Endoscopic Management of Snapping Hip Syndrome: An Intraoperative Masterclass

Key Takeaway
Welcome to the operating theater, fellows. Today, we're tackling symptomatic snapping hip syndrome. This masterclass will guide you through the intricate anatomy, meticulous preoperative planning, and precise endoscopic techniques for both iliopsoas and iliotibial band release. We'll cover crucial intraoperative execution, potential pitfalls, and comprehensive postoperative management, ensuring optimal patient outcomes for this often debilitating condition.
Comprehensive Introduction and Patho-Epidemiology
Welcome to this definitive masterclass on the endoscopic management of snapping hip syndrome. In the fascinating, yet historically frustrating realm of hip preservation surgery, few conditions present as dynamically and variably as snapping hip syndrome, formally designated in the orthopedic nomenclature as Coxa Saltans. This condition is far more than a simple, benign articular click; for our symptomatic patient demographic—often high-demand athletes, dancers, and active professionals—it manifests as a source of significant, debilitating pain and profound functional limitation. Our mandate as orthopedic surgeons is to thoroughly deconstruct its pathophysiological nuances, accurately differentiate its etiologies, and master the advanced endoscopic techniques required for its definitive surgical correction.
Historically, the clinical entity of Coxa Saltans was rigorously detailed and popularized by Allen and his colleagues, who meticulously described the distinct anatomical variants of this snapping phenomenon. Initially, the orthopedic community categorized this dynamic pathology into two primary extra-articular classifications: the Internal Type, which intricately involves the iliopsoas tendon complex, and the External Type, which is driven by the iliotibial band (ITB) and its dynamic relationship with the greater trochanter. This binary classification served as the foundational framework for decades of open surgical interventions, guiding our understanding of the extra-articular tendinous mechanics that generate the characteristic auditory and palpable snapping.
In contemporary hip preservation practice, a third category—the Intra-articular Type—has been widely recognized and integrated into our diagnostic algorithms. This classification serves as a critical catch-all for a multitude of intra-articular lesions, including acetabular labral tears, chondral delaminations, ligamentum teres avulsions, and intra-articular loose bodies, all of which can clinically mimic or concomitantly contribute to the mechanical snapping sensations reported by the patient. This evolution in our understanding underscores the absolute necessity of an exhaustive, multimodal diagnostic workup. However, for the purposes of this specific operative masterclass, our primary surgical focus will remain intensely concentrated on the extra-articular dynamic tendinous phenomena of the iliopsoas and the iliotibial band, and their state-of-the-art endoscopic management.
The epidemiological profile of symptomatic Coxa Saltans reveals a strong predilection for specific patient populations. While asymptomatic, incidental snapping of the iliopsoas or ITB is highly prevalent—estimated to occur in at least 10% to 15% of the general active population—the conversion to a symptomatic, pain-generating state is usually insidious. It is frequently precipitated by repetitive microtrauma, biomechanical overload, or acute macrotrauma. Dancers, martial artists, and long-distance runners are disproportionately affected due to the extreme ranges of hip flexion, abduction, and external rotation required by their disciplines. Understanding this patho-epidemiology is critical, as it directly informs our surgical decision-making, emphasizing the need for tissue-sparing endoscopic techniques that allow these high-demand patients to return to their elite functional baselines.
Detailed Surgical Anatomy and Biomechanics
Before we even consider establishing our endoscopic portals, we must meticulously review and internalize the complex three-dimensional anatomy of the peritrochanteric and anterior hip spaces. A profound, almost instinctual understanding of this topographical landscape is paramount to both successful surgical execution and, crucially, the avoidance of catastrophic iatrogenic injury to the dense network of surrounding neurovascular structures.
The Iliopsoas Complex and Internal Coxa Saltans
The iliopsoas complex functions as the most formidable and primary flexor of the hip joint, representing a sophisticated anatomical fusion of two distinct muscle bellies: the psoas major and the iliacus. The psoas major originates proximally from the transverse processes, lateral aspects of the vertebral bodies, and the intervertebral discs spanning from T12 down to L5. This extensive, deep retroperitoneal origin perfectly explains why a subset of our patients presenting with distal iliopsoas tendinopathy or snapping may paradoxically report referred flank, lower lumbar, or sacroiliac discomfort. The iliacus, conversely, originates from the superior two-thirds of the expansive iliac fossa, the sacral ala, and the anterior sacroiliac ligaments, forming a broad, fleshy muscle belly that converges with the psoas.
