Magnetic Resonance Imaging in Shoulder Pathology: Diagnosis & Surgical Insights
Key Takeaway
Magnetic Resonance Imaging (MRI) is crucial for diagnosing complex shoulder pathologies by offering superior soft tissue contrast. It accurately identifies rotator cuff tears, labral lesions, glenohumeral instability, and inflammation, guiding surgical decision-making and distinguishing between various sources of shoulder pain where clinical differentiation is challenging.
Pinpoint Shoulder Pain with Magnetic Resonance Imaging
Introduction & Epidemiology
Accurate diagnosis of shoulder pathology necessitates a systematic approach, commencing with a comprehensive history and physical examination. This clinical foundation is then augmented by appropriate imaging modalities, which are critical for confirming a presumptive diagnosis, delineating the extent of injury, and guiding treatment strategies—both non-operative and operative. Understanding the distinct advantages and limitations of various imaging techniques is paramount to optimizing diagnostic accuracy while minimizing redundant investigations and healthcare costs.
Shoulder pain is a prevalent musculoskeletal complaint, affecting a significant portion of the adult population, with reported lifetime prevalence rates ranging from 7% to 26%. Conditions leading to shoulder pain are diverse, encompassing rotator cuff tendinopathy and tears, glenohumeral instability (labral tears, capsular laxity), adhesive capsulitis, acromioclavicular (AC) joint pathology, biceps tendinopathy, and degenerative changes. The incidence of rotator cuff tears, for instance, increases significantly with age, with partial- or full-thickness tears observed in over 50% of individuals over 60 years old. Glenohumeral instability is more common in younger, active populations. The precise identification of the anatomical source of pain is crucial, as overlapping symptom profiles can make clinical differentiation challenging. Magnetic Resonance Imaging (MRI), with or without arthrography, has emerged as a cornerstone in the diagnostic armamentarium for many of these complex shoulder pathologies, offering superior soft tissue contrast compared to conventional radiography and computed tomography (CT). This chapter details the utility of various imaging options in diagnosing shoulder pathology, with a particular emphasis on MRI, and integrates these diagnostic insights into the framework of surgical decision-making, technique, and post-operative management.
Surgical Anatomy & Biomechanics
A thorough understanding of shoulder anatomy and biomechanics is fundamental to interpreting imaging findings and executing effective surgical interventions. The shoulder complex is comprised of four joints: the glenohumeral (GH), acromioclavicular (AC), sternoclavicular (SC), and scapulothoracic articulation. The glenohumeral joint, a diarthrodial ball-and-socket joint, provides the greatest range of motion of any joint in the body, owing to the significant mismatch between the large humeral head and the shallow glenoid fossa.
Bony Anatomy
- Humerus: The proximal humerus includes the humeral head, anatomical and surgical necks, greater and lesser tuberosities, and the bicipital groove. These landmarks are critical for identifying fracture patterns and attachment sites for the rotator cuff and biceps tendons.
- Scapula: Comprises the glenoid fossa (cartilage-covered and deepened by the labrum), coracoid process, acromion, and scapular body. The acromion morphology (Type I, II, III) is relevant in subacromial impingement.
- Clavicle: Articulates with the acromion laterally (AC joint) and the sternum medially (SC joint). Provides a strut for upper extremity suspension.
Soft Tissue Anatomy
- Rotator Cuff: Consists of four muscles: supraspinatus (initiates abduction), infraspinatus (external rotation), teres minor (external rotation), and subscapularis (internal rotation). These tendons form a continuous cuff around the humeral head, providing dynamic stability and movement. Their integrity is frequently assessed by MRI.
- Glenoid Labrum: A fibrocartilaginous ring that deepens the glenoid fossa by approximately 50%, enhancing glenohumeral stability. Tears (e.g., SLAP lesions, Bankart lesions) are common in instability.
- Capsule and Ligaments: The glenohumeral capsule is lax, allowing extensive motion. It is reinforced by the superior, middle, and inferior glenohumeral ligaments, which are critical static stabilizers, particularly the anterior band of the inferior glenohumeral ligament (IGHL) in external rotation and abduction.
- Biceps Tendon: The long head of the biceps tendon originates from the supraglenoid tubercle and superior labrum, traversing the bicipital groove. Pathology here (tendinopathy, tears, instability) is a frequent source of anterior shoulder pain.
- Subacromial Bursa: A fluid-filled sac reducing friction between the rotator cuff and the overlying acromion/coracoacromial ligament. Inflammation (bursitis) often accompanies rotator cuff pathology.
Biomechanics
Shoulder biomechanics involve a complex interplay of static and dynamic stabilizers.
*
Static Stabilizers:
Bony congruence, glenoid labrum, joint capsule, and glenohumeral ligaments.
*
Dynamic Stabilizers:
Rotator cuff muscles (compression of humeral head into glenoid), long head of biceps, and scapulothoracic musculature.
Proper scapular kinematics are essential for optimal glenohumeral function. Dysrhythmia can contribute to impingement and instability. Imaging, particularly MRI, allows for detailed assessment of these structures, revealing tears, inflammation, degenerative changes, and anatomical variations that predispose to pathology.
