Pediatric Sacral Fracture & Neurological Deficit: A Detailed Trauma Case Study
Key Takeaway
Pediatric sacral fractures with neurological deficits present with severe pain, lower extremity weakness, perineal numbness, and absent sacral reflexes. Diagnosis involves thorough clinical neurological examination, CT for fracture morphology, and MRI to confirm nerve root compression, edema, or hemorrhage, all crucial for guiding surgical decompression and stabilization planning.
Can You Spot Sacral Nerve Fibers in This Pediatric Trauma Case?
Patient Presentation & History
An 8-year-old male presented to the emergency department following a high-energy motor vehicle vs. pedestrian incident. The patient was struck by a car traveling approximately 40 km/h, sustaining direct trauma to the posterior pelvis and sacral region. He was conscious and alert on arrival but in significant pain, rated 9/10 on a visual analogue scale (appropriate for age). Initial assessment revealed a Glasgow Coma Scale (GCS) of 15, stable hemodynamics (BP 105/65 mmHg, HR 98 bpm, RR 20 rpm), and no immediate life-threatening injuries according to ATLS protocol. However, he complained of severe pain in his lower back and bilateral buttock regions, with inability to move his lower extremities or tolerate any weight-bearing. Specifically, he reported numbness in the perineal region and difficulty with micturition since the accident, though the latter was challenging to ascertain definitively given the acute pain and stress. There was no reported history of pre-existing neurological deficits, spinal deformities, or coagulopathies. The patient’s past medical history was otherwise unremarkable, and he was up-to-date on all vaccinations. His family history was non-contributory to skeletal or neurological conditions. The mechanism suggested a significant axial loading and shear component to the sacropelvic region.
Clinical Examination
Upon focused secondary survey, the patient was found to have tenderness to palpation over the entire sacrum and bilateral sacroiliac joints. Inspection revealed significant soft tissue swelling and ecchymosis over the gluteal regions and posterior sacrum. A superficial abrasion was noted centrally over the S2-S4 dermatomes. There was no obvious open wound or signs of degloving injury. Palpation of the anterior superior iliac spines, iliac crests, and pubic symphysis revealed no instability or significant tenderness, suggesting the primary injury was confined to the posterior pelvic ring.
Neurological examination of the lower extremities was critical and challenging due to pain. Gross motor function demonstrated profound weakness in bilateral hip extension and abduction (Grade 2/5) and hip flexion (Grade 3/5). Knee extension (L3/L4) and ankle dorsiflexion (L4/L5) were 4/5 bilaterally. However, ankle plantarflexion (S1/S2) was significantly impaired, rated 2/5 bilaterally, as was toe flexion (S2/S3), also 2/5. Sensory examination revealed decreased sensation to light touch and pinprick in the S2-S5 dermatomes bilaterally, specifically involving the posterior thighs, perianal region, and plantar aspects of the feet. Rectal examination revealed significantly diminished voluntary anal sphincter tone, and the bulbocavernosus reflex was absent. Plantar reflexes were bilaterally downgoing. No specific saddle anesthesia could be precisely mapped due to the child's distress, but the overall pattern suggested a significant sacral plexopathy or cauda equina injury. Peripheral pulses were 2+ bilaterally in all four extremities, and capillary refill was brisk, indicating no major vascular compromise. Pelvic stability assessment via a gentle compression-distraction maneuver was deferred due to the suspected sacral fracture and potential for exacerbation of neurological injury.
Imaging & Diagnostics
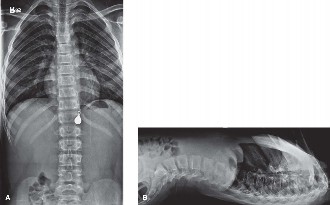
Initial radiographic series included anteroposterior (AP) pelvic, inlet, and outlet views. The AP pelvis demonstrated widening of the right sacroiliac joint space and an ill-defined fracture line extending through the right sacral ala. The inlet view further clarified the posterior displacement of the right hemipelvis and comminution within the sacral ala. The outlet view suggested vertical translation. Given the high-energy mechanism and clinical findings, a computed tomography (CT) scan of the pelvis was immediately performed.