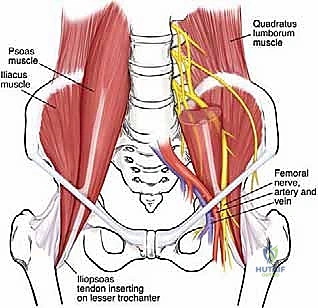
As these two powerful muscles descend toward the pelvic brim, they begin a complex convergence. The psoas tendon typically forms first, just proximal to the level of the inguinal ligament. As it crosses the joint, it undergoes a fascinating and surgically relevant 90-degree rotation: its anterior surface comes to lie medially, while its posterior surface rotates laterally. An accessory tendon originating from the iliacus frequently joins this evolving complex. These tendinous structures ultimately fuse to form the robust enthesis of the iliopsoas, which fans out to insert firmly over the lesser trochanter of the proximal femur. Crucially for the endoscopic surgeon, a significant portion of the lateral iliacus muscle fibers remains distinctly separate from the main tendon, attaching directly to the anterior femoral shaft just anterior to the lesser trochanter; preserving these fleshy fibers during a tendinous release is vital for maintaining postoperative hip flexion strength.
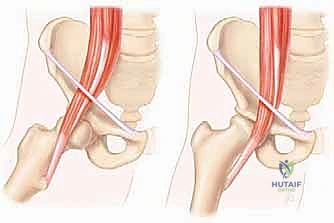
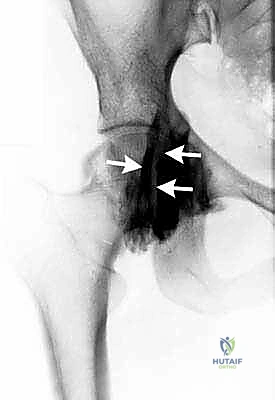
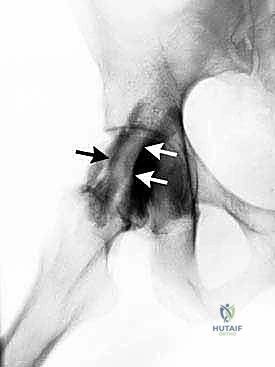
The biomechanical pathogenesis of internal snapping is intrinsically linked to the tendon's trajectory. As the iliopsoas exits the protective basin of the pelvis, it is redirected significantly—angling approximately 40 to 45 degrees—over the bony prominence of the pectineal eminence and the anterior capsule of the hip joint. The snapping event is a dynamic subluxation: as the hip transitions from a flexed, abducted, and externally rotated position into extension and internal rotation, the tensioned iliopsoas tendon abruptly translates from a lateral position to a medial position across the femoral head and pectineal eminence. This sudden, forceful translation against the bony or capsular ridge generates the classic, deep auditory "clunk" and the sharp, localized pain characteristic of internal Coxa Saltans.
The Iliotibial Band and External Coxa Saltans
Transitioning to the lateral compartment, the fascia lata represents a robust, inelastic fibromuscular sheath that circumferentially envelops the entire hip and thigh region. Renowned anatomist A.K. Henry eloquently described this fascial structure as the "pelvic deltoid," a highly accurate metaphor reflecting its extensive, multi-layered coverage and stabilizing function, much like the deltoid muscle envelops the glenohumeral joint. This dense fascia encases three key superficial muscles in the proximal thigh: the tensor fascia lata (TFL) anteriorly, the sartorius medially, and the gluteus maximus posteriorly.
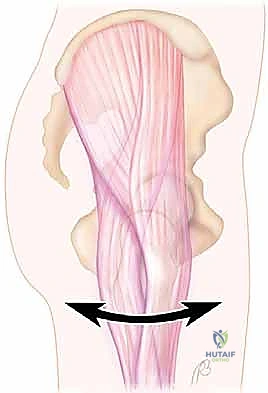
The iliotibial band itself is not a standalone tendon, but rather a thickened, longitudinal confluence of the fascial insertions of the tensor fascia lata and the superficial fibers of the gluteus maximus. It courses distally down the lateral aspect of the thigh to insert on Gerdy's tubercle of the proximal anterolateral tibia. In the peritrochanteric space, the ITB acts as a critical lateral stabilizer of the pelvis during the single-leg stance phase of the gait cycle. The deep fibers of the gluteus maximus also contribute to this complex by inserting directly into the proximal femur at the gluteal tuberosity, creating a tethering effect that influences the tension of the overlying ITB.