Indications & Contraindications
The decision to pursue surgical intervention for shoulder pathology is based on a confluence of clinical findings, patient factors, and imaging results. MRI plays a pivotal role in confirming the diagnosis, characterizing the extent of injury, and planning the operative approach.
General Indications for Shoulder Surgery
- Failed Non-Operative Management: Persistent pain and dysfunction despite an adequate trial of conservative measures (rest, activity modification, NSAIDs, physical therapy, injections).
- Acute Traumatic Injuries: Displaced fractures (proximal humerus, clavicle, scapula), acute, symptomatic full-thickness rotator cuff tears in active individuals, recurrent glenohumeral instability.
- Progressive Pathology: Conditions likely to worsen without intervention, such as large, symptomatic rotator cuff tears.
- Mechanical Symptoms: Locking, catching, or persistent instability.
- Neurological Deficits: Nerve impingement requiring decompression.
Specific Pathology and Imaging-Guided Indications
- Rotator Cuff Tears: MRI provides detailed information on tear size (full vs. partial thickness), retraction, muscle atrophy, fatty infiltration, and tendon quality. Surgical repair is typically indicated for symptomatic full-thickness tears, large partial-thickness tears (>50% thickness), or acute tears in younger, active patients.
- Glenohumeral Instability: MR arthrogram is superior for visualizing labral tears (Bankart, SLAP, ALPSA, Perthes lesions), capsular laxity, and associated bony defects (Hill-Sachs, bony Bankart). Surgical stabilization is indicated for recurrent instability, significant labral pathology, or large bony defects.
- Biceps Tendinopathy/Tears: MRI can identify tendinopathy, subluxation, partial tears, or complete ruptures of the long head of the biceps. Surgical options include tenotomy or tenodesis for persistent pain.
- Acromioclavicular Joint Pathology: While primarily diagnosed clinically and with radiographs, MRI can confirm severe AC joint arthritis, osteolysis, or chronic instability.
- Adhesive Capsulitis: Usually managed non-operatively, but MRI can help rule out other pathologies. In refractory cases, arthroscopic capsular release may be indicated.
- Proximal Humerus Fractures: Indicated for displaced, unstable fractures, especially in younger patients. MRI can assess associated soft tissue injuries, though CT is primary for bony detail.
- Shoulder Arthroplasty: Indicated for advanced glenohumeral arthritis, complex proximal humerus fractures in elderly patients, or irreparable rotator cuff arthropathy.
Contraindications to Shoulder Surgery
Absolute contraindications are rare and typically relate to the patient's overall medical status. Relative contraindications include:
*
Active Infection:
Requires eradication before elective surgery.
*
Severe Comorbidities:
Uncontrolled diabetes, severe cardiovascular or pulmonary disease, posing excessive anesthetic risk.
*
Unrealistic Patient Expectations:
Poor understanding of potential outcomes or recovery timeline.
*
Lack of Patient Compliance:
Inability or unwillingness to adhere to post-operative rehabilitation protocols.
*
Smoking:
Significant risk factor for impaired healing and complications.
Operative vs. Non-Operative Indications
| Condition | Primary Non-Operative Indications | Primary Operative Indications |
|---|---|---|
| Rotator Cuff Tear | Small partial-thickness tears, asymptomatic tears, low demand patients, failed non-op. | |
| Glenohumeral Instability | Initially non-operative physical therapy focused on peri-scapular muscle strengthening and rotator cuff exercises for first-time dislocations. | Recurrent dislocations, significant labral tears (Bankart, SLAP II+), bony Bankart or Hill-Sachs lesions >20% glenoid/humeral head engagement, failed non-op. |
| Biceps Tendinopathy | Rest, activity modification, NSAIDs, physical therapy, subacromial/biceps sheath injections. | Refractory pain from tendinopathy, symptomatic subluxation/dislocation of biceps, Popeye deformity (cosmetic/functional concerns), associated rotator cuff pathology. |
| AC Joint Arthritis | NSAIDs, activity modification, injections (steroid, PRP). | Persistent symptomatic arthritis despite non-operative treatment, osteolysis of distal clavicle. |
| Adhesive Capsulitis | Extensive physical therapy, NSAIDs, oral steroids, intra-articular steroid injections. | Refractory stiffness limiting function, particularly after 6-9 months of conservative management. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for successful shoulder surgery, optimizing outcomes and mitigating risks. This phase heavily relies on integrating clinical assessment with advanced imaging findings.
Imaging for Pre-Operative Planning
Radiography
Radiographs are the initial imaging modality for evaluation of the shoulder. They provide crucial information regarding bony architecture, alignment, and gross pathology.
* Provides little information on soft tissue around the shoulder.
* Shoulder series should consist of at least two orthogonal views.
* Trauma evaluation includes:
*
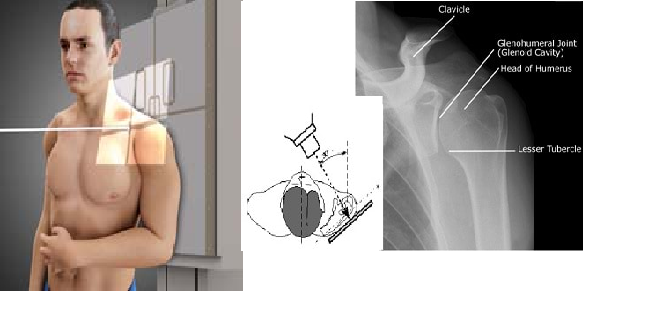
True anteroposterior (AP) aka Grashey (
▶
Fig.**
5.1
):
* Erect, sitting, or supine with patient rotated 30–45 degrees in relation to the image detector.
* Evaluate glenohumeral joint, fracture (proximal humerus, clavicle, scapula, and ribs), and proximal humeral migration.
* Fig. 5.1 Grashey.

