Posterior Shoulder Joint Approach: Anatomy, Indications, & Surgical Techniques
Key Takeaway
The posterior shoulder joint approach provides crucial access to the posterior glenoid and humeral head. It's indicated for complex pathologies like glenoid retroversion osteotomy, biopsy/excision of posterior glenoid tumors, and drainage of severe posterior shoulder joint infections, especially when extensive bone work or direct visualization is required beyond arthroscopic capabilities.
Unlocking the Posterior Shoulder Joint Approach: Techniques & Indications
Introduction & Epidemiology
The posterior approach to the shoulder joint, while less frequently employed than its anterior counterparts, offers critical exposure to the posterior glenoid, humeral head, and surrounding structures. Its application is typically reserved for specific, often complex, pathological conditions that demand direct visualization and manipulation of these posterior aspects. Historically, open posterior approaches were a mainstay for addressing recurrent posterior instability, but advancements in arthroscopic techniques have refined the indications, largely limiting the open approach to scenarios requiring extensive bone work, tumor excision, or complex fracture management.
Epidemiologically, conditions necessitating a posterior open approach are uncommon. Posterior glenohumeral dislocations represent approximately 2-5% of all shoulder dislocations, with a significant proportion amenable to closed reduction or arthroscopic intervention. However, complex posterior fracture-dislocations, chronic locked dislocations, or cases with substantial glenoid bone loss often mandate an open posterior approach for optimal reduction and fixation. Similarly, tumors or infections localized to the posterior scapula or glenoid are rare but demand direct access for biopsy, excision, or drainage. Understanding the nuanced indications and meticulous surgical technique for this approach is paramount for any orthopedic surgeon managing complex shoulder pathology.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is foundational to safely and effectively utilize the posterior approach. The key structures to navigate include bony landmarks, muscle layers, and critical neurovascular elements.
Bony Landmarks
The primary bony landmarks defining the posterior shoulder are the acromion , the spine of the scapula , the medial border of the scapula , and the coracoid process (palpable anteriorly but relevant to understanding glenoid orientation). The spine of the scapula extends obliquely from the medial border laterally to form the acromion, providing a crucial landmark for incision and deltoid detachment. The glenoid itself, a shallow piriform fossa, is key, with its posterior aspect being the target of many indications for this approach. The proximal humerus, specifically the humeral head, anatomical neck, and greater tuberosity, are also intimately involved, particularly in fracture-dislocation scenarios.
Muscular Layers
The posterior shoulder is covered by several muscle layers.
*
Superficial Layer:
The
deltoid muscle
forms the most superficial layer over the shoulder joint. Its posterior fibers originate from the spine of the scapula and acromion, converging to insert on the deltoid tuberosity of the humerus.
*
Deep Layer (Rotator Cuff):
Beneath the deltoid, the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) are encountered. For the posterior approach, the
infraspinatus
and
teres minor
are of primary importance. The infraspinatus originates from the infraspinous fossa and inserts onto the middle facet of the greater tuberosity. The teres minor originates from the lateral border of the scapula and inserts onto the inferior facet of the greater tuberosity. These two muscles contribute to external rotation and lie directly over the posterior capsule. The interval between the infraspinatus and teres minor can be a useful plane for capsular access, though a trans-tendinous split of the infraspinatus is more common for wider exposure.
Neurovascular Structures
Precise knowledge of neurovascular structures is critical to avoid iatrogenic injury.
*
Axillary Nerve:
This nerve, originating from the posterior cord of the brachial plexus (C5-C6), courses around the surgical neck of the humerus, deep to the deltoid. It lies approximately 5-7 cm distal to the acromion, making the distal extent of the deltoid split a potential risk zone. It innervates the deltoid and teres minor.
*
Posterior Circumflex Humeral Artery:
Accompanies the axillary nerve, supplying blood to the deltoid and humeral head.
*
Suprascapular Nerve:
Arises from the upper trunk of the brachial plexus (C5-C6), passes through the suprascapular notch, and then through the spinoglenoid notch to innervate the supraspinatus and infraspinatus muscles. It is typically deep and medial to the exposure but can be at risk during aggressive retraction or excessive glenoid screw placement.