The pathogenesis of external snapping hip syndrome is defined by the abrupt, mechanical flipping of a thickened portion of the ITB—or occasionally the anterior border of the gluteus maximus or gluteus medius—back and forth across the prominent apex of the greater trochanter. In a state of hip extension, the thickened, tensioned posterior border of the ITB lies firmly posterior to the greater trochanter. As the hip initiates flexion, the ITB is dragged anteriorly; when the tension overcomes the friction of the trochanteric prominence, the band snaps violently forward. This mechanical friction syndrome invariably leads to secondary inflammation of the underlying greater trochanteric bursa, resulting in the localized lateral hip pain that drives the patient to seek surgical intervention.
Intra-articular Considerations and the Capsulolabral Interface
While our focus remains extra-articular, a masterful endoscopic surgeon must intimately understand the relationship between the extra-articular snapping structures and the intra-articular capsulolabral complex. The anterior capsule of the hip joint is intimately blended with the overlying iliopsoas muscle and tendon; in fact, the iliopsoas bursa, the largest bursa in the human body, communicates directly with the intra-articular space in up to 15% of normal adult hips. This anatomical proximity means that chronic internal snapping can induce secondary capsular inflammation, labral irritation, or even focal chondral damage at the anterior rim of the acetabulum due to the repetitive, concussive force of the snapping tendon.
Furthermore, when performing a transcapsular endoscopic release of the iliopsoas—a technique we will detail extensively—the surgeon must navigate the delicate interface between the peripheral compartment of the hip joint and the extra-articular psoas tunnel. The zona orbicularis, a distinct circular band of capsular fibers surrounding the femoral neck, serves as a critical intraoperative landmark. The iliopsoas tendon lies immediately anterior to the capsule at the level of the peripheral compartment. An overly aggressive capsulotomy or careless radiofrequency ablation in this region risks not only iatrogenic damage to the labrum but also catastrophic injury to the femoral neurovascular bundle, which lies mere millimeters anterior to the psoas tendon sheath.
Therefore, a profound respect for the capsulolabral interface is mandatory. The surgeon must utilize precise, controlled movements, relying on tactile feedback and high-definition endoscopic visualization to separate the capsular tissue from the tendinous fibers. Understanding the dynamic interplay between the dynamic stabilizers (the muscles and tendons) and the static stabilizers (the capsule and labrum) is the hallmark of advanced hip preservation surgery, ensuring that resolving a snapping tendon does not inadvertently result in micro-instability of the hip joint.
Exhaustive Indications and Contraindications
The decision to proceed with endoscopic surgical intervention for Coxa Saltans must be approached with rigorous clinical judgment, grounded in a comprehensive evaluation of the patient's history, physical examination, and advanced imaging. Surgery is never prophylactic in this condition; it is strictly reserved for patients who have demonstrably failed a prolonged, meticulously supervised course of conservative management and who present with significant functional impairment.
Patient Selection Criteria
The absolute primary indication for endoscopic release of either the iliopsoas or the iliotibial band is recalcitrant, painful snapping that has completely failed to respond to a minimum of three to six months of dedicated non-operative therapy. This conservative regimen must have included targeted physical therapy focusing on core stabilization, pelvic tilt correction, and specific stretching protocols (e.g., Thomas stretch for iliopsoas, Ober stretch for ITB), alongside non-steroidal anti-inflammatory drugs (NSAIDs), activity modification, and at least one image-guided (ultrasound or fluoroscopy) corticosteroid injection into the respective bursa or tendon sheath.
Furthermore, the snapping must be consistently reproducible on clinical examination and directly correlate with the patient's primary pain complaint. For internal snapping, the pain is typically localized to the deep anterior groin, exacerbated by bringing the hip from flexion/abduction/external rotation into extension/internal rotation. For external snapping, the pain is localized over the greater trochanter, often visible as a pseudo-subluxation event during active flexion and extension. Crucially, the patient must experience a temporary but profound relief of their specific symptoms following a diagnostic local anesthetic injection into the psoas bursa or the trochanteric bursa; this positive response is considered pathognomonic and serves as the ultimate green light for surgical intervention.
Contraindications and Relative Exclusions
Contraindications to endoscopic management of snapping hip syndrome must be strictly respected to avoid disastrous clinical outcomes. Absolute contraindications include the presence of active local or systemic infection, severe, advanced osteoarthritis of the hip joint (Tonnis Grade 2 or 3), and profound, uncorrected underlying biomechanical abnormalities such as severe femoral retroversion or acetabular dysplasia (lateral center edge angle < 20 degrees). In dysplastic patients, the iliopsoas and ITB often act as critical secondary stabilizers of the hip joint; releasing them can precipitate catastrophic, rapid-onset micro-instability and accelerated joint degeneration.