*
Anteroposterior (AP)
: Standard AP view, often used in conjunction with Grashey.
* Fig. 5.2 Anteroposterior (AP).

*
Axillary View (West Point or Stryker Notch):
Essential for assessing glenoid bone loss, anterior glenoid rim fractures, and humeral head defects (e.g., Hill-Sachs lesions).
*
Scapular Y View:
For assessing glenohumeral dislocation direction and scapular body/neck fractures.
*
Zanca View:
Specifically for AC joint assessment, often with stress views.
* For advanced evaluation:
*

*

*

*

*

Computed Tomography (CT)
CT provides superior bony detail and is invaluable for:
* Complex fracture evaluation (proximal humerus, scapula, glenoid).
* Quantifying glenoid bone loss in recurrent instability.
* Assessing malunion or nonunion.
* Pre-operative planning for shoulder arthroplasty, including 3D reconstruction.
*

*

*

*

*

Magnetic Resonance Imaging (MRI) / MR Arthrography
MRI is the gold standard for soft tissue evaluation and is critical for "pinpointing" the precise pathology causing shoulder pain.
*
Rotator Cuff:
Highly sensitive and specific for full-thickness tears, partial-thickness tears, tendinopathy, and muscle atrophy/fatty infiltration. Helps assess tear pattern, size, and retraction, which are vital for surgical planning.
*
Labrum and Capsule:
Essential for diagnosing labral tears (Bankart, SLAP, anterior labroligamentous periosteal sleeve avulsion - ALPSA, Perthes lesions), capsular laxity, and glenohumeral ligament integrity. MR arthrography, involving intra-articular injection of gadolinium contrast, significantly enhances visualization of labral-ligamentous structures and articular cartilage, improving diagnostic yield for subtle tears or detachments.
*
Biceps Tendon:
Identifies tendinopathy, subluxation, instability, and tears of the long head of the biceps.
*
Bone Contusions/Edema:
Detects occult fractures, bone bruising, and stress reactions often associated with instability or trauma.
*
Cartilage Assessment:
While not as precise as arthroscopy, MRI can show chondral lesions, loose bodies, and early degenerative changes.
*
Fluid Collections:
Identifies joint effusions, bursitis, and paralabral cysts.
*