The CT scan provided detailed three-dimensional information, revealing a complex, comminuted right sacral fracture involving Denis Zone II and extending into Zone III (medial to the right sacral foramen), with significant displacement. Specifically, the fracture line coursed obliquely through the right S1 and S2 sacral foramen, with bone fragments potentially impinging on the exiting S1 and S2 nerve roots. There was evident disruption of the anterior sacroiliac ligament complex and the posterior sacral elements, consistent with an unstable injury pattern. The sacral canal appeared narrowed by displaced bone fragments at the S1-S2 level on the right. No intraluminal extravasation of contrast was noted on CT angiogram performed concurrently, ruling out major arterial injury.
Figure 1: Pre-operative CT scan, axial view, demonstrating the comminuted right sacral fracture involving Denis Zones II and III, with significant displacement of bone fragments into the sacral canal.
Given the strong clinical suspicion of neurological compromise and the CT findings suggesting neural canal impingement, a magnetic resonance imaging (MRI) scan of the lumbosacral spine and pelvis was obtained. The MRI confirmed significant edema and hemorrhage surrounding the S1, S2, and S3 nerve roots on the right, with direct compression by displaced sacral fracture fragments. T2-weighted images showed high signal intensity within the nerve roots themselves, indicative of nerve contusion and possible Wallerian degeneration. No obvious nerve root avulsion was identified, but significant perineural fibrosis and inflammation were evident. The MRI also helped rule out concomitant lumbar spine injuries or disc herniations that could contribute to the neurological deficit. Templating for potential sacral fixation was initiated based on the CT and MRI, assessing screw trajectory and length to avoid further neurovascular compromise. The goal was to plan for adequate decompression and stable fixation.
Differential Diagnosis
The differential diagnosis for sacral region pain and neurological deficit in a pediatric trauma patient is broad but can be narrowed significantly by the acute presentation and high-energy mechanism.
| Feature | Sacral Fracture with Neurological Compromise (Index Case) | Lumbosacral Dissociation | Isolated Sacroiliac Joint Dislocation (without fracture) |
|---|---|---|---|
| Mechanism | High-energy, axial loading, direct trauma to sacrum. | High-energy, often pure shear or distractive forces to lumbosacral junction. | Moderate-to-high energy, rotational or compressive forces to pelvis. |
| Pain Location | Sacral, gluteal, perineal, radiating to lower extremities. | Lumbosacral junction, radiating to sacrum/buttocks/lower extremities. | Sacroiliac joint, buttock, radiating to posterior thigh. |
| Neurological Deficit | Specific sacral root involvement (S1-S5) leading to bowel/bladder dysfunction, perineal numbness, plantarflexion/toe flexion weakness. | Often cauda equina syndrome with L5/S1 root involvement, variable bowel/bladder dysfunction. | Less common; if present, typically due to significant pelvic ring instability with nerve traction. |
| Physical Exam | Sacral tenderness, gluteal ecchymosis, diminished anal tone, positive bulbocavernosus reflex. | Tenderness at L5-S1, palpable step-off, profound neurological deficit. | SI joint tenderness, pain on provocative SI maneuvers (e.g., Faber test), leg length discrepancy. |
| Radiographic Findings | Fracture lines through sacral ala/foramina, displacement of bone fragments into canal (Denis Zone II/III). | Widening of L5-S1 disc space, facet disruption, transverse process fractures, superior displacement of L5 relative to S1. | Widening/subluxation of SI joint on stress views, no obvious fracture. |
| CT Findings | Detailed fracture morphology, neural canal compromise, fragment displacement. | Clear visualization of L5-S1 dissociation, facet joint disruption, associated avulsion fractures. | SI joint incongruity, capsular disruption, absence of fracture. |
| MRI Findings | Nerve root contusion/compression, edema, hemorrhage within sacral canal. | Ligamentous disruption (iliolumbar, posterior longitudinal), nerve root stretching/impingement. | Ligamentous disruption (sacroiliac ligaments), joint capsule edema/hemorrhage. |
| Management | Surgical decompression and stabilization for unstable fractures with neurological deficit. | Urgent surgical stabilization and decompression. | Often non-operative if stable; surgical stabilization for irreducible/unstable dislocations. |
Surgical Decision Making & Classification
The decision for operative intervention in this pediatric sacral trauma case was primarily driven by the unstable fracture pattern, significant displacement, and clear evidence of neurological compromise (sacral plexopathy affecting S1-S5, including bowel/bladder dysfunction and perineal numbness). While non-operative management might be considered for stable, non-displaced sacral fractures, especially in children due to their high healing potential, the presence of a neurological deficit mandates surgical decompression and stabilization.