Relative contraindications include a history of multiple previous open surgical procedures in the affected anatomical region, which can result in dense, unyielding scar tissue that distorts the delicate neurovascular anatomy and makes endoscopic navigation exceptionally hazardous. Additionally, patients with profound, unmanaged psychiatric comorbidities or those exhibiting secondary gain motivations (e.g., complex worker's compensation cases) are generally poor candidates, as their subjective perception of pain and willingness to adhere to the rigorous postoperative rehabilitation protocol are often significantly compromised.
| Parameter | Internal Snapping Hip (Iliopsoas) | External Snapping Hip (Iliotibial Band) |
|---|---|---|
| Primary Indication | Painful anterior groin snapping failing >6 months conservative care. | Painful lateral trochanteric snapping failing >6 months conservative care. |
| Diagnostic Confirmation | Positive response to image-guided psoas bursa injection. | Positive response to image-guided trochanteric bursa injection. |
| Concomitant Pathology | Frequently associated with anterior labral tears or FAI. | Frequently associated with greater trochanteric pain syndrome (GTPS) or gluteus medius tears. |
| Absolute Contraindication | Severe acetabular dysplasia (LCEA < 20°); active infection. | Active infection; severe hip osteoarthritis. |
| Relative Contraindication | Previous open anterior hip surgery; profound generalized hyperlaxity. | Previous open lateral hip surgery; severe abductor deficiency. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning and flawless operating room setup are the invisible pillars upon which surgical success rests. The endoscopic environment is unforgiving; a poorly positioned patient or inadequate pre-operative imaging can rapidly transform a routine tendinous release into an intraoperative nightmare characterized by poor visualization, spatial disorientation, and heightened risk to the patient.
Advanced Imaging and Pre-Operative Templating
While the diagnosis of Coxa Saltans is fundamentally clinical, advanced imaging is an absolute prerequisite prior to any surgical intervention. Plain radiographs, including an AP pelvis, Dunn lateral, and false profile view, are mandatory to evaluate for underlying osseous abnormalities such as femoroacetabular impingement (FAI), coxa vara, or subtle dysplastic morphology. These bony parameters dictate the safety and efficacy of our soft tissue releases.
Magnetic Resonance Imaging (MRI), preferably a high-resolution non-contrast 3T scan or a Magnetic Resonance Arthrogram (MRA), is the gold standard for evaluating the soft tissue envelope. For the internal snapping hip, the MRI allows us to assess the integrity of the anterior labrum, the volume of the iliopsoas muscle belly, and the presence of any fluid within the iliopsoas bursa. For the external snapping hip, we meticulously evaluate the axial and coronal sequences for thickening of the ITB, fluid within the greater trochanteric bursa, and crucially, the integrity of the gluteus medius and minimus insertions on the greater trochanter. Pre-operative templating involves measuring the distance from standard arthroscopic portals to the anticipated site of pathology, ensuring our instrumentation will have adequate reach and trajectory.
Dynamic real-time ultrasonography has emerged as an invaluable adjunct in our pre-operative arsenal. It allows the surgeon to directly visualize the dynamic snapping event in real-time. We can observe the iliopsoas tendon abruptly translating over the pectineal eminence or the ITB snapping forcefully over the greater trochanter. This dynamic visual confirmation, coupled with the ability to perform a simultaneous targeted diagnostic injection, provides unparalleled diagnostic certainty and aids in precise surgical planning.
Anesthesia, Patient Positioning, and Operating Room Setup
The choice of anesthesia and patient positioning is dictated by the specific type of snapping hip and the surgeon's preferred approach. Endoscopic hip surgery is typically performed under general anesthesia with profound muscle relaxation, which is essential to overcome the massive forces of the hip musculature and allow for adequate joint distraction if intra-articular work is required.
For the internal snapping hip, the patient is almost universally positioned supine on a specialized hip distraction table. The operative leg is secured in a well-padded traction boot, and the perineal post is carefully positioned against the medial thigh to avoid pudendal nerve neuropraxia. Even if we are planning an extra-articular lesser trochanteric release, having the patient on a traction table allows for seamless transition to intra-articular arthroscopy should concomitant labral pathology need to be addressed. The hip is typically positioned in neutral rotation, slight extension, and 10 to 15 degrees of abduction. Fluoroscopy is brought in from the contralateral side, positioned to provide unhindered AP and lateral views of the operative hip.

