Mastering Periprosthetic and Distal Humeral Fractures: Advanced Surgical Techniques and Biomechanics
Key Takeaway
Periprosthetic and distal humeral fractures present complex reconstructive challenges due to compromised bone stock and articular comminution. Successful management demands a rigorous understanding of fracture biomechanics, precise implant selection, and meticulous surgical execution. This comprehensive guide details evidence-based protocols for open reduction and internal fixation (ORIF), optimal surgical approaches including olecranon osteotomy, and advanced plating techniques to achieve stable fixation and facilitate early postoperative mobilization.
PERIPROSTHETIC HUMERAL SHAFT FRACTURES
Periprosthetic humeral shaft fractures following shoulder or elbow arthroplasty represent a rare but highly demanding clinical scenario. The primary contributing factor to these fractures is compromised bone stock secondary to age-related osteoporosis, osteomalacia, or rheumatoid arthritis. Consequently, a diverse array of fracture patterns can emerge from low-energy mechanisms, such as direct blows, minor twisting injuries, "same-level" falls, or intraoperative technical errors during the primary or revision arthroplasty.
Fractures surrounding humeral arthroplasties may manifest at the tuberosity level, the metaphysis, or the upper diaphysis—either encompassing the stem or extending distal to the stem tip. Similarly, fractures associated with the humeral component of total elbow arthroplasties (TEA) can occur at any level, ranging from the medial or lateral column to regions proximal to the stem tip.
Treatment Algorithm and Decision Making
The management of periprosthetic humeral fractures is dictated by two critical variables: fracture stability and implant stability (loosening).
- Stable Fractures with Well-Fixed Components: Can be managed conservatively with functional bracing and strict immobilization.
- Stable Fractures with Component Loosening: Necessitate revision arthroplasty. This can be performed immediately or delayed until after fracture healing if the patient remains symptomatic.
- Unstable Fractures (with or without loosening): Require operative intervention. If the component is loose, revision arthroplasty combined with fracture fixation is mandatory, adhering to the general principles of revision surgery.
Clinical Pearl: Bone quality ultimately dictates the necessity for supplemental fixation. The surgeon must be prepared to utilize structural allograft struts, methyl methacrylate (PMMA) cement, or autogenous bone grafting to achieve a biomechanically sound construct in osteopenic bone.
Surgical Guidelines for Well-Fixed Components
When addressing unstable periprosthetic humeral shaft fractures where the existing prosthesis remains well-fixed, the goal is primary fracture union rather than prophylactic revision to a long-stem implant. Revision arthroplasty carries higher complication rates and inferior functional outcomes compared to primary arthroplasty.
The following evidence-based guidelines, adapted from Cameron and Iannotti, should direct surgical fixation:
- Tuberosity Fractures: Displaced tuberosity fractures must be anatomically reduced and repaired using heavy non-absorbable suture or cerclage wire. Any associated rotator cuff pathology must be addressed concurrently to restore dynamic stability.
- Diaphyseal Fractures: Unstable diaphyseal fractures around or below the prosthesis mandate Open Reduction and Internal Fixation (ORIF). Standard cerclage wiring or limited screw fixation is biomechanically insufficient.
- Construct Rigidity: A heavy, broad-contact plate utilizing proximal cerclage cables and distal locking screws is the gold standard.
- Biomechanical Requirement: The construct requires a minimum of four proximal cables and four distal screws, engaging at least eight cortices.
- Cable Selection: We strongly recommend the use of 2.0-mm cables over standard 1.6-mm cables to prevent fatigue failure and cable pull-through in osteoporotic bone.
Management of Severe Osteopenia
In the presence of profound osteopenia, standard plating techniques may fail due to screw pull-out. Fixation can be augmented with PMMA cement; however, extreme caution must be exercised to prevent cement extrusion into the fracture site, which would inhibit osteogenesis and lead to nonunion.
Surgical Warning: If severe osteopenia is encountered, the fixation construct should be reinforced with a full-thickness cortical allograft strut. This strut must be applied orthogonally (90 degrees) to the primary plate-cable-screw construct using additional cables, effectively creating a bicolumnar biomechanical shield. Autograft bone should be packed meticulously around the fracture site to stimulate union.
Intraoperative Fractures
Intraoperative fractures during primary shoulder or elbow arthroplasty are devastating complications that can largely be avoided through meticulous preoperative templating, careful reaming, and profound respect for osteopenic bone. If an intraoperative fracture occurs, it must be addressed immediately during the index procedure, either via rigid internal fixation or by bypassing the fracture with a longer-stemmed revision implant that extends at least two cortical diameters past the most distal fracture line.