*
Radial Nerve:
While not directly within the surgical field of the shoulder joint itself, its proximity distal to the humerus makes it a consideration during patient positioning and limb manipulation, especially in complex fracture cases.
The internervous plane for the posterior approach is typically between the posterior deltoid (innervated by the axillary nerve) and the infraspinatus (innervated by the suprascapular nerve). A controlled split of the posterior deltoid allows access to the infraspinatus and teres minor.
Indications & Contraindications
The posterior approach, though rarely required, provides unparalleled access to the posterior and inferior aspects of the glenohumeral joint. Its indications are highly specific, often involving complex bony pathology or extensive soft tissue deficits.
The posterior approach offers access to the posterior and inferior aspects of the shoulder joint. It rarely is needed, but can be used in the following instances:
- Glenoid osteotomy: For correction of glenoid retroversion, typically in cases of posterior instability or dysplasia.
- Biopsy and excision of tumors: Especially those located in the posterior glenoid, scapular neck, or infraspinous fossa.
- Drainage of sepsis: The approach allows for dependent drainage of posterior shoulder joint infections with the patient in a supine or semi-recumbent position, which can be advantageous in critically ill patients.
- Treatment of fractures of the scapula neck, particularly those in association with fractured clavicles (floating shoulder): When closed reduction is not possible or adequate stability for early motion cannot be achieved. The posterior approach allows direct visualization and stable internal fixation of the scapular body and neck.
- Treatment of posterior fracture dislocations of the proximal humerus: Particularly those with a significant impression fracture (reverse Hill-Sachs lesion, >25% articular involvement), chronic locked dislocations, or cases with associated glenoid fracture.
Other potential indications include:
* Open reduction and internal fixation of complex posterior glenoid fractures.
* Repair of chronic or extensive posterior labral tears and capsular deficiencies not amenable to arthroscopic repair, especially with associated bony pathology.
* Decompression of the suprascapular nerve at the spinoglenoid notch (though this is often done arthroscopically or through a smaller, more focused approach).
* Revision shoulder arthroplasty for posterior glenoid component issues.
Contraindications
Relative contraindications include:
* Active infection not amenable to primary drainage (absolute contraindication for elective procedures).
* Severe soft tissue compromise or extensive scarring from previous posterior surgery.
* Uncontrolled coagulopathy.
* Patient factors precluding safe anesthesia or prolonged positioning.
* Pathology amenable to less invasive or alternative approaches (e.g., arthroscopic repair of small posterior labral tears, closed reduction of acute posterior dislocations without significant bony injury).
Table: Indications for Posterior Open Approach vs. Alternative Management Strategies
| Indication for Posterior Open Approach | Alternative/Conservative Management Strategies |
|---|---|
| Complex posterior glenoid fractures (e.g., intra-articular, comminuted) | Non-operative (sling, physical therapy) for stable, non-displaced fractures; Arthroscopic fixation for select small fragments |
| Chronic locked posterior glenohumeral dislocation (>3 weeks) | Closed reduction (often unsuccessful or carries high complication rate in chronic cases) |
| Posterior fracture-dislocation of proximal humerus (>25% head impression) | Closed reduction with immobilization (for small impression fractures); Arthroscopic reduction and fixation |
| Extensive glenoid retroversion/dysplasia requiring osteotomy | Non-operative management (physical therapy) for mild cases; Arthroscopic labral repair/capsular shift for instability without bony correction |
| Biopsy/Excision of posterior scapular/glenoid tumors | Percutaneous biopsy for diagnosis; Anterior approach for tumors involving anterior glenoid/scapula |
| Deep posterior shoulder sepsis requiring dependent drainage | Arthroscopic debridement/lavage; Image-guided percutaneous drainage; Systemic antibiotics |
| Unstable scapular neck fractures (floating shoulder) requiring fixation | Non-operative (sling, physical therapy) for stable, minimally displaced fractures or those without associated clavicle fracture |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful execution of the posterior approach.
Pre-Operative Planning
-
Imaging Review:
- Plain Radiographs: AP, lateral (scapular Y), and axillary views are essential to assess bony architecture, fracture patterns, and glenohumeral congruity.
