Midshaft Clavicle Fractures: An Evidence-Based Guide to Diagnosis, Management, and Outcomes

Key Takeaway
Operative management for midshaft clavicle fractures is indicated for open fractures, neurovascular compromise, or severe skin compromise. Relative indications include significant displacement (>100%), shortening (>1.5-2cm), severe comminution, and nonunion, especially in high-demand patients, aiming to restore anatomical alignment and optimize functional outcomes.
Introduction & Epidemiology
Midshaft clavicle fractures are a common musculoskeletal injury, accounting for approximately 2.6% to 5% of all adult fractures and up to 44% of all shoulder girdle fractures. They typically result from a direct blow to the shoulder or a fall onto an outstretched arm. Historically, these fractures were predominantly managed non-operatively, with high union rates and satisfactory functional outcomes reported for many fracture patterns. However, advancements in surgical techniques and fixation hardware, coupled with a deeper understanding of fracture biomechanics and the functional implications of malunion, have led to an evolving paradigm in treatment.
The shift towards operative management for specific fracture patterns is driven by evidence suggesting improved functional outcomes, lower rates of symptomatic malunion, and reduced time to union in select patient populations. This comprehensive review aims to delineate the current understanding of midshaft clavicle fractures, providing an evidence-based framework for treatment selection, surgical technique, and post-operative management, targeting orthopedic surgeons, residents, and medical students.
Surgical Anatomy & Biomechanics
The clavicle is a unique S-shaped long bone, serving as the sole bony connection between the axial skeleton and the upper extremity. Its critical functions include maintaining the length of the shoulder girdle, protecting the underlying neurovascular structures (brachial plexus, subclavian artery and vein), and providing attachment points for several muscles vital for shoulder motion and stability.
Key Anatomical Features:
*
Shape:
The medial two-thirds are convex anteriorly, while the lateral one-third is concave anteriorly. The midshaft is the narrowest and weakest portion, making it most susceptible to fracture.
*
Muscle Attachments:
*
Superiorly:
Trapezius (lateral third), Sternocleidomastoid (medial third).
*
Inferiorly:
Subclavius (subclavian groove), Pectoralis major (medial half), Deltoid (lateral half).
*
Ligamentous Attachments:
*
Medially:
Sternoclavicular ligaments (anterior, posterior, interclavicular, costoclavicular).
*
Laterally:
Acromioclavicular ligaments (superior, inferior), Coracoclavicular ligaments (trapezoid and conoid) which are crucial for suspending the scapula.
*
Neurovascular Structures:
Immediately posterior and inferior to the clavicle lie the subclavian artery and vein, and the brachial plexus. These structures are at risk during severe displacement or iatrogenic injury during surgical fixation. The supraclavicular nerves (sensory branches of the cervical plexus) cross the clavicle superiorly and are vulnerable during surgical incision and dissection.
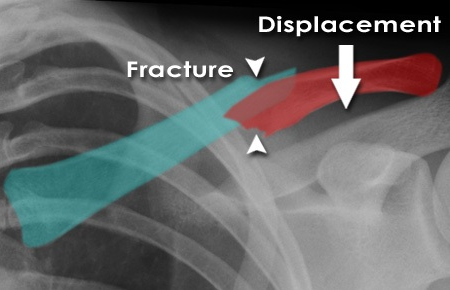
Biomechanics of Fracture:
Midshaft clavicle fractures typically result in characteristic displacement patterns due to muscle pull:
*
Medial fragment:
Often pulled superiorly by the sternocleidomastoid muscle.
*
Lateral fragment:
Often pulled inferiorly and medially by the deltoid muscle and the weight of the arm, and posteriorly by the pectoralis major.
*
Shortening:
Can occur significantly, particularly with comminution, due to the medializing forces. Shortening greater than 1.5-2 cm has been correlated with poorer functional outcomes in some studies.
The intramedullary canal is relatively small, making traditional intramedullary nailing less stable for many patterns compared to plate osteosynthesis. The cortical bone is relatively thin, requiring careful screw placement to achieve adequate purchase.
Indications & Contraindications
The decision-making process for midshaft clavicle fractures requires a careful assessment of fracture characteristics, patient factors, and functional demands. While many fractures still heal with non-operative management, specific indications for surgical intervention have become more defined.
