Achilles Tendon Repair: The Percutaneous Perspective You Need

Key Takeaway
Here are the crucial details you must know about Achilles Tendon Repair: The Percutaneous Perspective You Need. Achilles tendon rupture is a common injury to the body's thickest tendon, often caused by forceful movements. Untreated ruptures form nonfunctional fibrous gaps, severely impairing mobility. From a tendon repair perspective percutaneous approaches aim to restore tendon integrity, addressing the clinically diagnosed tear typically presenting with an audible snap and a palpable gap, preventing chronic disability.
Introduction and Epidemiology
Rupture of the Achilles tendon remains one of the most common major tendon ruptures treated by orthopedic surgeons, with an estimated incidence of 18 per 100,000 individuals in the general population. The demographic distribution typically exhibits a bimodal peak, primarily affecting active individuals between the ages of 30 and 50 years—often colloquially referred to as "weekend warriors"—and a secondary, smaller peak in the elderly population associated with degenerative tendinopathy. Despite the frequency of this injury, more than 20% of acute ruptures are misdiagnosed at initial presentation in the emergency department or primary care setting. This diagnostic failure frequently leads to chronic or neglected ruptures, complicating subsequent surgical management and significantly compromising patient outcomes.
The pathogenesis of Achilles tendon rupture is multifactorial, combining mechanical overload with underlying tendinopathic degeneration. The most common mechanism of injury involves an eccentric load applied to a dorsiflexed ankle with the knee extended, such as pushing off with the weight-bearing forefoot during a sudden acceleration phase in sports. Alternatively, sudden unexpected dorsiflexion of the ankle or violent dorsiflexion of a plantarflexed foot can exceed the ultimate tensile strength of the tendon, resulting in catastrophic failure. Systemic factors and pharmacological agents significantly alter the structural integrity of the collagen matrix. Corticosteroid injections, systemic fluoroquinolone administration, inflammatory arthropathies, and inherent poor vascularity of the tendon have all been strongly associated with an increased risk of rupture.

The natural history of an untreated or delayed Achilles tendon rupture is characterized by the retraction of the proximal musculotendinous unit and the formation of a discrete gap. Over time, this gap between the ruptured tendon ends fills with a disorganized, mechanically inferior fibrous scar tissue. This nonfunctional scar elongates the resting length of the gastrocsoleus complex, profoundly altering the length-tension relationship of the muscle fibers. Consequently, patients experience significant deficits in plantarflexion power, finding routine activities such as walking, ascending stairs, and standing on tiptoes on the affected limb nearly impossible.
Surgical Anatomy and Biomechanics
Musculotendinous Architecture
The Achilles tendon is the thickest and strongest tendon in the human body, capable of withstanding loads up to ten times body weight during running and jumping activities. It is formed by the confluence of the gastrocnemius and soleus muscles. The two heads of the gastrocnemius arise from the posterior aspects of the medial and lateral femoral condyles, crossing both the knee and ankle joints. As the fleshy part of the muscle descends to approximately the midcalf, the fibers insert into a broad, flat aponeurosis. This aponeurosis narrows and thickens as it descends, receiving the tendon of the soleus on its deep anterior surface to form the true Achilles tendon.
Measuring approximately 15 cm in length, the tendon extends distally to insert into the posterior surface of the calcaneal tuberosity. A critical anatomical feature is the internal rotation of the tendon fibers as they descend. The fibers originating from the medial gastrocnemius rotate laterally to insert on the posterior and lateral aspect of the calcaneus, while the fibers from the soleus rotate medially to insert on the deeper, medial aspect. This complex spiraling architecture is thought to impart a mechanical advantage, allowing the tendon to store and release elastic strain energy efficiently during the stretch-shortening cycle of human locomotion.
Vascular Supply and Tissue Viability
The vascular supply to the Achilles tendon is precarious and highly relevant to its pathogenesis and surgical management. The tendon receives its blood supply from three main sources: the musculotendinous junction proximally, the osseotendinous junction distally, and the surrounding paratenon along its length. Angiographic studies have consistently demonstrated a relative hypovascular zone, or "watershed area," located approximately 2 to 6 cm proximal to the calcaneal insertion. This region of diminished vascularity correlates precisely with the most frequent site of spontaneous rupture and is highly susceptible to degenerative tendinosis. The paratenon, a highly vascularized connective tissue sheath surrounding the tendon, provides the majority of the extrinsic blood supply to this watershed area. Preservation of the paratenon during surgical intervention is paramount to ensure adequate healing and minimize the risk of postoperative skin necrosis and deep infection.