- Computed Tomography (CT): Crucial for evaluating complex bony pathology, such as glenoid fractures, posterior impression fractures of the humeral head (reverse Hill-Sachs), and quantification of glenoid retroversion or bone loss. Three-dimensional (3D) reconstructions from CT data are invaluable for surgical planning, especially for fracture reduction and plate contouring.
- Magnetic Resonance Imaging (MRI): Useful for assessing soft tissue injuries (e.g., rotator cuff tears, labral tears) and differentiating tumor types.
-
Surgical Strategy:
- Determine the exact pathology to be addressed.
- Plan the incision type and extent.
- Anticipate specific instrumentation (e.g., small fragment sets, specific plating systems for scapula/humerus, specialized retractors).
- Consider potential need for bone grafting in cases of significant bone loss.
- Discuss potential complications and contingency plans.
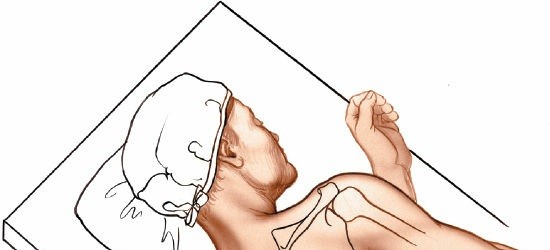
Patient Positioning
The choice of patient position depends on surgeon preference, the specific pathology, and the need for intraoperative imaging. The prone position or lateral decubitus position are the most commonly used.
-
Prone Position:
- Advantages: Provides excellent exposure to the entire posterior scapula and glenohumeral joint, allowing for easy access to the medial scapular border if needed. It facilitates dependent drainage in cases of infection.
-
Setup:
- The patient is positioned prone on a radiolucent operating table.
- Adequate padding is crucial to prevent pressure neuropathies, especially for the ulnar nerves, superficial peroneal nerves, and facial structures.
- The head is typically turned to the contralateral side and supported by a soft headrest, ensuring the ear is not folded.
- The ipsilateral arm is draped free to allow full range of motion, often placed on a padded arm board in slight abduction and internal rotation or allowed to hang free to provide traction.
- Ensure the chest is supported to allow for respiratory excursion, often with chest rolls or a special prone positioner.
-
C-arm access should be verified before draping.



Careful attention to the patient's ear and head position is necessary to prevent inadvertent folding or pressure injury.
-
Lateral Decubitus Position:
- Advantages: Allows for simultaneous anterior approach if needed, and easier access to the axilla. Some surgeons find this position more comfortable for longer cases.
-
Setup:
- The patient is positioned in a true lateral decubitus position with the affected side up.
- Adequate padding at all pressure points (axilla, contralateral arm, bony prominences).
- An axillary roll is placed to protect the neurovascular bundle of the dependent arm.
- The ipsilateral arm can be supported on an arm holder or suspended in traction, allowing for controlled manipulation and access.
Detailed Surgical Approach / Technique
The posterior approach typically begins with identifying key landmarks and creating a skin incision that allows for broad access while minimizing soft tissue disruption.
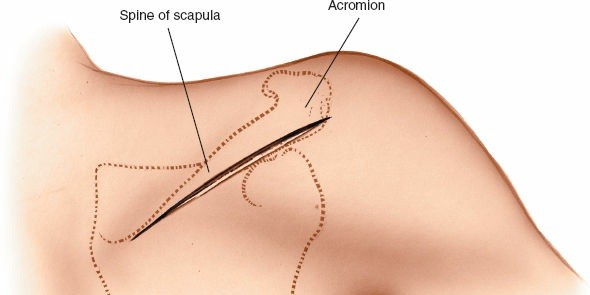
Landmarks and Incision
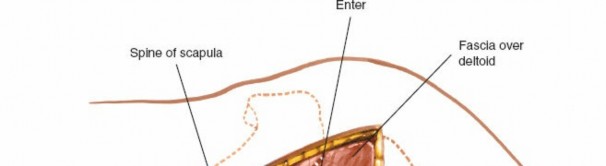
The acromion and the spine of the scapula form one continuous arch. The spine of the scapula extends obliquely from the medial border laterally to form the acromion.
1.