Indications for Operative Management
The primary goal of operative fixation is to restore anatomical alignment, provide stable fixation, and facilitate early rehabilitation, ultimately aiming for superior functional outcomes and lower rates of symptomatic malunion or nonunion.
Absolute Indications:
*
Open fractures:
Require urgent debridement and stabilization to prevent infection.
*
Neurovascular compromise:
Acute or progressive neurological deficit (brachial plexus injury) or vascular compromise (subclavian artery/vein injury) due to fracture fragments.
*
Skin compromise / impending open fracture:
Severe tenting of the skin that risks perforation.
*
Polytrauma patient:
Where a stable clavicle fixation facilitates overall patient mobilization and rehabilitation.
*
Floating shoulder:
Ipsilateral clavicle and scapular neck/body fracture, though this is debated for midshaft fractures.
Relative Indications (Stronger Evidence for Operative Management):
*
Significant Displacement:
Complete displacement (>100% cortical apposition) or significant translation of fracture fragments.
*
Significant Shortening:
>1.5-2 cm shortening has been associated with poorer outcomes (e.g., Constant score). This is a critical factor, though precise thresholds remain debated.
*
Severe Comminution:
Particularly with a "Z-type" configuration or multiple fragments, which are inherently unstable.
*
Distal fragment instability:
Due to severe comminution or detachment of coracoclavicular ligaments.
*
Nonunion or symptomatic malunion:
After a trial of non-operative management.
*
Patient factors:
High-demand patients (e.g., athletes, manual laborers) who require early return to function and optimal shoulder mechanics.
*
Scapulothoracic dissociation:
Extremely rare but a devastating injury pattern requiring stabilization.
Indications: Operative vs. Non-Operative
| Feature / Indication | Non-Operative Management | Operative Management |
|---|---|---|
| Fracture Displacement | Minimally displaced (<100% cortical apposition, <5mm translation) | Complete displacement (>100% cortical apposition) |
| Fracture Shortening | <1.5 cm | >1.5-2 cm (consideration of patient height and body habitus) |
| Comminution | Simple, two-part transverse or short oblique fractures | Severe comminution, "Z-type" fractures, segmental fractures |
| Skin Integrity | Intact skin | Open fracture, impending open fracture (severe skin tenting) |
| Neurovascular Status | Intact neurovascular exam | Acute or progressive neurovascular compromise |
| Associated Injuries | Isolated clavicle fracture | Floating shoulder (ipsilateral scapular fracture), polytrauma |
| Patient Factors | Low demand, good compliance, minimal symptoms | High-demand patient, athlete, manual laborer, intolerable symptoms |
| Nonunion/Malunion | Not present | Symptomatic nonunion or malunion |
| Ipsilateral Upper Extremity | Intact | Scapulothoracic dissociation (rare) |
Contraindications for Operative Management
Absolute contraindications for any elective surgery apply, including:
*
Active infection:
Local or systemic.
*
Uncontrolled comorbidities:
Significant cardiac, pulmonary, or metabolic disease precluding safe anesthesia and surgery.
*
Severe osteopenia/osteoporosis:
May contraindicate plate fixation due to poor screw purchase, requiring alternative strategies or non-operative management if possible.
*
Unrealistic patient expectations.
Relative contraindications include:
* Poor surgical candidate status.
* Non-displaced or minimally displaced fractures that are expected to heal well non-operatively.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is paramount for successful outcomes and minimizing complications.
Pre-Operative Planning
-
Clinical Assessment:
- Detailed History: Mechanism of injury, hand dominance, occupation, activity level, prior shoulder issues.
-
Physical Examination:
- Neurovascular Status: Essential to document pre-operatively. Assess sensation (especially supraclavicular nerve distribution), motor function, and pulses. Palpate for subcutaneous hematoma or crepitus.
- Skin Integrity: Note any abrasions, lacerations, or severe tenting.
- Associated Injuries: Evaluate for ipsilateral shoulder, cervical spine, chest wall, or upper extremity injuries.
-
Imaging Studies:
- Standard Radiographs: True AP, 30-45 degree cephalic tilt (serendipity view), and orthogonal views (e.g., 30 degree caudal tilt view) are crucial for assessing displacement, shortening, and comminution.
- CT Scan: Highly recommended for complex comminuted fractures, severe shortening assessment, assessing intra-articular extension (less common in midshaft), or when planning revision surgery for nonunion. It provides detailed 3D anatomy.