The fracture was classified using the
Denis Classification
system as a
Zone II/III fracture
.
*
Denis Zone II
(transforaminal): This involves the sacral foramina, often leading to exiting nerve root impingement. Our patient had clear involvement of the S1 and S2 foramina.
*
Denis Zone III
(medial to the foramen/central canal): This indicates injury to the sacral canal itself, affecting the cauda equina or sacral nerve roots directly. The CT and MRI confirmed displaced fragments within the sacral canal, compressing multiple nerve roots.
Furthermore, the overall pelvic ring injury pattern could be considered an unstable posterior ring injury according to the Young-Burgess classification, likely a vertical shear component given the sacral fracture and potential SI disruption, though the primary focus remained on the sacrum itself. In the pediatric population, fracture characteristics often exhibit greater plasticity; however, the principles of reduction and stabilization for neurological preservation remain paramount. Given the patient's age, future growth potential, and the risk of persistent neurological deficits, prompt surgical intervention was deemed essential. The surgical goals were direct decompression of the sacral nerve roots, anatomical reduction of the sacral fracture, and stable fixation to promote healing and neurological recovery. The timing of surgery was urgent, within 12 hours of presentation, to maximize the potential for neurological recovery.
Surgical Technique / Intervention
The patient was positioned prone on a radiolucent operating table, ensuring careful padding of all pressure points, especially in a pediatric patient. Anesthesia was induced, and a Foley catheter was inserted to monitor urine output and also serve as an intraoperative indicator of urethral integrity. Fluoroscopy was used for initial localization and throughout the procedure.
A midline posterior approach was utilized, extending from the L5 spinous process down to the distal sacrum, curving slightly to the right to expose the sacral region. Subperiosteal dissection was carefully performed to expose the posterior sacrum, including the fractured sacral ala and the posterior elements of S1 and S2. Meticulous hemostasis was maintained to optimize visualization.
Upon exposure, the comminuted sacral fracture was clearly visualized. Multiple displaced bone fragments were impinging upon the right S1 and S2 nerve roots, which were visibly swollen and under tension. A critical step was the direct decompression of these nerve roots. This involved careful removal of impinging bone fragments using Kerrison rongeurs and osteotomes, followed by gentle manipulation to unroof the sacral canal and foramina. Special attention was paid to identifying and preserving the delicate nerve rootlets. The dura was inspected for any tears; none were identified. After adequate decompression, the nerve roots were observed to relax, and their mobility improved.
Next, fracture reduction was performed. This involved a combination of indirect and direct maneuvers. Indirect reduction was attempted via traction on the ipsilateral lower extremity and manipulation of the right iliac wing. Direct reduction of the sacral fracture fragments was then performed using reduction clamps and custom-bent instruments. The goal was to restore the anatomical alignment of the sacrum, particularly the continuity of the sacral foramen and the sacral canal. Intraoperative fluoroscopy confirmed satisfactory reduction in AP, inlet, and outlet views.