Palpation:
Identify the acromial angle, the spine of the scapula, and the medial border of the scapula. The posterior aspect of the glenohumeral joint lies roughly inferior to the posterior corner of the acromion.
2.
Incision:
* A common incision begins just medial to the posterolateral corner of the acromion, curves along the spine of the scapula, and then extends distally and slightly medially over the infraspinous fossa. The length depends on the required exposure.
* An alternative, more limited incision can be made directly vertical from the posterolateral acromion for access primarily to the joint capsule.
* For scapular body/neck fractures, a more extensive curvilinear incision may follow the medial border inferiorly.
After skin incision, dissection proceeds through subcutaneous tissue to identify the deep fascia.
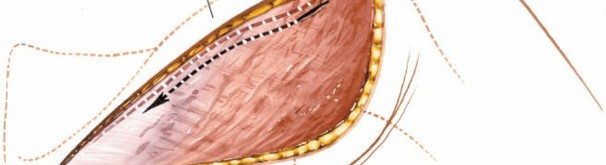
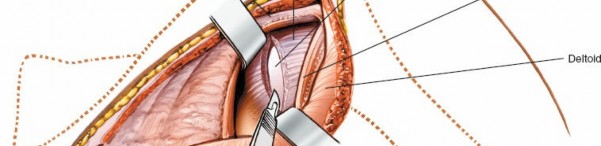
Superficial Dissection: Deltoid Split
- Fascia Incision: Incise the deep fascia along the planned path.
- Deltoid Identification: The posterior deltoid fibers are identified originating from the spine of the scapula.
-
Deltoid Detachment/Split:
- For maximal exposure, the posterior deltoid can be detached from the spine of the scapula and reflected laterally. Care must be taken to elevate it subperiosteally to preserve its origin.
-
Alternatively, a deltoid-splitting approach can be used. A split is made in the posterior deltoid fibers, typically along the line of the skin incision. The split should not extend more than 5-7 cm distally from the acromion to avoid injury to the axillary nerve and posterior circumflex humeral artery, which typically cross the humerus at this level.


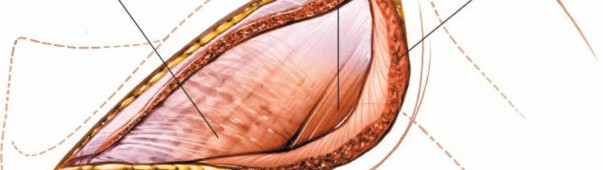
The deltoid is carefully retracted to expose the underlying rotator cuff.
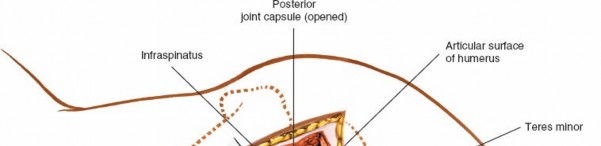
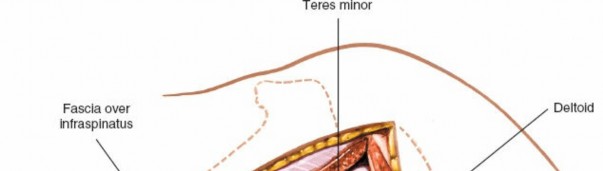
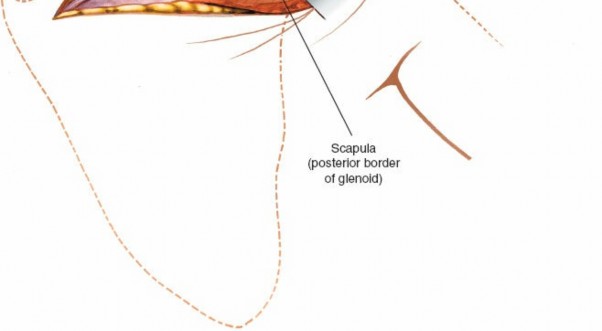
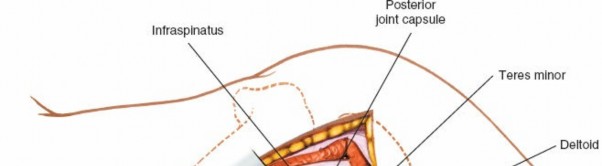
Deep Dissection: Rotator Cuff Exposure and Internervous Plane
-
Identification of Infraspinatus and Teres Minor:
Once the deltoid is retracted, the underlying infraspinatus and teres minor muscles are exposed. These muscles run obliquely from the scapula to the greater tuberosity of the humerus. The suprascapular nerve innervates the infraspinatus. The teres minor is innervated by a branch of the axillary nerve.