Sural Nerve Topography
A thorough understanding of the sural nerve anatomy is the absolute cornerstone of safe percutaneous Achilles tendon repair. The sural nerve provides sensory innervation to the lateral aspect of the hindfoot and foot. It typically courses distally in the posterior calf, running adjacent to the small saphenous vein. In the distal third of the leg, the nerve crosses the lateral border of the Achilles tendon. Cadaveric studies indicate that the nerve crosses the lateral border of the tendon at an average distance of 9.8 cm (range, 7 to 13 cm) proximal to the calcaneal insertion. During percutaneous or minimally invasive repair techniques, blind passage of sutures through the proximal tendon stump carries a significant risk of sural nerve entrapment, laceration, or tethering. Consequently, modern percutaneous techniques mandate specific maneuvers, such as the "sural nerve sweep" or the use of specialized protective jigs, to displace the nerve anteriorly and laterally away from the trajectory of the passing needles.

Indications and Contraindications
The management of acute Achilles tendon ruptures remains a topic of intense debate within the orthopedic community. The decision between nonoperative management, traditional open repair, and percutaneous/minimally invasive repair must be highly individualized, taking into account the patient's age, functional demands, medical comorbidities, and the chronicity of the injury. Percutaneous repair was originally described as a compromise between open surgery and conservative management, aiming to provide the optimal functional outcome of open repair—specifically, restoring tendon tension and maximizing push-off strength—while significantly decreasing the wound healing complications and skin breakdown historically associated with large longitudinal posterior incisions.
Recent literature suggests that minimally invasive surgery is less expensive, less time-demanding, and yields functional outcomes comparable to open repair in the surgical management of acute Achilles tendon ruptures. However, the surgeon must weigh these benefits against the slightly higher risk of iatrogenic neurologic complications, such as sural nerve injury, which are more frequent after percutaneous repair compared to open techniques where the nerve can be directly visualized and protected.
| Indication Category | Operative Management (Percutaneous or Open) | Non Operative Management |
|---|---|---|
| Patient Profile | Young, active individuals, high-demand athletes, manual laborers. | Elderly, sedentary individuals, patients with severe medical comorbidities (e.g., uncontrolled diabetes, severe peripheral vascular disease). |
| Injury Characteristics | Acute ruptures (< 3-4 weeks), delayed presentations where tendon ends do not appose in equinus. | Acute ruptures where ultrasound confirms excellent apposition of tendon ends in 20 degrees of plantarflexion. |
| Local Tissue Status | Healthy overlying skin envelope. | Poor skin integrity, active local infection, severe venous stasis disease. |
| Compliance | Capable of adhering to strict postoperative weight-bearing and rehabilitation protocols. | Unlikely to comply with surgical restrictions, but able to tolerate cast or functional brace immobilization. |
| Contraindications | Active systemic infection, severe peripheral arterial disease precluding wound healing. | Massive gap (> 5 cm) in chronic ruptures precluding functional healing without surgical reconstruction. |
Pre Operative Planning and Patient Positioning
Clinical Evaluation and Diagnostic Testing
The diagnosis of an acute Achilles tendon rupture is primarily clinical. Patients frequently present with a history of feeling a sudden blow to the posterior aspect of the leg, often describing an audible snap followed immediately by sharp pain and an inability to bear weight or push off the affected foot.
Physical examination reveals a palpable gap in the substance of the Achilles tendon in the acute setting. However, in delayed presentations, organizing hematoma and soft tissue edema may fill this defect, rendering palpation unreliable. It is a critical diagnostic pitfall to rely on active plantarflexion, as this motion is usually preserved due to the compensatory actions of the tibialis posterior, flexor hallucis longus, and flexor digitorum longus muscles.
The most reliable clinical tests rely on the mechanical discontinuity of the gastrocsoleus complex. The calf squeeze test, originally described by Simmonds in 1957 but frequently credited to Thompson, is performed with the patient prone and the ankles clear of the examination table. The examiner squeezes the fleshy, muscular belly of the calf. This action deforms the soleus and normally results in passive plantarflexion of the foot if the Achilles tendon is intact. An absence of plantarflexion indicates a complete rupture. The affected leg must always be compared to the contralateral uninjured leg to account for baseline laxity.
