Pediatric Orthopaedic Case Study: Late-Presenting Infant DDH - Clinical & Diagnostic Insights
Key Takeaway
Late-presenting Developmental Dysplasia of the Hip (DDH) in infants often presents with a new limp, gluteal fold asymmetry, and a positive Galeazzi sign. A critical finding is marked restriction of passive hip abduction. Barlow and Ortolani maneuvers are typically negative, emphasizing thorough clinical examination and imaging for accurate diagnosis.
Orthopaedic Cases: Pediatric Orthopaedic Approach to Infant DDH
Patient Presentation & History
This case details the management of Developmental Dysplasia of the Hip (DDH) in an infant. DDH represents a spectrum of conditions ranging from hip instability to frank dislocation, characterized by an abnormal relationship between the femoral head and the acetabulum. The natural history, if untreated, often leads to progressive acetabular dysplasia, femoral head deformity, premature osteoarthritis, and significant functional impairment.
Our index patient, an 8-month-old female, presented to clinic with a new onset right-sided limp and asymmetry of her gluteal folds, noted by her parents. She was a first-born child, delivered vaginally at full term following an uncomplicated pregnancy, though a history of oligohydramnios was noted retrospectively. There was no recorded positive family history of DDH. Universal newborn hip screening, typically performed at birth by a pediatrician, did not identify any concerns. No formal risk-factor based ultrasound screening was performed at 4-6 weeks due to lack of local protocol adherence for her risk factors (first-born, oligohydramnios). She had achieved age-appropriate motor milestones for crawling and pulling to stand, with the limp becoming apparent shortly after she began cruising. She had no known comorbidities.
The significance of her late presentation at 8 months is critical. While newborn screening aims to identify unstable hips amenable to non-operative treatment, cases presenting later, beyond the optimal window for Pavlik harness use, often necessitate more invasive interventions. The presence of a limp (Trendelenburg gait or shortened limb) in a walking or cruising infant, or asymmetry of skin folds, are red flags for undiagnosed hip pathology, including DDH.
Clinical Examination
A thorough clinical examination was conducted with the infant cooperative but demonstrating clear signs consistent with DDH.
Inspection:
Upon initial observation, a notable asymmetry of the gluteal and thigh skin folds was apparent, with more numerous and deeper folds on the right side compared to the left. When the patient was placed in the supine position with hips and knees flexed, the right knee appeared lower than the left when comparing the femoral lengths (positive
Galeazzi sign
or Allis sign), indicating an apparent limb length discrepancy due to proximal migration of the dislocated femoral head. The right hip appeared to be held in a position of slight external rotation and adduction at rest.
Palpation:
Palpation around the hip joints revealed no overt tenderness, warmth, or swelling. Assessment of muscle tone was within normal limits, ruling out obvious neuromuscular causes. The greater trochanter on the right side felt more prominent and superiorly positioned relative to the iliac crest when compared to the left, a further indicator of hip dislocation.
Range of Motion (ROM):
Passive range of motion was assessed for both hips.
*
Abduction:
The most striking finding was a marked restriction of passive abduction in the right hip. While the left hip abducted freely to approximately 70-80 degrees, the right hip could only be abducted to about 30 degrees, often accompanied by soft tissue resistance and palpable tightness in the adductor musculature. This restricted abduction is a key sign in older infants where instability maneuvers may no longer be positive.
*
Adduction:
Full adduction was possible bilaterally.
*
Flexion:
Full flexion to 120-130 degrees was present bilaterally, though the right hip exhibited a slight increase in "piston" movement (telescoping), suggesting instability.
*
Rotation:
Internal and external rotation were assessed with the hip flexed to 90 degrees. No gross abnormalities were noted in rotational profiles, although the right hip felt less stable throughout the range.
Instability Maneuvers:
Given the patient's age (8 months), the classic Barlow and Ortolani maneuvers, which are highly sensitive in the newborn period, were performed but with expected limited utility.
*
Barlow Maneuver:
Attempted to elicit posterior dislocation by adducting and applying posterior pressure to the flexed hip. No definitive 'clunk' of dislocation was elicited, likely due to established contractures and scarring.
*
Ortolani Maneuver:
Attempted to reduce a dislocated hip by abducting and applying anterior pressure. No 'clunk' of reduction was felt, confirming the hip was irreducible by gentle manipulation.
Neurological/Vascular Assessment:
A comprehensive neurological examination of the lower extremities revealed no focal deficits, symmetrical deep tendon reflexes, and normal sensation to light touch. Peripheral pulses (femoral, dorsalis pedis, posterior tibial) were symmetrical and strong bilaterally, indicating intact vascular supply. These assessments are crucial to rule out underlying neurological conditions that can cause hip instability or to identify any iatrogenic compromise post-intervention.
In summary, the clinical examination strongly suggested a chronic, irreducible right hip dislocation with significant restricted abduction and a positive Galeazzi sign, consistent with the patient's age and presentation history.