- Internervous Plane: The true internervous plane is between the teres minor (axillary nerve) and the infraspinatus (suprascapular nerve). A common approach involves splitting the infraspinatus muscle longitudinally in line with its fibers. This "trans-infraspinatus" approach provides excellent access to the posterior capsule and glenoid. The split should be central to minimize injury to the muscle belly.
-
Retraction:
The infraspinatus and teres minor are carefully retracted, typically superiorly and inferiorly, to expose the posterior glenohumeral capsule. Self-retaining retractors can be used, but care must be taken to avoid excessive pressure on the muscles and nerves.
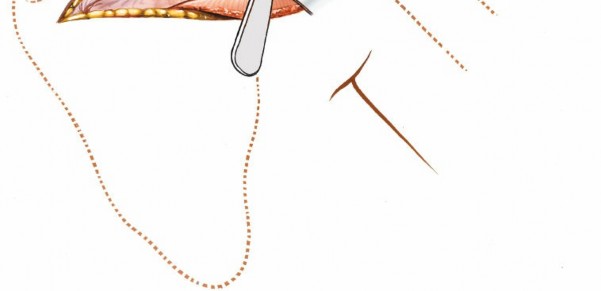

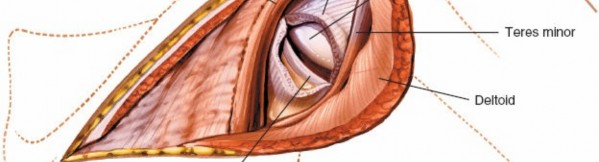
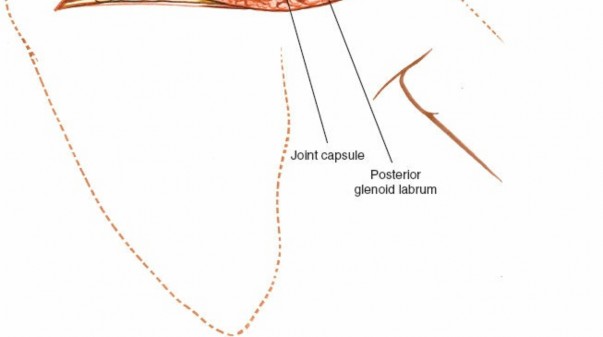
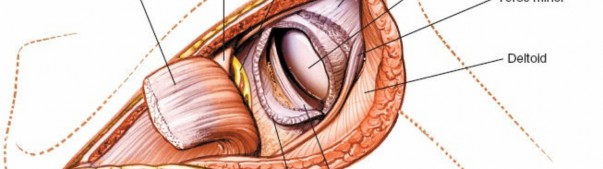
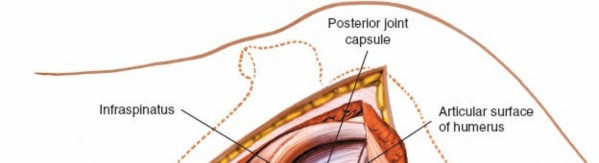
Joint Entry (Capsulotomy)
- Capsule Identification: The posterior glenohumeral joint capsule is visualized.
-
Capsulotomy:
A T-shaped or inverted T-shaped capsulotomy is commonly performed for wide joint access.
- A transverse incision is made along the attachment of the capsule to the glenoid or humerus.
- A vertical incision is then made, extending from the transverse cut superiorly and inferiorly, allowing reflection of capsular flaps.