*

*

*

*

*

*

*

*

*

*

*

*

*

*

*

*

*

*

*

Patient Positioning
Proper patient positioning is critical for surgical access, visualization, and safety.
*
Beach Chair Position:
* Most common for arthroscopic and open shoulder procedures.
* Patient is semi-recumbent (30-70 degrees of trunk elevation).
* Head is secured in a headrest, ensuring neutral cervical spine alignment.
* The operative arm is draped free or suspended in a traction device, allowing for manipulation.
* Advantages: Familiar anatomical orientation, easy conversion to open procedures, ability to assess stability and range of motion.
* Disadvantages: Risk of cerebral hypoperfusion (especially in hypotensive patients), potential for brachial plexus stretch.
*
Lateral Decubitus Position:
* Patient lies on the contralateral side, secured with axillary and hip rolls.
* Operative arm is suspended in a traction device with weights, allowing for joint distraction.
* Advantages: Optimal joint distraction for arthroscopic working space, reduced risk of cerebral hypoperfusion, good visualization for posterior pathologies.
* Disadvantages: Positioning can be time-consuming, potential for nerve compression from traction, restricted access to anterior structures.
Detailed Surgical Approach / Technique
The surgical technique for shoulder pathology is dictated by the specific diagnosis, lesion characteristics, patient factors, and surgeon preference. MRI findings are instrumental in refining the operative strategy. Here, we outline general principles for common procedures.
Rotator Cuff Repair
Arthroscopic Rotator Cuff Repair
- Portals: Standard posterior viewing portal, anterosuperior, anteroinferior, lateral, and posterolateral working portals.
- Debridement: Bursectomy for improved visualization, debridement of torn tendon edges and footprint, acromioplasty if impingement is significant.
- Mobilization: Release adhesions and perform interval slides (e.g., supraspinatus, infraspinatus) to achieve tension-free repair.
- Footprint Preparation: Decortication of the greater tuberosity to promote healing.
-
Anchor Placement:
Single-row, double-row, or transosseous equivalent repair constructs.
- Single-row: Anchors placed medially, sutures passed through tendon and tied.
- Double-row: Medial row anchors for compression, lateral row anchors or suture bridges for broad footprint coverage and load sharing. MRI studies have demonstrated improved footprint restoration with double-row techniques in certain tear patterns.
- Suture Management: Knotless or knotted techniques for tendon fixation.
- Biceps Tenodesis/Tenotomy (if indicated): For associated long head of biceps pathology.
Glenohumeral Instability (Labral Repair)
Arthroscopic Bankart Repair
- Portals: Standard posterior viewing portal, anterosuperior and anteroinferior working portals.
- Assessment: Diagnostic arthroscopy confirms Bankart lesion (anterior-inferior labral avulsion) and assesses associated Hill-Sachs lesion, glenoid bone loss, and capsular laxity. MRI is critical pre-operatively to delineate these findings.
- Labral Mobilization: The torn labrum and capsuloligamentous complex are mobilized from the glenoid neck.
- Glenoid Preparation: Rasping or burring of the anterior glenoid neck to create a bleeding bed for healing.
- Anchor Placement: Multiple suture anchors (typically 3-5) are placed along the anterior-inferior glenoid rim.
- Suture Passage and Repair: Sutures are passed through the detached labrum and capsule, then tied to re-approximate the labral-ligamentous complex to the glenoid rim, restoring anterior stability and tensioning the capsule.
Arthroscopic SLAP Repair (Superior Labral Anterior Posterior)
- Portals: Standard posterior viewing portal, anterosuperior and anteroinferior working portals.
- Assessment: Diagnostic arthroscopy confirms SLAP tear, often involving the biceps anchor. MRI or MR arthrogram pre-operatively aids in classifying the SLAP lesion (e.g., Type II, IV).
- Labral Preparation: Debridement of unstable portions of the labrum and biceps, light abrasion of the superior glenoid.
- Anchor Placement: One or two suture anchors are typically placed in the superior glenoid, depending on tear length.
- Suture Passage and Repair: Sutures are passed through the torn superior labrum and biceps anchor, then tied to re-fixate the complex to the superior glenoid.
Latarjet Procedure (for Bony Glenoid Loss)
- Approach: Deltopectoral approach, often preferred for significant anterior glenoid bone loss (>20-25% on pre-operative CT).
- Coracoid Osteotomy: The coracoid process, with attached conjoined tendon, is osteotomized.
- Coracoid Transfer: The coracoid graft is transferred and fixed to the anterior glenoid rim with two bicortical screws. This provides a bony block effect and a sling effect from the conjoined tendon.