DISTAL HUMERAL FRACTURES
Fractures of the distal humerus remain one of the most formidable challenges in orthopedic traumatology. Despite significant advancements in implant technology and surgical techniques, these injuries are fraught with complications. They frequently involve severe articular comminution and predominantly occur in elderly patients with osteoporotic bone.
The ultimate functional outcome is often compromised by stiffness, pain, and residual weakness. While a perfectly "normal" elbow is a rare outcome, modern bicolumnar plating techniques and accelerated rehabilitation protocols have yielded good to excellent results in approximately 87% of patients. Unlike proximal humerus or humeral shaft fractures, the vast majority of distal humeral fractures in adults demand operative intervention.
Exception to Operative Management: Nonoperative treatment utilizing the "bag of bones" technique (brief immobilization followed by gravity-assisted range of motion) is reserved strictly for elderly, low-demand patients with severe medical comorbidities that preclude surgical intervention.
Anatomy, Biomechanics, and Classification
The complexity of distal humeral fractures is best understood through the "two-column" and "tie-arch" concepts of elbow stability. The distal humerus is formed by a medial and lateral column that diverge from the diaphysis, supporting the articular segment (trochlea and capitellum) like an arch. Disruption of this arch leads to profound multidirectional instability.
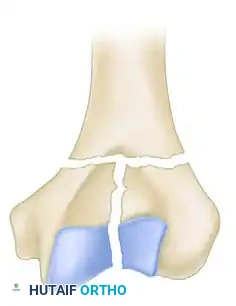
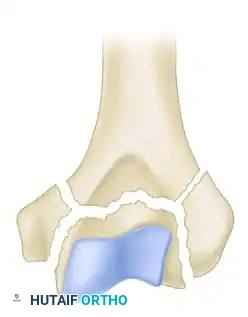
While the AO/OTA classification system is exhaustive (defining 61 types across A, B, and C categories), the Jupiter and Mehne classification, as well as the Mehne and Matta bicolumnar descriptions, offer superior utility for preoperative templating. Mehne and Matta categorize complex bicolumnar fractures based on their geometric configuration:
Mehne and Matta High T-Fracture configuration.
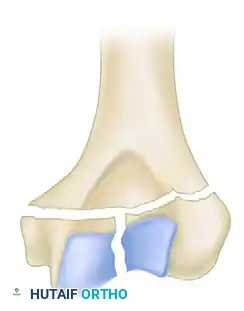
Mehne and Matta Low T-Fracture configuration.
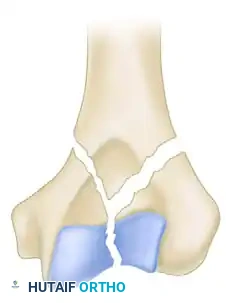
Mehne and Matta Y-Fracture configuration.
Mehne and Matta Medial Lambda configuration.
Mehne and Matta Lateral Lambda configuration.
Mehne and Matta H-Fracture configuration.
Surgical Approaches to the Distal Humerus
The primary goal of surgery is the anatomical restoration of the articular surface combined with stable internal fixation of both columns to the diaphysis, permitting immediate postoperative motion. The choice of surgical approach is critical and depends on the fracture pattern and the need for articular visualization.
1. Olecranon Osteotomy (Trans-olecranon Approach)
Historically, the posterior approach utilizing an intra-articular chevron olecranon osteotomy has provided the most unparalleled, panoramic exposure of the distal humeral articular surface. It is the gold standard for complex AO Type C fractures. However, it carries inherent risks, including osteotomy nonunion, hardware prominence, and triceps weakness.
2. Triceps-Sparing and Triceps-Reflecting Approaches
Concerns regarding osteotomy complications have driven the evolution of triceps-reflecting approaches (e.g., Bryan-Morrey, or the Triceps-Reflecting Anconeus Pedicle [TRAP] approach) and triceps-splitting approaches (e.g., Campbell approach).