The knee flexion test (Matles test) is another highly sensitive diagnostic maneuver. With the patient prone and the ankles clear of the table, the patient is asked to actively flex both knees to 90 degrees. During this movement, an intact gastrocsoleus complex will maintain the foot in slight plantarflexion. Conversely, if the Achilles tendon is ruptured, the foot on the affected side will fall into neutral or frank dorsiflexion under the influence of gravity.
Imaging Modalities and Diagnostics
While the diagnosis is usually clinical, imaging studies are valuable for confirming the diagnosis, assessing the size of the tendon gap, and ruling out concomitant pathology. Plain lateral radiographs of the ankle should be obtained to rule out bony avulsion fractures of the calcaneal tuberosity. In the setting of a tendon rupture, radiographs may reveal an irregular configuration or obliteration of Kager's fat pad—the radiolucent, fat-filled triangular space located anterior to the Achilles tendon, posterior to the tibia, and superior to the calcaneus.
Ultrasonography is a highly effective, dynamic, and cost-efficient imaging modality. It allows for real-time assessment of the tendon gap and can be used dynamically to determine if the tendon ends appose when the foot is placed in plantarflexion, which is crucial information when considering nonoperative management. Magnetic Resonance Imaging (MRI) is the gold standard for detailed anatomical visualization. While not strictly necessary for acute, clinically obvious ruptures, MRI is invaluable for evaluating chronic, neglected ruptures, assessing the degree of tendinosis, and pre-operative planning for complex reconstructions requiring tendon transfers or V-Y advancements.

Operating Room Setup and Anesthesia
Once the decision for percutaneous surgical intervention is established, meticulous preoperative planning and patient positioning are required. An assessment of the patient's general health, vascular status, and skin condition must be documented. Surgery is typically performed under general anesthesia or regional anesthesia (spinal or sciatic/popliteal block).
The patient is positioned prone on the operating table. Care must be taken to pad all bony prominences, particularly the chest, iliac crests, and knees. The feet should be positioned extending just past the edge of the table to allow for unencumbered intraoperative manipulation of the ankle joint through a full range of motion. A thigh tourniquet is applied to provide a bloodless surgical field, although some surgeons prefer to operate without a tourniquet to continuously assess tissue perfusion and avoid ischemic complications. The entire lower extremity from the toes to the mid-thigh is prepped and draped in a standard sterile fashion.
Detailed Surgical Approach and Technique
Evolution of Percutaneous and Minimally Invasive Strategies
The percutaneous repair of the Achilles tendon has evolved significantly since its initial description. Early blind percutaneous techniques, such as the Ma and Griffith method, involved passing sutures through the skin and tendon without direct visualization. While effectively minimizing wound complications, these blind techniques were plagued by unacceptably high rates of sural nerve entrapment. This led to the development of minimally invasive, jig-assisted techniques (e.g., the Percutaneous Achilles Repair System [PARS] or the Achillon device). These modern systems utilize a small transverse or longitudinal incision directly over the rupture site, allowing for direct visualization of the tendon ends, evacuation of the fracture hematoma, and the introduction of a specialized jig deep to the paratenon to guide suture placement safely away from the sural nerve.
Incision and Hematoma Evacuation
The surgical technique begins with the identification of the palpable tendon defect. A 2 to 3 cm transverse or longitudinal incision is made directly over the palpable gap. Blunt dissection is carried down through the subcutaneous tissue to the level of the paratenon. The paratenon is carefully incised longitudinally, preserving its medial and lateral reflections to ensure adequate blood supply for subsequent tendon healing.
Upon entering the paratenon sheath, the fracture hematoma is encountered and thoroughly evacuated using suction and blunt sweeping motions. The organized hematoma and frayed, degenerative margins of the ruptured tendon ends are minimally debrided. Aggressive debridement should be avoided in acute repairs, as the mop-end morphology of the tendon rupture provides essential surface area for healing and biological integration.
Instrumentation and Jig Placement
With the tendon ends visualized, the proximal stump is grasped with an Allis clamp or strong toothed forceps and placed under gentle distal traction. The specialized percutaneous jig is then introduced into the paratenon sheath, sliding proximally along the anterior and posterior surfaces of the proximal tendon stump. It is imperative that the jig is placed strictly within the paratenon but extra-tendinous to avoid iatrogenic damage to the tendon substance.
Suture Passing and Sural Nerve Protection
Once the jig is fully seated proximally, the passing pins or needles are introduced through the designated guide holes. To mitigate the risk of sural nerve injury during this critical step, the surgeon must perform a "sural nerve sweep." This involves making a small stab incision at the level of the lateral guide hole and using a blunt hemostat to gently sweep the subcutaneous tissues anteriorly and laterally, physically displacing the sural nerve away from the trajectory of the passing needle.