For the external snapping hip, the patient is classically positioned in the lateral decubitus position on a standard radiolucent operating table, firmly secured with a beanbag or pegboard system. The operative leg is draped free, allowing the surgeon to dynamically flex, extend, and rotate the hip during the procedure to reproduce the snap and confirm the adequacy of the release in real-time. The fluoroscopy C-arm is draped and positioned to allow for orthogonal views of the greater trochanter. Meticulous padding of all bony prominences, particularly the contralateral fibular head and axilla, is mandatory to prevent positioning-related neuropraxias during these potentially lengthy endoscopic cases.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the endoscopic release requires a mastery of spatial orientation, precise portal placement, and meticulous soft tissue handling. The techniques described below represent the current state-of-the-art in hip preservation surgery, designed to maximize surgical efficacy while minimizing iatrogenic morbidity.
Endoscopic Iliopsoas Release Techniques
For the internal snapping hip, the surgeon must choose between three primary endoscopic approaches: the transcapsular release at the level of the joint line, the endoscopic release at the lesser trochanter, or the central compartment release. The transcapsular approach is currently the most widely utilized, particularly when concomitant intra-articular pathology exists.


The procedure begins with the establishment of standard anterolateral (AL) and mid-anterior (MAP) portals under fluoroscopic guidance. Once intra-articular access is achieved, a thorough diagnostic arthroscopy is performed. To access the iliopsoas tendon, an anterior capsulotomy is created using a radiofrequency ablation wand, extending from the 2 o'clock to the 3 o'clock position (in a right hip), just distal to the anterior labrum. This exposes the underlying iliopsoas tendon sheath.



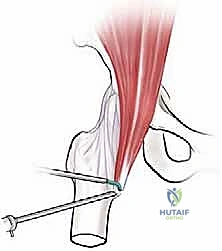
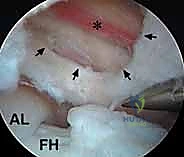
The tendon sheath is carefully opened, revealing the distinct, pearlescent white tendinous portion of the iliopsoas lying anterior to the red, fleshy muscle belly of the iliacus. It is absolutely critical to isolate only the tendinous portion. Using a curved arthroscopic shaver or radiofrequency wand, the tendinous fibers are meticulously transected from medial to lateral. As the tendon is released, the underlying iliacus muscle belly will immediately bulge anteriorly, filling the defect. This selective tenotomy ensures the elimination of the snapping cord while preserving the muscular continuity of the iliacus, thereby preventing catastrophic postoperative hip flexion weakness.



Alternatively, the lesser trochanteric release is performed entirely extra-articularly. Portals are established distally, guided by fluoroscopy to target the lesser trochanter. The iliopsoas bursa is entered, and the tendon is visualized at its direct insertion onto the bone. This approach is highly effective for isolated snapping without intra-articular pathology but carries a theoretically higher risk to the medial femoral circumflex artery branches if the dissection strays too far posteriorly or medially.



Endoscopic Iliotibial Band Lengthening and Release
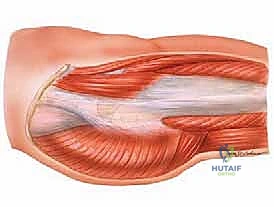
The endoscopic management of the external snapping hip aims to relieve the mechanical tension of the ITB over the greater trochanter while preserving the overall structural integrity of the lateral fascial envelope. With the patient in the lateral decubitus position, proximal and distal peritrochanteric portals are established, typically 3 to 4 centimeters proximal and distal to the vastus ridge, aligned with the longitudinal axis of the femur.

The arthroscope is introduced into the peritrochanteric space, superficial to the greater trochanteric bursa but deep to the ITB. An extensive bursectomy is performed using a 4.5mm or 5.5mm motorized shaver to clear the inflammatory tissue and clearly delineate the deep surface of the ITB and the underlying insertions of the gluteus medius and minimus. Once a clear visual field is established, the thickened, snapping portion of the ITB is identified.



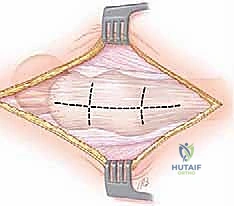
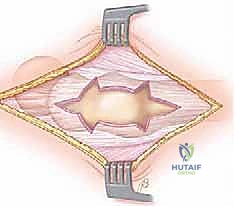
The release is typically performed using a radiofrequency wand to create a cruciate or diamond-shaped defect in the ITB directly over the maximal prominence of the greater trochanter. The longitudinal cut is made first, parallel to the fibers of the ITB, followed by a transverse cut. The edges of the fascial defect will immediately retract, creating a window. The operative leg is then dynamically taken through a full range of motion—flexion, extension, internal, and external rotation—while visualizing the defect endoscopically. The surgeon must confirm that the edges of the ITB window no longer impinge upon or snap across the greater trochanter during these provocative maneuvers.