- Active-Assisted Range of Motion (AAROM) and Active Range of Motion (AROM) : Progressively increase AAROM and AROM for all planes, with careful monitoring of pain and apprehension.
-
Strengthening
:
- Isometric exercises : For rotator cuff (internal/external rotation, abduction, adduction) and deltoid, performed without resistance initially.
- Light resistance exercises : Using elastic bands or light weights for rotator cuff and scapular stabilizers (e.g., band external rotation, rows, push-ups against a wall).
- Biceps and triceps strengthening .
- Proprioception and Neuromuscular Control : Begin closed-chain exercises (e.g., weight shifts on a stable surface), rhythmic stabilization drills.
- Restrictions : Avoid overhead activities, aggressive stretching into external rotation and abduction. No heavy lifting or contact sports.
Phase III: Advanced Strengthening and Return to Sport (Weeks 12-24+)
- Goals : Maximize strength, power, endurance, and sport-specific function; gradually return to full activity and sport.
-
Exercises
:
- Progressive Resistance Exercises : Increase intensity and complexity of exercises for all major shoulder muscle groups.
- Plyometrics : For overhead athletes, begin with low-intensity plyometric drills (e.g., medicine ball throws) to restore power and dynamic stability.
- Sport-Specific Drills : Gradually introduce activities specific to the patient's sport, starting with controlled movements and progressing to higher intensity.
- Interval Throwing Programs : For throwing athletes, a structured interval throwing program is initiated, progressing in distance and intensity.
-
Return to Sport Criteria
: This is a multi-factorial decision, typically not before 4-6 months post-operatively, and often longer (6-9 months) for overhead or contact sports. Criteria include:
- Full, pain-free range of motion comparable to the contralateral side.
- Strength at least 90% of the contralateral side (often assessed with isokinetic testing).
- Absence of apprehension during sport-specific movements.
- Completion of sport-specific training without symptoms.
- Psychological readiness.
- Long-term Maintenance : Continued emphasis on rotator cuff and scapular strengthening exercises to maintain stability and prevent recurrence.
Patient compliance with the rehabilitation program, along with close communication between the surgeon, physical therapist, and patient/family, is crucial for achieving optimal long-term outcomes and minimizing the high recurrence rates seen in this population.
Summary of Key Literature / Guidelines
The management of pediatric and adolescent glenohumeral instability has evolved significantly, driven by an increased understanding of its unique epidemiology and pathoanatomy. Key literature and professional guidelines emphasize tailored approaches recognizing the distinct challenges of the developing skeleton and high activity levels.
-
High Recurrence Rates in Adolescents : Numerous studies consistently highlight the significantly higher recurrence rates following a primary traumatic anterior glenohumeral dislocation in adolescents (under 20 years old) compared to adults. Historically, non-operative management of primary dislocations in this cohort led to recurrence rates often exceeding 70%, particularly in males participating in contact or overhead sports (e.g., Kirkley et al., 1998; Hovelius et al., 2008 ). This stark difference strongly influences the threshold for surgical intervention.
-
Early Surgical Intervention :
- The high recurrence rates and potential for cumulative damage (e.g., progressive glenoid bone loss, Hill-Sachs engagement, chondral injury) have led to a paradigm shift towards considering early surgical stabilization for high-risk adolescent patients after a primary dislocation, especially competitive athletes.
- Meta-analyses and systematic reviews (e.g., Olds et al., 2015 ) have demonstrated superior outcomes and lower recurrence rates with early surgical stabilization compared to conservative management in young, active individuals.
- While consensus on all primary dislocations is not universal, a strong argument exists for operative management in adolescents with risk factors such as male gender, participation in collision sports, or evidence of significant Bankart lesions on MRI.
-
Arthroscopic vs. Open Repair :
- For the majority of soft tissue Bankart lesions without significant bone loss, arthroscopic Bankart repair has become the standard of care due to its minimally invasive nature, excellent visualization, and comparable efficacy to open repair in terms of recurrence rates in selected patient populations (e.g., Boileau et al., 2006 ).
- However, open repair may still be preferred in specific complex cases, revision surgeries, or when significant bone loss necessitates a Latarjet procedure.
-
Role of Bone Augmentation (Latarjet/Remplissage) :
- The importance of addressing osseous defects (glenoid bone loss and engaging Hill-Sachs lesions) is well-established. Pre-operative CT scans are critical for quantifying these lesions.
- Glenoid bone loss >15-20% is a strong predictor of failure after isolated soft tissue Bankart repair. In these cases, open Latarjet or other bone block procedures are indicated to restore glenoid concavity and provide a biological sling effect, significantly reducing recurrence rates (e.g., Burkhart and De Beer, 2004 ).
- For engaging Hill-Sachs lesions, arthroscopic remplissage (capsulotenodesis into the defect) performed concurrently with Bankart repair can reduce recurrence rates by preventing engagement (e.g., Provencher et al., 2010 ).
-
Rehabilitation :
- Standardized, progressive rehabilitation protocols are crucial, emphasizing initial protection of the repair, gradual restoration of motion, and progressive strengthening of the rotator cuff and periscapular stabilizers.
- Return to sport criteria are stringent, typically requiring full range of motion, near-normal strength, and absence of apprehension, usually not before 4-6 months for non-contact sports and 6-9 months for collision/overhead sports.
-
AAOS Clinical Practice Guidelines : The American Academy of Orthopaedic Surgeons (AAOS) provides clinical practice guidelines for the management of glenohumeral instability. While not specific to pediatric patients alone, they offer strong recommendations on imaging, physical exam, and indications for surgical intervention that can be extrapolated and adapted for the adolescent population, emphasizing individualized treatment based on risk factors and patient goals.
In summary, the management of pediatric shoulder instability, particularly in adolescents, requires a nuanced approach. The high recurrence rates in this age group, coupled with the potential for progressive articular damage, often favors a more aggressive, early surgical stabilization strategy in high-risk patients with traumatic anterior instability. Arthroscopic Bankart repair remains the cornerstone for soft tissue lesions, but meticulous pre-operative planning to identify and address significant bony defects is critical for successful long-term outcomes.
You Might Also Like