-
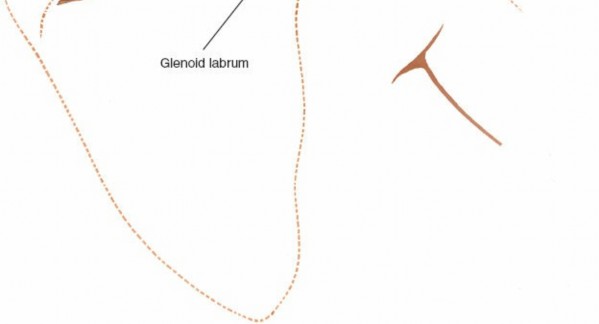
For specific posterior labral repair or stabilization, the capsule may be incised closer to the glenoid, potentially leaving a cuff of tissue for repair.

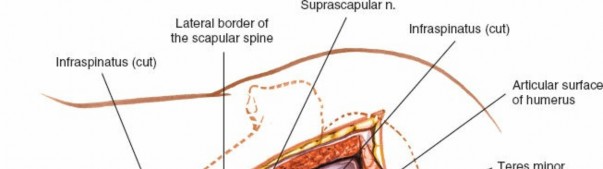
The glenohumeral joint is now exposed, allowing visualization of the humeral head and posterior glenoid.
Addressing Specific Pathology
Once the joint is exposed, specific procedures can be performed:
-
Posterior Fracture-Dislocation of the Humeral Head:
- Reduction: Gentle traction and external rotation are applied to the arm. If a locked dislocation, specific maneuvers may be needed to disengage the humeral head.
-
Management of Impression Fracture (Reverse Hill-Sachs):
- For small defects (<25%), direct reduction and stabilization may suffice.
- For larger defects (25-40%), a disimpaction osteotomy and bone grafting (autograft or allograft) may be required to restore the articular surface.
-
For very large defects (>40-50%) or severe comminution, hemiarthroplasty or total shoulder arthroplasty may be indicated, particularly in older patients.

- Fixation: Once reduced, stability is assessed. Internal fixation may involve screws, suture anchors, or in specific cases, specialized plates.
-
Glenoid Fractures / Osteotomy:
- Fracture Fixation: Direct reduction of fragments using clamps or K-wires, followed by plate and screw fixation. Contoured plates designed for the posterior scapula are often used.
- Osteotomy: Precise osteotomy of the glenoid can be performed to correct retroversion or address bone loss. Fixation with screws or small plates is then achieved.
-
Tumor Excision / Biopsy:
- Resection of bone or soft tissue tumors with appropriate margins. Biopsy material is sent for frozen section analysis as required.
-
Drainage of Sepsis:
- Thorough debridement of infected tissues, copious irrigation, and placement of drains.
Closure
- Capsule Repair: The capsulotomy is meticulously repaired with strong, non-absorbable sutures to restore stability.
- Rotator Cuff Repair: The split infraspinatus is repaired.
- Deltoid Repair: The deltoid origin is reattached to the spine of the scapula, or the split is closed. Careful repair of the deltoid is crucial for maintaining muscle function and preventing post-operative weakness.
- Layered Closure: Subcutaneous tissues and skin are closed in layers. A drain may be placed, especially in cases of fracture or infection.
Complications & Management
While the posterior approach offers excellent exposure, it carries potential risks. Awareness of these complications and strategies for their management is essential.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategy |
|---|---|---|
| Nerve Injury | ||
| Axillary Nerve | < 5% | Observation for neuropraxia (up to 12 months); EMG/NCS for diagnosis; Nerve exploration/grafting for persistent deficit |
| Suprascapular Nerve | < 2% | Observation; EMG/NCS; Nerve exploration/decompression if entrapped (rarely from posterior approach itself) |
| Vascular Injury | Rare | Direct repair; Ligation (for smaller vessels); Embolization |
| Infection | 1-5% | Debridement, irrigation, IV antibiotics; Hardware removal (if stable or nonunion present); Chronic suppressive antibiotics |
| Hematoma | 2-10% | Observation; Surgical evacuation if symptomatic or large; Drain placement |
| Stiffness / Loss of Motion | 10-20% | Aggressive physical therapy; Manipulation under anesthesia; Arthroscopic or open capsular release |
| Recurrent Instability | 5-15% | Revision surgery (arthroscopic or open) with soft tissue repair or bone grafting; Consider arthroplasty for severe cases |
| Nonunion / Malunion (Fracture) | 5-10% | Revision fixation with bone grafting; Corrective osteotomy; Arthroplasty (for proximal humerus) |
| Hardware Failure | 5-10% | Hardware removal; Revision fixation; Arthroplasty |
| Deltoid Dysfunction | 2-5% | Physical therapy; Deltoid repair if detached; Tendon transfer (rare) |
Detailed Complication Management
-
Nerve Injury:
- Axillary Nerve: Most commonly injured during distal extension of the deltoid split or vigorous retraction. Prevention involves careful identification of the nerve and limiting the distal split to 5-7 cm from the acromion. Post-operatively, if a deficit is noted, observation for up to 6-12 months is often warranted, as most are neuropraxias. Electrodiagnostic studies (EMG/NCS) can help assess the severity and prognosis. Surgical exploration and nerve grafting may be considered for persistent complete deficits.