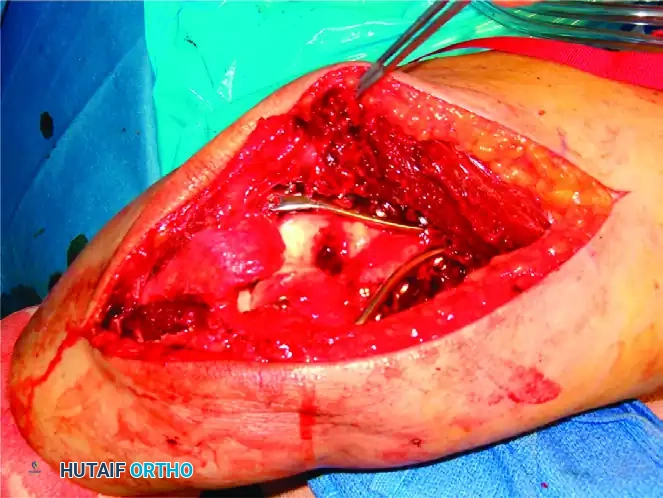
Intraoperative view of plate application through a triceps-reflecting approach, preserving the extensor mechanism.
Radiographic confirmation of bicolumnar fixation achieved via a triceps-reflecting exposure.
These approaches are particularly advantageous when total elbow arthroplasty (TEA) is considered as a backup option, or in patients with severe osteopenia where osteotomy healing is questionable.
Ulnar Nerve Management
Regardless of the posterior approach selected, the ulnar nerve must be meticulously identified, neurolysed, and protected. Routine anterior transposition remains controversial. Recent literature suggests that routine transposition may increase the incidence of iatrogenic ulnar neuritis by up to four times compared to in situ decompression, provided the nerve is not under tension from the hardware construct.
Principles of Internal Fixation
Stable fixation of the distal humerus requires rigid bicolumnar plating. Historically, orthogonal plating (90-90 configuration, with one plate medial and one posterolateral) was the standard. However, contemporary biomechanical studies and clinical outcomes heavily support parallel (180-degree) plating, which provides superior resistance to varus/valgus stress and torsional forces, particularly in comminuted fractures.
The Sanchez-Sotelo Principles of Fixation
To achieve maximum biomechanical stability, the following principles must be strictly adhered to:
* Plate Utilization: Every screw inserted into the distal fragment should pass through a plate.
* Interdigitation: Each screw should engage a bone fragment on the opposite side that is also secured to a plate.
* Distal Density: Maximize the number of screws placed into the distal articular fragments.
* Maximum Length: Each screw should be as long as possible to maximize thread purchase in osteoporotic bone.
* Articular Capture: Each screw should engage as many articular fragments as possible.
* Supracondylar Compression: Plates must be applied to achieve dynamic compression at the supracondylar level for both columns.
* Implant Rigidity: The plates utilized must possess sufficient stiffness to resist bending or fatigue failure before supracondylar union occurs. Precontoured anatomical locking plates are vastly superior to one-third tubular or standard 3.5-mm reconstruction plates.
Step-by-Step Reconstruction Strategies
Reconstruction of the distal humerus is a complex puzzle that must be approached systematically. Two primary strategies exist:
Strategy 1: Articular-First Reconstruction
1. Anatomically reduce and provisionally fix the articular fragments (trochlea and capitellum) using K-wires.
2. Convert provisional fixation to definitive fixation using headless compression screws, countersunk mini-fragment screws, or bioabsorbable screws.
3. Reduce the reconstructed articular block to the humeral shaft and secure it with bicolumnar plates.
Strategy 2: Column-First Reconstruction (Preferred for severe articular comminution)
1. Reduce and rigidly fix the least comminuted condyle (usually the lateral column) to the humeral shaft.
2. Reconstruct the articular surface, building off the stabilized condyle.
3. Reduce and fix the contralateral condyle to the shaft and the reconstructed articular block.
Surgical Pitfall: When utilizing lag screws across the trochlea in the presence of bone loss, extreme care must be taken to avoid over-compression. Narrowing the trochlea will alter the radiocapitellar and ulnohumeral kinematics, leading to rapid joint destruction and severe stiffness.
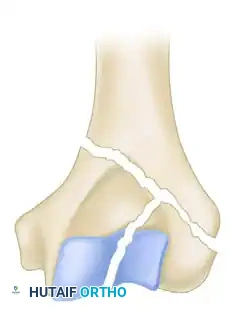
For isolated column fractures (AO/OTA Type B), a direct approach with simple lag screw fixation and buttress plating is often sufficient.