Fixation construct
: Given the unstable nature of the injury and the need for robust stability in a growing child, a combination of fixation techniques was employed:
1.
Iliosacral Screws
: Two percutaneously placed iliosacral screws were planned to stabilize the SI joint and the sacral ala. A guide wire was advanced under biplanar fluoroscopic guidance from the iliac crest, across the sacroiliac joint, and into the S1 and S2 vertebral bodies. The trajectory was carefully planned to avoid the sacral canal and sciatic notch. Cannulated screws (6.5mm) were then advanced over the guide wires. The pedicle of L5 was also considered for an additional screw for lumbopelvic fixation but was deemed unnecessary given the reduction quality and sacral comminution.
2.
Sacral Reconstruction Plate/Tension Band Plating
: To augment fixation and provide direct compression across the comminuted sacral fracture, a custom-bent posterior sacral reconstruction plate (3.5mm) was contoured and placed over the posterior sacral elements. This plate served as a tension band, providing additional stability. Screws were carefully inserted into the sacral ala and the stable portions of the sacral body, again with strict fluoroscopic control to ensure no intrusion into the neural canal.

Figure 2: Post-operative AP fluoroscopic image demonstrating anatomically reduced sacral fracture with stable fixation using two iliosacral screws and a posterior sacral tension band plate.
Thorough irrigation was performed, and meticulous closure in layers completed the procedure. A drain was placed and removed on post-operative day 2. The estimated blood loss was 250 mL, and the patient tolerated the procedure well.
Post-Operative Protocol & Rehabilitation
Immediately post-operatively, the patient was admitted to the pediatric intensive care unit for close neurological monitoring and pain management.
Phase 1: Early Post-operative (Weeks 0-6)
*
Pain Management
: Multimodal analgesia including intravenous patient-controlled analgesia (PCA) transitioning to oral medications.
*
Neurological Monitoring
: Hourly neurological checks (motor, sensory, anal tone, bulbocavernosus reflex) for the first 24-48 hours, then four-hourly, looking for signs of deterioration or improvement.
*
Bowel and Bladder Management
: Foley catheter remained in situ for 5 days. Bowel regimen initiated with stool softeners to prevent straining. Neurological bladder training would commence if voiding difficulties persisted after catheter removal.
*
Mobility
: Strict non-weight bearing (NWB) on the affected side and protected partial weight-bearing (PWB) on the contralateral side with a walker/crutches. Log rolling for turning.
*
Physical Therapy
: Early initiation of gentle passive range of motion (PROM) for hips and knees. Ankle pump exercises. Respiratory physiotherapy.
*
Wound Care
: Daily dressing changes, monitoring for infection.
Phase 2: Intermediate Healing (Weeks 6-12)
*
Imaging
: Follow-up radiographs at 6 weeks to assess fracture healing and hardware integrity. CT scan may be considered if union is questionable or symptoms persist.
*
Weight-Bearing
: Gradual progression to protected weight-bearing (e.g., 25% to 50%) with crutches, as tolerated and guided by clinical healing and imaging.
*
Physical Therapy
: Focus on strengthening exercises for hip abductors, extensors, and core musculature. Progressive ambulation training. Neurological rehabilitation for sacral plexus, including biofeedback for perineal muscles if needed.
*
Neurological Recovery
: Continued monitoring of sensory and motor deficits. Referral to a pediatric neurorehabilitation specialist if neurological recovery is plateauing or incomplete.
Phase 3: Advanced Rehabilitation & Return to Activity (Months 3-6+)
*
Weight-Bearing
: Full weight-bearing as tolerated once radiographic union is evident and pain subsides.
*
Physical Therapy
: Advanced strengthening, balance, and proprioceptive training. Gradual return to age-appropriate activities.
*
Hardware Removal
: Consideration for hardware removal typically 12-18 months post-operatively in pediatric patients, especially if hardware causes impingement or if the child has significant growth remaining. This decision is made on a case-by-case basis.