Complications & Management
Despite advances in surgical techniques and imaging, complications can occur. MRI often plays a role in post-operative evaluation of persistent symptoms.
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Rotator Cuff Tear | Partial tears (<50% thickness), small full-thickness tears (<1 cm), low-demand patients, good response to conservative treatment. | Rotator cuff tears with significant symptoms unresponsive to conservative management; symptomatic full-thickness tears (even small ones) in active patients; progressive tears. |
| Glenohumeral Instability | First-time dislocation without significant labral/bony damage, older patients, sedentary lifestyle, good response to bracing/PT. | Recurrent dislocations, significant labral tears (Bankart, SLAP Type II+), bony Bankart or Hill-Sachs defects >20-25% glenoid/humeral head engagement, failed non-op. |
| Biceps Tendinopathy | Mild to moderate pain, no mechanical symptoms, good response to physical therapy, injections. | Refractory pain despite conservative management, symptomatic subluxation/dislocation of biceps, significant partial tears (>50% thickness), complete tears in high-demand patients. |
| AC Joint Arthritis | Mild to moderate pain, responsive to NSAIDs, activity modification, steroid injections. | Persistent debilitating pain despite non-operative treatment, symptomatic distal clavicle osteolysis, significant chronic instability with pain. |
| Adhesive Capsulitis | Initial acute/painful phase, early stiffness phase, improvement with extensive physical therapy, injections. | Refractory stiffness after 6-9 months of aggressive non-operative treatment, significant functional limitation. |
General Complications
- Infection: Superficial or deep. Management involves antibiotics, debridement, and potentially hardware removal.
- Nerve Injury: Brachial plexus (most common), axillary nerve (deltoid paralysis), musculocutaneous nerve (biceps weakness). Often transient neuropraxia, but persistent deficits may require neurolysis or tendon transfers. Pre-operative MRI helps identify nerve variations or pre-existing compression.
- Vascular Injury: Rare but serious, involving axillary artery or vein.
- Stiffness (Adhesive Capsulitis): Post-operative incidence is higher in certain patient populations (diabetics). Managed with aggressive physical therapy, NSAIDs, steroid injections, or arthroscopic capsular release in refractory cases.
- Pain: Persistent or new pain. Requires thorough evaluation (including repeat imaging) to identify the cause.
- Hardware-related Issues: Anchor pull-out, suture failure, screw loosening. May require revision surgery.
Specific Complications
-
Rotator Cuff Repair:
- Re-tear: Most common. Risk factors include large tears, poor tendon quality, fatty infiltration (assessed by MRI), and older age. Management: repeat conservative treatment, revision repair (open or arthroscopic), or in irreparable cases, superior capsule reconstruction, latissimus dorsi transfer, or reverse total shoulder arthroplasty.
- Deltoid Detachment: Can compromise repair integrity and function.
-
Glenohumeral Instability Repair:
- Recurrent Instability: Failure of repair. Risk factors include significant unaddressed bone loss, young age, participation in contact sports, hyperlaxity. Management: revision surgery (arthroscopic or open Latarjet/bone block).
- Stiffness: Over-tightening of the capsule.
-
Biceps Tenodesis/Tenotomy:
- Continued Biceps Pain: If tenodesis fails or if a tenotomy leaves a prominent muscle belly.
- Popeye Deformity (tenotomy): Cosmetic concern.
-
Shoulder Arthroplasty:
- Infection, instability, glenoid loosening, humeral loosening, periprosthetic fracture, rotator cuff failure (for anatomic TSA). These are extensive and require dedicated discussion.
Post-Operative Rehabilitation Protocols
Rehabilitation is an integral component of successful surgical outcomes, guided by the type of surgery, repair integrity, and patient factors. The goal is to protect the repair while gradually restoring motion, strength, and function. Close communication between the surgeon and physical therapist is essential.
General Principles
- Protection Phase: Initial period focused on protecting the surgical repair, minimizing stress, and controlling pain/inflammation.
- Mobility Phase: Gradual restoration of passive and then active range of motion, adhering to specific ROM restrictions.
- Strengthening Phase: Progressive strengthening of rotator cuff and scapular stabilizer musculature.
- Return to Activity Phase: Sport-specific or work-specific training, culminating in full functional return.
Rotator Cuff Repair Rehabilitation (Example)
-
Phase I: Protection (Weeks 0-6)
- Goal: Protect repair, minimize pain, prevent stiffness.