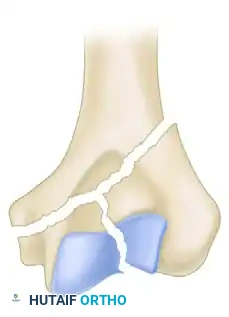
Illustration of an isolated lateral condylar fracture.

Fixation of the lateral condyle utilizing a lag screw and a contoured mini-fragment buttress plate.
Postoperative Rehabilitation and Outcomes
The entire premise of rigid bicolumnar fixation is to permit immediate postoperative mobilization. If the biomechanical goals of surgery are met, rehabilitation must commence within 3 days of surgery.
- Immobilization Risk: Immobilization exceeding 3 weeks universally results in profound, often irreversible, arthrofibrosis and disabling elbow stiffness.
- Protocol: Supervised physical therapy is mandated three times weekly, supplemented by a rigorous daily home exercise program focusing on active and active-assisted range of motion.
- Adjuncts: If early motion milestones are not achieved by week 4, dynamic flexion and extension splinting should be prescribed immediately.
While union rates for distal humeral fractures have improved dramatically with modern locking plate technology, stiffness remains the most frequent complication, occasionally necessitating secondary procedures such as arthroscopic or open capsular release and hardware removal. Despite these challenges, meticulous adherence to bicolumnar fixation principles reliably yields functional arcs of motion (average 108 degrees) and restores over 70% of native limb strength.
📚 Medical References
- humeral fractures: mechanisms of fracture and treatment options, J Shoulder Elbow Surg 7:406, 1998.
- Chin PY, Sperling JW, Cofi eld RH, et al: Complications of total shoulder arthroplasty: are they fewer or different? J Shoulder Elbow Surg 15:19, 2006.
- Coste JS, Reig S, Trojani C, et al: The management of infection in arthroplasty of the shoulder, J Bone Joint Surg 86B:65, 2004.
- Crosby LA: Complications. In Crosby LA, ed: Total shoulder arthroplasty , Rosemont, Ill, 2000, American Academy of Orthopaedic Surgeons. Dines JS, Fealy S, Strauss EJ, et al: Outcomes analysis of revision total shoulder replacement, J Bone Joint Surg 88:1494, 2006.
- Fink B, Sallen V, Guderian H, et al: Resection interposition arthroplasty of the shoulder affected by infl ammatory arthritis, J Shoulder Elbow Surg 10:365, 2001.
- Franklin JL, Barrett WP, Jackins SE, et al: Glenoid loosening in total shoulder arthroplasty: association with rotator cuff defi ciency, J Arthroplasty 3:39, 1988.
- Hasan SS, Leith JM, Campbell B, et al: Characteristics of unsatisfactory shoulder arthroplasties, J Shoulder Elbow Surg 11:431, 2002.
- Hawkins RJ, Greis PE, Bonutti PM: Treatment of symptomatic glenoid loosening following unconstrained shoulder arthroplasty, Orthopedics 22:230, 1999.
- Hennigan SP, Iannotti JP: Instability after prosthetic arthroplasty of the shoulder, Orthop Clin North Am 32:649, 2001.
- Hersch JC, Dines JM: Arthroscopy for failed shoulder arthroplasty, Arthroscopy 16:606, 2000.
- Kjaersgaard-Andersen P, Frich LH, Søjbjerg JO, et al: Heterotopic bone formation following total shoulder arthroplasty, J Arthroplasty 4:99, 1989.
- Klimkiewica JJ, Iannotti JP, Rubash HE, et al: Aseptic loosening of the humeral component in total shoulder arthroplasty, J Shoulder Elbow Surg 7:422, 1998.
- Klingman M, Roffman M: Humeral fracture following shoulder arthroplasty, Orthopedics 22:511, 1999.
- Kørsgaard-Andersen P, Frich LH, Søjberg JO, et al: Heterotopic bone formation following total shoulder arthroplasty, J Arthroplasty 4:99, 1989.
- Krakauer JD, Cofi eld RH: Periprosthetic fractures in total shoulder arthroplasty, Op Tech Orthop 4:243, 1994.
- Kumar S, Sperling JW, Haidukewych GH, Cofi eld RH: Periprosthetic humeral fractures after shoulder arthroplasty, J Bone Joint Surg 86A:680, 2004.
- Lynch NM, Cofi eld RH, Silbert PL, et al: Neurologic complications after total shoulder arthroplasty, J Shoulder Elbow Surg 5:53, 1996.
- Milbrink J, Wigren A: Resection arthroplasty of the shoulder, Scand J Rheumatol 19:432, 1990.