Imaging & Diagnostics
Imaging studies are paramount for confirming the diagnosis, assessing the severity of DDH, identifying any impediments to reduction, and guiding treatment. The choice of imaging modality depends largely on the patient's age and the ossification status of the femoral head and acetabulum.
Ultrasound (US):
For infants up to 4-6 months of age, ultrasound remains the gold standard for diagnosing and monitoring DDH because the femoral head and acetabulum are predominantly cartilaginous, making them radiolucent on plain radiographs.
*
Graf Classification:
The primary method for static ultrasound evaluation involves the coronal view, assessing acetabular morphology and femoral head coverage.
*
Alpha angle:
Represents the bony acetabular roof angle (normal >60 degrees).
*
Beta angle:
Represents the cartilaginous acetabular roof angle (normal <55 degrees).
* Given our patient's age of 8 months, the utility of Graf classification was limited as increasing ossification obscures adequate cartilaginous visualization. However, a preliminary ultrasound at presentation was performed to visualize soft tissue structures. It confirmed the femoral head was completely dislocated superiorly and posteriorly, with a significantly hypoplastic and shallow acetabulum. The labrum was noted to be inverted, and a hypertrophied pulvinar was suspected. Dynamic ultrasound confirmed irreducibility.
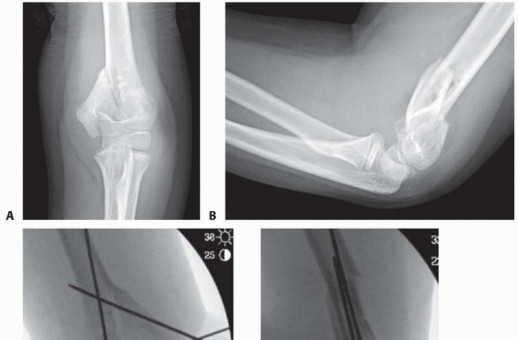
X-ray (Radiographs):
After 4-6 months of age, when the femoral head ossific nucleus typically appears, plain radiographs of the pelvis become the primary imaging modality.
*
Anteroposterior (AP) Pelvis with both hips in neutral position:
This is the standard view. Key radiographic lines and measurements include:
*
Hilgenreiner's line (Y-line):
A horizontal line connecting the bilateral triradiate cartilages.
*
Perkin's line:
A vertical line drawn perpendicular to Hilgenreiner's line, extending from the lateral aspect of the acetabular roof. The femoral head ossific nucleus should be in the inferomedial quadrant formed by these lines. In our patient, the right femoral head ossific nucleus was displaced superiorly and laterally, well outside the inferomedial quadrant.
*
Acetabular Index (AI):
The angle formed by Hilgenreiner's line and a line drawn from the medial aspect of the acetabular roof to its lateral aspect. Normal AI is typically <30 degrees at birth and decreases with age. In DDH, the AI is increased, indicating acetabular shallowness. Our patient's right AI measured 45 degrees, significantly elevated.
*
Shenton's line:
A continuous curvilinear line formed by the medial margin of the femoral neck and the superior margin of the obturator foramen. This line is typically interrupted in hip dislocation, which was evident on the right side of our patient.
*
Tear-drop distance:
The distance between the medial border of the femoral neck and the lateral margin of the true acetabular tear-drop. This distance is often asymmetrical in unilateral dislocation.
*
Femoral head ossific nucleus:
Its absence or small size can indicate delayed development, which is common in dislocated hips. On the right, the ossific nucleus was present but notably smaller and displaced compared to the left.
*
Frog-leg lateral view:
Provides additional information on femoral head coverage and anterior/posterior displacement. This view confirmed the posterior and superior dislocation.
Computed Tomography (CT) / Magnetic Resonance Imaging (MRI):
These advanced modalities are generally reserved for specific indications:
*
CT:
Primarily used for post-operative assessment of reduction and spica cast positioning, especially to confirm concentric reduction and detect subtle subluxation within the cast, as it provides excellent bony detail. It minimizes radiation by using limited cuts through the hips.
*
MRI:
The preferred modality for visualizing soft tissue impediments to reduction, such as an inverted labrum, hypertrophied pulvinar, constricted capsule, or an impinged iliopsoas tendon, prior to open reduction. It is also valuable for assessing the integrity of the femoral head's articular cartilage and for identifying early signs of avascular necrosis (AVN), although this is typically a follow-up concern.
* For our patient, given her age and irreducible dislocation requiring open reduction, a pre-operative MRI was obtained. This confirmed an extensively inverted cartilaginous labrum, a hypertrophied pulvinar filling the acetabular fossa, a taut and hourglass-shaped joint capsule, and an anteriorly displaced, hypertrophied iliopsoas tendon creating a block to reduction. These findings solidified the need for open surgical intervention.
Differential Diagnosis
When evaluating an infant with suspected DDH, it is crucial to consider a differential diagnosis, particularly given the potential for overlapping symptoms. Below is a detailed comparison of DDH with common alternative diagnoses.
| Feature | Developmental Dysplasia of the Hip (DDH)
You Might Also Like