High-tensile strength, non-absorbable, multi-strand sutures (e.g., #2 or #5 ultra-high-molecular-weight polyethylene) are passed transversely through the proximal tendon stump at multiple levels. Modern jigs allow for the creation of a locking, Krackow-equivalent suture configuration percutaneously. After the proximal sutures are passed, the jig is carefully withdrawn distally, pulling the suture ends out through the central rupture incision.
The process is then repeated for the distal tendon stump. The jig is inserted distally toward the calcaneal insertion, and sutures are passed through the distal tendon. Because the distal stump is shorter and the sural nerve typically courses further lateral at this level, the risk of nerve injury is lower, but vigilance must be maintained.

Tendon Reduction and Knot Tying
With both the proximal and distal sutures exiting the central paratenon incision, the critical step of tendon reduction and tensioning is performed. The ankle is placed in approximately 15 to 20 degrees of plantarflexion to approximate the tendon ends and replicate the resting tension of the uninjured contralateral limb. The sutures from the proximal and distal stumps are paired and tied using secure, low-profile knots.
The surgeon must directly visualize the tendon ends during knot tying to ensure intimate apposition without overriding or bunching of the tendon fibers. The resting tension of the repaired tendon is confirmed by performing a squeeze test on the table and comparing the cascade of the foot to the contralateral side. Once secure fixation is achieved, the paratenon is meticulously closed over the repair site using an absorbable suture (e.g., 3-0 Vicryl) to restore the gliding layer and provide a vascularized bed for healing. The subcutaneous tissues and skin are closed in a layered, tension-free manner.
Complications and Management
Despite the advantages of percutaneous repair, complications can and do occur. The surgeon must be adept at recognizing and managing these issues to optimize patient outcomes.
Iatrogenic Neurologic Injury
The most significant complication unique to percutaneous Achilles repair is iatrogenic injury to the sural nerve. This can manifest as transient neuropraxia, painful neuroma formation, or permanent sensory loss along the lateral aspect of the foot. The incidence of sural nerve injury is significantly higher in blind percutaneous techniques compared to open repair. However, the advent of jig-assisted techniques and the routine use of the blunt dissecting "sural nerve sweep" have reduced this risk to levels comparable to open surgery. If a patient presents postoperatively with severe, radiating lateral foot pain suggestive of a tethered nerve, early re-exploration and neurolysis may be indicated.
Rerupture and Tendon Elongation
Rerupture is a devastating complication that historically occurred more frequently with nonoperative management but remains a risk with any surgical repair. The rerupture rate following percutaneous repair is generally reported between 2% and 5%. Reruptures typically occur within the first 12 weeks postoperatively, often due to patient noncompliance or an unexpected slip or fall. Management of a rerupture usually necessitates an open surgical approach, often requiring V-Y fascial advancement, turndown flaps, or flexor hallucis longus (FHL) tendon transfer to bridge the resultant gap and augment the repair.
Tendon elongation is a more subtle but equally detrimental complication. If the tendon heals in an elongated position, the length-tension relationship of the gastrocsoleus complex is permanently altered, resulting in a persistent loss of terminal plantarflexion power and an inability to perform a single-leg heel raise. This underscores the critical importance of tying the repair sutures with the ankle in adequate plantarflexion and adhering strictly to postoperative bracing protocols.
| Complication | Estimated Incidence (Percutaneous) | Etiology and Risk Factors | Prevention and Salvage Strategies |
|---|---|---|---|
| Sural Nerve Injury | 2% - 10% (lower with modern jigs) | Blind suture passage, anatomical variation, tethering by suture loop. | Prevention: Sural nerve sweep, jig-assisted techniques. Salvage: Early exploration, suture removal, neurolysis. |
| Rerupture | 2% - 5% | Noncompliance, early unprotected weight-bearing, traumatic fall. | Prevention: Rigid adherence to rehab protocols, secure multi-strand locking sutures. Salvage: Open reconstruction, FHL transfer, V-Y advancement. |
| Deep Infection | < 1% | Poor skin envelope, diabetes, smoking, paratenon damage. | Prevention: Meticulous soft tissue handling, extra-tendinous jig placement. Salvage: Aggressive I&D, IV antibiotics, potential flap coverage. |
| Tendon Elongation | 5% - 10% | Tying sutures in insufficient plantarflexion, aggressive early stretching. | Prevention: Tie sutures in 15-20 degrees equinus, verify resting tension intraoperatively. Salvage: Late shortening osteotomy or tendon imbrication (rarely indicated, highly complex). |
| Venous Thromboembolism | 1% - 5% | Immobilization, hypercoagulable state, tourniquet use. | Prevention: Early mobilization, chemical prophylaxis in high-risk patients. Salvage: Therapeutic anticoagulation (LMWH or DOACs). |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is arguably as critical to the final functional outcome as the surgical execution itself. Historically, patients were immobilized in a rigid equinus cast for 6 to 8 weeks, which reliably protected the repair but led to profound calf atrophy, joint stiffness, and prolonged recovery times.