- Moeckel BH, Altchek DW, Warren RF, et al: Instability of the shoulder after arthroplasty, J Bone Joint Surg 75A:492, 1993.
- Murthi AM, Vosburgh CL, Neviaser TJ: The incidence of pathologic changes of the long head of the biceps tendon, J Shoulder Elbow Surg 9:382, 2000.
- Neer CS II, Kirby RM: Revision of humeral head and total shoulder arthroplasties, Clin Orthop Relat Res 170:189, 1982.
- [Neer CS, Rockwood CA: Fractures and dislocations of the shoulder. In Rockwood CA, Green DP, eds: Fractures , Philadelphia, 1984, Lippincott.
Norris TR, Lipson SR: Management of the unstable prosthetic shoulder arthroplasty, Instr Course Lect 47:141, 1998.](https://pubmed.ncbi.nlm.nih.gov/?term=Neer%20CS%2C%20Rockwood%20CA%3A%20Fractures%20and%20dislocations%20of%20the%20shoulder.%20In%20Rockwood%20CA%2C%20Green%20DP%2C%20eds%3A%20Fractures%20%2C%20Philadelphia%2C%201984%2C%20Lippincott.%0A%0ANorris%20TR%2C%20Lipson%20SR%3A%20Management%20of%20the%20unstable%20prosthetic%20shoulder%20arthroplasty%2C%20Instr%20Course%20Lect%2047%3A141%2C%201998.)
- Peterson SA, Hawkins RJ: Revision of failed total shoulder arthroplasty, Orthop Clin North Am 29:519, 1998.
- Sanchez-Sotelo J, Sperling JW, Rowland CM, et al: Instability after shoulder arthroplasty: results of surgical treatment, J Bone Joint Surg 85A:622, 2003.
- Sperling JW, Cofi eld RH: Revision total shoulder arthroplasty for the treatment of glenoid arthrosis, J Bone Joint Surg 80A:860, 1998.
- Sperling JW, Cofi eld RH, Rowland CM: Heterotopic ossifi cation after total shoulder arthroplasty, J Arthroplasty 15:179, 2000.
- Sperling JW, Kozak TK, Hanssen AD, et al: Infection after total shoulder arthroplasty, Clin Orthop Relat Res 382:206, 2001.
- Wallace AL, Walsh WR, Sonnabend DH: Dissociation of the glenoid component in cementless total shoulder arthroplasty, J Shoulder Elbow Surg 8:81, 1999.
- Wiater JM, Levine WN: Revision shoulder arthroplasty. In Crosby LA, ed: Total shoulder arthroplasty, Rosemont, Ill, 2000, American Academy of Orthopaedic Surgeons. Williams GR Jr, Wong KL, Pepe MD, et al: The effect of articular malposition after total shoulder arthroplasty on glenohumeral translations, range of motion, and subacromial impingement, J Shoulder Elbow Surg 10:399, 2001.
- Wirth MA, Rockwood CA: Complications of total shoulder replacement arthroplasty, J Bone Joint Surg 78A:603, 1996.
- Worland RL, Kim DY, Arredondo J: Periprosthetic humeral fractures: management and classifi cation, J Shoulder Elbow Surg 8:590, 1999.
- Wright TW, Cofi eld RH: Humeral fractures after shoulder arthroplasty, J Bone Joint Surg 77A:1340, 1995.
- [Elbow
History Coonrad RW: History of total elbow arthoplasty. In American Academy of Orthopaedic Surgeons (Inglis AE, ed): Symposium on total joint replacement of the upper extremity. St Louis, 1982, Mosby. Mills R, Rush J: Skin arthroplasty of the elbow, Aust NZ J Surg 41:179, 1971.](https://pubmed.ncbi.nlm.nih.gov/?term=Elbow%0A%0AHistory%20Coonrad%20RW%3A%20History%20of%20total%20elbow%20arthoplasty.%20In%20American%20Academy%20of%20Orthopaedic%20Surgeons%20%28Inglis%20AE%2C%20ed%29%3A%20Symposium%20on%20total%20joint%20replacement%20of%20the%20upper%20extremity.%20St%20Louis%2C%201982%2C%20Mosby.%20Mills%20R%2C%20Rush%20J%3A%20Skin%20arthroplasty%20of%20the%20elbow%2C%20Aust%20NZ%20J%20Surg%2041%3A179%2C%201971.)
You Might Also Like