*
Long-Term Follow-up
: Regular clinical and radiographic follow-up to monitor for malunion, nonunion, or late neurological complications. Assessment of bowel/bladder function and sexual function in the long term.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- High Index of Suspicion in Pediatric Trauma : Sacral fractures are less common in children than adults, but when they occur, they are often associated with high-energy trauma and significant neurological injury due to the elastic nature of pediatric bone and surrounding ligaments.
- Challenges in Pediatric Neurological Exam : Obtaining a precise neurological assessment in a child, especially with pain, can be difficult. Look for subtle signs: changes in crying patterns, decreased spontaneous movement, guarding, decreased anal tone, and absence of age-appropriate reflexes (e.g., bulbocavernosus reflex). Documenting bowel and bladder function rigorously is paramount.
-
Multimodal Imaging is Key
:
- Plain Radiographs : Initial screening, but often underestimate the extent of sacral fractures. AP, inlet, and outlet views are essential.
- CT Scan : The gold standard for bony detail, fracture morphology, neural canal compromise, and displacement. Essential for surgical planning.
- MRI Scan : Crucial for evaluating soft tissue injury, nerve root integrity (contusion, avulsion, compression), and dural tears. Essential for confirming neurological involvement and guiding decompression.
- Denis Classification for Sacral Fractures : Understand Zones I (alar), II (foraminal), and III (central canal). Zone II and III injuries carry a higher risk of neurological deficit.
- Urgent Decompression for Neurological Deficit : Unstable sacral fractures with evolving or present neurological deficits (especially bowel/bladder dysfunction) warrant urgent surgical decompression and stabilization, ideally within 24 hours, to maximize the potential for neurological recovery.
-
Precise Surgical Technique
:
- Prone Positioning : Standard for posterior sacral approaches.
- Meticulous Dissection : Subperiosteal dissection to expose sacral elements, identifying nerve root exits.
- Direct Decompression : Carefully remove impinging bone fragments. Visual confirmation of nerve root relaxation is ideal.
- Fluoroscopic Guidance : Absolute necessity for safe screw placement (iliosacral, trans-sacral) to avoid iatrogenic nerve or vessel injury. Biplanar views are critical.
- Robust Fixation : Pediatric bone can be more forgiving, but unstable sacral fractures require strong fixation (e.g., iliosacral screws, posterior tension band plating) to prevent redisplacement and promote healing.
- Interdisciplinary Care : Involve pediatric neurosurgery, urology, and rehabilitation medicine early for comprehensive management and long-term follow-up.
Pitfalls:
- Underestimation of Injury Severity : Relying solely on plain radiographs can lead to missed or underestimated sacral fractures, especially with non-displaced fractures or those obscured by bowel gas.
- Inadequate Neurological Assessment : Failure to perform a comprehensive neurological exam, particularly rectal tone and perineal sensation, can miss critical deficits. Do not assume neurological deficits are transient.
- Delayed Intervention : Procrastination in surgical decompression for neurological compromise can lead to irreversible nerve damage and poorer functional outcomes.
- Iatrogenic Nerve Injury : Inaccurate placement of iliosacral screws or aggressive decompression can damage exiting nerve roots, the sciatic nerve, or superior gluteal vessels. Thorough pre-operative templating and strict intraoperative fluoroscopic control are vital.
- Hardware-Related Complications : Screw pull-out, breakage, or prominence, especially in a growing child. Consideration for hardware removal after union.
- Failure to Recognize Associated Injuries : Sacral fractures are often part of a larger pelvic ring injury; missing an anterior ring component can lead to persistent instability. Lumbar spine injuries also need to be ruled out.
- Long-Term Bowel/Bladder Dysfunction : Even with successful surgical intervention, some degree of residual neurological dysfunction is possible, requiring long-term management and support.
- Lack of Pediatric Specificity : Treating pediatric sacral fractures exactly like adult fractures without considering growth plates, bone plasticity, and unique rehabilitation challenges can lead to suboptimal outcomes.