- Immobilization: Sling worn continuously (except for hygiene and exercises) for 4-6 weeks, depending on tear size and repair security.
- Exercises: Passive range of motion (PROM) within prescribed limits (e.g., flexion to 90-120 degrees, external rotation to 0-30 degrees depending on tendon repaired). Pendulum exercises. Scapular setting exercises.
- Restrictions: No active range of motion (AROM), no lifting, no weight-bearing, no sudden movements.
-
Phase II: Controlled Motion (Weeks 6-12)
- Goal: Restore full passive range of motion, initiate active-assisted and active motion.
- Exercises: Progress to active-assisted ROM (AAROM) and gentle AROM. Isometric rotator cuff exercises. Light scapular strengthening.
- Restrictions: Avoid heavy lifting, overhead activities, or forceful movements.
-
Phase III: Strengthening (Weeks 12-24)
- Goal: Restore strength, endurance, and neuromuscular control.
- Exercises: Progressive resistive exercises for rotator cuff and scapular stabilizers. Begin functional exercises.
- Restrictions: Gradual return to activities.
-
Phase IV: Return to Activity (Months 6+ for high-demand)
- Goal: Optimize strength, power, and endurance for specific activities.
- Exercises: Sport-specific drills, plyometrics, advanced strengthening.
Labral Repair Rehabilitation (Example for Anterior Stabilization)
-
Phase I: Protection (Weeks 0-4)
- Goal: Protect repair, minimize pain.
- Immobilization: Sling for 3-4 weeks, often with external rotation limit (e.g., 10-20 degrees).
- Exercises: PROM within protected range (e.g., flexion to 90 degrees, external rotation to neutral). Pendulums, elbow/wrist/hand exercises.
-
Phase II: Controlled Motion (Weeks 4-12)
- Goal: Restore full ROM, initiate gentle strengthening.
- Exercises: Progress PROM, AAROM, AROM. Isometric rotator cuff and scapular strengthening.
- Restrictions: Avoid abduction with external rotation (anterior apprehension position).
-
Phase III: Strengthening (Weeks 12-24)
- Goal: Restore strength, endurance.
- Exercises: Progressive resistive exercises, proprioceptive training.
-
Phase IV: Return to Activity (Months 6+ for high-demand)
- Goal: Sport/work-specific training.
Summary of Key Literature / Guidelines
The field of orthopedic shoulder surgery is continuously evolving, with evidence-based guidelines shaping current best practices.
- American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines: Provide comprehensive recommendations for diagnosis and treatment of various shoulder conditions, including rotator cuff tears, glenohumeral instability, and adhesive capsulitis. These guidelines are regularly updated and synthesize the highest quality evidence. For example, the AAOS guidelines for rotator cuff repair emphasize the importance of patient factors, tear characteristics (size, retraction, fatty infiltration – all assessed by MRI), and the benefits of early surgical repair in specific populations.
- Arthroscopy Association of North America (AANA): Publishes numerous instructional articles and surgical technique videos, contributing to standardization and dissemination of arthroscopic procedures.
- Journal of Bone and Joint Surgery (JBJS), American Journal of Sports Medicine (AJSM), Journal of Shoulder and Elbow Surgery (JSES), Arthroscopy: The Journal of Arthroscopic and Related Surgery: These peer-reviewed journals are primary sources for cutting-edge research on shoulder pathology, surgical techniques, outcomes, and complications.
- MRI in Shoulder Diagnostics: Numerous studies have validated the high diagnostic accuracy of MRI, particularly MR arthrography, for labral and capsular lesions. Meta-analyses consistently report sensitivity and specificity in the range of 85-95% for detecting various soft tissue pathologies. The role of 3.0 Tesla MRI over 1.5 Tesla MRI continues to be investigated for improved resolution and diagnostic yield in subtle lesions.
- Biologic Augmentation: Research continues into the use of biologics (e.g., PRP, bone marrow aspirate concentrate, acellular dermal matrices) to enhance rotator cuff healing, with variable results and ongoing clinical trials.
- Rehabilitation Protocols: The emphasis in rehabilitation has shifted towards individualized, phase-specific protocols. Recent literature supports early passive motion for rotator cuff repairs and controlled, progressive strengthening for instability repairs.
In conclusion, the integration of a thorough clinical evaluation with advanced imaging, particularly MRI, is indispensable for pinpointing the source of shoulder pain, guiding surgical indications, refining operative planning, and optimizing post-operative management. Adherence to evidence-based guidelines and a deep understanding of anatomy and biomechanics are cornerstones for achieving successful outcomes in the surgical treatment of shoulder pathology.