- Suprascapular Nerve: Less commonly injured directly, but can be at risk during aggressive retraction in the spinoglenoid notch region or with misplaced superior glenoid screws.
-
Infection: Superficial wound infections are managed with antibiotics and local wound care. Deep joint infections often require surgical debridement, thorough irrigation, intravenous antibiotics, and potentially removal of hardware once stable or if nonunion develops.
-
Hematoma: Meticulous hemostasis during surgery is key. Post-operative drains can reduce hematoma formation. Large, symptomatic hematomas may require surgical evacuation.
-
Stiffness / Loss of Motion: A common sequela of any shoulder surgery. Aggressive, supervised physical therapy is paramount. If conservative measures fail, manipulation under anesthesia or arthroscopic/open capsular release may be necessary.
-
Recurrent Instability: Can occur if soft tissue repairs fail or if significant glenoid/humeral bone loss was not adequately addressed. Revision surgery, which may involve further soft tissue tightening or bone grafting, is often required.
-
Nonunion / Malunion: Specific to fracture cases. Nonunion may necessitate revision surgery with bone grafting and more robust fixation. Malunion might require corrective osteotomy or, in severe cases of proximal humerus malunion, arthroplasty.
-
Hardware Failure: Plates and screws can fail due to excessive stress, inadequate bone quality, or incomplete reduction. Management depends on the context but often involves hardware removal and revision fixation.
Post-Operative Rehabilitation Protocols
Rehabilitation following a posterior shoulder approach is tailored to the specific pathology addressed, the stability achieved intraoperatively, and the patient's general health status. The goals are to protect the repair, restore range of motion, regain strength, and optimize functional return. Most protocols follow a phased approach.
Phase I: Initial Protection (0-6 weeks)
- Goals: Protect surgical repair, minimize pain and swelling, promote soft tissue healing.
-
Immobilization:
- Typically, a shoulder immobilizer or sling is used continuously for 4-6 weeks, removing only for hygiene and specific exercises.
- For fracture-dislocations, the duration of immobilization might be longer (6-8 weeks), and specific positions (e.g., slight abduction, neutral rotation) may be prescribed to protect the reduction.
-
Exercises:
- Passive Range of Motion (PROM): Gentle, pain-free PROM (forward flexion, external rotation up to neutral, internal rotation to abdomen) initiated by a therapist. Avoid excessive internal rotation, adduction, and extension that could stress the posterior capsule.
- Elbow, Wrist, Hand ROM: Active range of motion exercises for the unaffected joints to prevent stiffness.
- Scapular Stabilization: Gentle isometric scapular squeezes (avoiding shoulder motion).
- Weight-Bearing: No weight-bearing or lifting with the affected arm.
Phase II: Controlled Motion (6-12 weeks)
- Goals: Gradually restore active range of motion, initiate light strengthening.
- Immobilization: Sling discontinued, or used for comfort as needed.
-
Exercises:
- Active-Assisted Range of Motion (AAROM): Progress from PROM to AAROM (patient assists movement with other hand or pulley system).
- Active Range of Motion (AROM): Gradually initiate pain-free AROM in all planes.
- Isometric Strengthening: Begin gentle isometric exercises for rotator cuff (internal/external rotation), deltoid, and scapular stabilizers.
- Proprioception: Gentle proprioceptive exercises.
- Weight-Bearing: Light activities of daily living (ADLs) are allowed within pain limits. Avoid lifting objects heavier than 1-2 lbs.