Early Functional Rehabilitation
Modern protocols emphasize early functional rehabilitation, which has been shown to stimulate collagen synthesis, improve tendon fiber alignment, and reduce the time to return to work and sports. Immediately postoperatively, the patient is placed in a well-padded splint in 20 degrees of plantarflexion and kept non-weight-bearing for the first 2 weeks to allow for initial soft tissue healing and incision sealing.
Phased Recovery Timeline
At the 2-week postoperative mark, the splint is removed, the incision is inspected, and sutures are removed. The patient is then transitioned into a rigid functional walking boot equipped with a heel lift system (typically three wedges, equating to approximately 20-30 degrees of plantarflexion). Progressive weight-bearing is initiated as tolerated.
Over the subsequent 4 to 6 weeks, the wedges are systematically removed—usually one wedge every 10 to 14 days—gradually bringing the ankle to a neutral position. During this phase, active plantarflexion and controlled, active-assisted dorsiflexion to neutral are encouraged, but passive stretching into dorsiflexion is strictly prohibited to prevent tendon elongation.
By 6 to 8 weeks, the boot is typically discontinued, and the patient transitions to normal footwear, often utilizing a small silicone heel cup for comfort. Formal physical therapy intensifies, focusing on concentric and eccentric strengthening of the gastrocsoleus complex, proprioceptive training, and gait normalization. Return to light jogging is generally permitted around 12 to 16 weeks, while unrestricted return to high-impact sports and explosive activities may require 6 to 9 months, contingent upon the restoration of symmetric calf strength and the ability to perform repetitive single-leg heel raises without fatigue.
Summary of Key Literature and Guidelines
The paradigm of Achilles tendon rupture management has shifted significantly over the past two decades, heavily influenced by high-quality randomized controlled trials and meta-analyses.
Evidence Based Practice
A landmark study by Willits et al. (JBJS, 2010) challenged the traditional dominance of surgical intervention. This randomized controlled trial demonstrated that when acute Achilles tendon ruptures are treated with an accelerated functional rehabilitation protocol, the rerupture rates between operative and nonoperative management are statistically comparable, while nonoperative management avoids all surgical complications. This study established functional rehabilitation as a viable and highly effective standard of care.
However, subsequent meta-analyses, such as those by Soroceanu et al. (JBJS, 2012), have refined these conclusions. While confirming that early functional rehab normalizes rerupture rates between open and nonoperative groups, these analyses also demonstrated that surgical repair provides statistically significant advantages in restoring terminal push-off strength, reducing the incidence of tendon elongation, and facilitating an earlier return to physically demanding occupations and sports.
The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines reflect this nuanced evidence base. The guidelines support both operative and nonoperative management, emphasizing that the decision must be shared with the patient. When surgery is elected, the guidelines note that minimally invasive and percutaneous techniques offer a distinct advantage over traditional open repairs by significantly reducing the rate of superficial and deep wound infections, provided the surgeon employs meticulous techniques to protect the sural nerve.
In conclusion, percutaneous Achilles tendon repair represents a powerful tool in the orthopedic surgeon's armamentarium. By combining the biomechanical advantages of surgical tensioning with the biological benefits of a minimally invasive tissue-sparing approach, percutaneous repair optimizes functional recovery while mitigating the catastrophic wound complications that have historically plagued this challenging clinical entity.
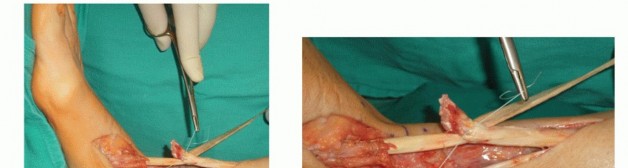
Clinical & Radiographic Imaging
You Might Also Like