Phase III: Progressive Strengthening (12-24 weeks)
- Goals: Restore strength, endurance, and full functional range of motion.
-
Exercises:
- Progressive Resistive Exercises (PREs): Introduce light resistance bands and weights for rotator cuff strengthening (internal/external rotation, abduction, scaption), deltoid, and periscapular muscles.
- Advanced Scapular Stabilization: Focus on dynamic scapular control.
- Endurance Training: Low-resistance, high-repetition exercises.
- Return to Activity-Specific Drills: Begin sport-specific or occupation-specific exercises, gradually increasing intensity and complexity.
- Weight-Bearing: Progressively increase weight-bearing and lifting capabilities.
Phase IV: Return to Activity (24+ weeks)
- Goals: Optimize strength, power, and endurance for full return to sport or demanding work.
-
Exercises:
- High-Level Strengthening: Advanced PREs, plyometric exercises if appropriate.
- Functional Training: Simulate sport-specific movements (e.g., throwing, overhead activities) or work tasks.
- Maintenance Program: Long-term home exercise program to maintain gains.
- Return to Sport/Work: Gradual, progressive return based on functional assessment, strength testing, and physician approval.
Key Considerations:
- Individualization: Protocols must be individualized based on patient factors (age, activity level, bone quality), intraoperative findings, and healing response.
- Pain Management: Effective pain control is crucial for participation in therapy.
- Communication: Close communication between the surgeon, physical therapist, and patient is essential for optimal outcomes.
- Avoidance: For posterior instability cases, avoid combined internal rotation, adduction, and extension, which can reproduce posterior subluxation/dislocation.
Summary of Key Literature / Guidelines
The literature on open posterior shoulder approaches, while less extensive than for anterior approaches, highlights critical principles and evolving indications.
- Posterior Instability: Initial open posterior capsulorrhaphy techniques described by authors such as Boyd and Sisk (1971) demonstrated success in addressing recurrent posterior instability. However, modern arthroscopic techniques have largely superseded open stabilization for isolated soft tissue posterior instability. The open approach is now typically reserved for cases with significant bony deficiencies (e.g., glenoid retroversion, large posterior glenoid bone loss) or chronic, locked posterior dislocations.
- Posterior Fracture-Dislocations: Management of posterior fracture-dislocations of the proximal humerus remains a complex challenge. Hawkins et al. (1987) provided foundational classifications and treatment guidelines, emphasizing the importance of recognizing the impression fracture (reverse Hill-Sachs lesion) and guiding treatment based on its size and chronicity. Defects less than 25% of the humeral head articular surface are often amenable to soft tissue procedures or internal fixation alone, while those between 25-40% frequently require impaction osteotomy with bone grafting. Defects exceeding 40% may lead to higher rates of failure and often indicate consideration for hemiarthroplasty or total shoulder arthroplasty, particularly in older patients with poor bone quality.
- Scapular Fractures: While many scapular body and neck fractures are managed non-operatively, displaced intra-articular fractures, those affecting the glenoid neck resulting in significant glenoid displacement, or "floating shoulder" injuries (scapular neck fracture with concomitant clavicle fracture) may necessitate open reduction and internal fixation. Ada and Miller (1991) and subsequent works have refined the indications for operative intervention, often favoring a posterior approach for direct access to the scapular spine and glenoid neck. Biomechanical studies emphasize the need for stable fixation constructs, often involving plates along the lateral border or posterior aspect of the scapula.
- Tumor Excision and Drainage: For tumors or deep infections of the posterior glenohumeral joint or scapula, the posterior approach provides direct visualization and the ability to obtain adequate margins or achieve thorough debridement and dependent drainage, which is often crucial for infection resolution.
Current guidelines often advocate for a multidisciplinary approach in complex cases, utilizing advanced imaging (CT with 3D reconstruction) for precise pre-operative planning. The decision to employ an open posterior approach should be carefully weighed against less invasive options, considering the specific pathology, patient factors, and surgeon expertise. The judicious application of this approach, based on a deep understanding of anatomy and pathology, remains a critical skill in the armamentarium of the orthopedic shoulder surgeon.
Clinical & Radiographic Imaging