- MRI: Rarely indicated acutely unless concomitant soft tissue injury (e.g., rotator cuff tear) or brachial plexus injury is suspected.
-
Templating and Hardware Selection:
- Plate Type: Low-profile pre-contoured locking plates are generally preferred. Superior plating is biomechanically superior but carries a higher risk of hardware prominence. Antero-inferior plating may be considered to reduce prominence, but care must be taken to avoid violating the superior cortex with screws.
- Screw Type: Locking screws provide angular stability, important in osteopenic bone or comminuted fractures. Non-locking screws allow for compression. Bicortical screw purchase is ideal for maximum stability, but careful intraoperative assessment of length is critical to avoid neurovascular injury.
- Length of Plate: Aim for at least 6 cortices of purchase on each side of the fracture.
- Informed Consent: Discuss surgical risks including infection, bleeding, neurovascular injury, nonunion, malunion, hardware prominence/irritation, need for future hardware removal, persistent pain, and refracture.
Patient Positioning
The choice between supine and beach chair position depends on surgeon preference, anesthetic considerations, and the fracture pattern.
-
Beach Chair Position:
- Advantages: Allows for easy access to the superior and anterior aspects of the clavicle. Facilitates examination of the shoulder and arm for reduction maneuvers. Less risk of venous congestion compared to flat supine.
- Disadvantages: Requires careful positioning to avoid brachial plexus stretch.
- Setup: Patient is placed in a semi-recumbent position with the torso elevated 30-45 degrees. The head is stabilized and turned slightly away from the operative side. Both arms are draped free, allowing for intraoperative manipulation to aid reduction and assess range of motion. A bump may be placed under the ipsilateral scapula to protract the shoulder.
-
(This image could illustrate a patient in beach chair position, or a shoulder drape.)
-
Supine Position:
- Advantages: Simpler positioning, less risk of hypotension with anesthesia.
- Disadvantages: May be slightly more challenging for shoulder manipulation.
- Setup: Patient is flat on the operating table. A small bump can be placed under the ipsilateral scapula to bring the clavicle anteriorly. The head is turned away, and the arm is draped free.
General Setup:
*
Sterile Prep and Drape:
Standard shoulder and arm prep. Ensure adequate exposure from the sternum to the acromion and inferiorly to the deltopectoral groove.
*
Fluoroscopy:
C-arm fluoroscopy should be positioned to allow for AP and cephalic/caudal tilt views without disrupting the sterile field. This is essential for confirming reduction and hardware placement.
Detailed Surgical Approach / Technique
The goal is anatomical reduction and rigid internal fixation to allow early motion and minimize complications. The superior approach is most common.
1. Incision and Dissection
- Incision: A curvilinear or straight incision is made directly over the fracture site, following the Langer's lines of the skin to optimize cosmetic outcome. The length of the incision should allow for adequate exposure of the fracture fragments and enough intact clavicle for plate placement. Typically, this is 6-10 cm.
- Subcutaneous Dissection: Carefully incise the skin and subcutaneous tissue. Identify and protect the supraclavicular nerves, which typically cross the clavicle perpendicular to the incision line. These nerves provide sensation to the skin over the superior chest and shoulder. Attempt to identify and retract them to minimize risk of neuropraxia or transection, which can result in a bothersome area of numbness.
- Platysma Muscle: Incise the platysma muscle (if present in the area) in line with the skin incision.
- Periosteum: Incise the periosteum longitudinally along the superior aspect of the clavicle, taking care to minimize extensive periosteal stripping, which can compromise bone vascularity. Elevate the periosteum just enough to expose the fracture fragments.
2. Fracture Reduction
- Assessment: Once the fracture fragments are exposed, carefully assess the fracture pattern, degree of displacement, comminution, and any soft tissue interposition.
-
Reduction Maneuvers:
- Traction and Manipulation: Apply longitudinal traction to the arm, often combined with manipulation of the shoulder (e.g., upward pressure on the elbow, posterior pressure on the acromion) to restore length and alignment.
- Direct Reduction: Use bone clamps (e.g., Verbrugge, pointed reduction clamps, Lambotte clamps) to grasp and manipulate the main fragments. Gentle levering with a periosteal elevator can also assist.
- Comminuted Fractures: In highly comminuted fractures, the goal is restoration of overall length and alignment, even if exact anatomical reduction of every small fragment is not achievable. Bridge plating may be necessary.
- Temporary Fixation: Once reduced, temporary fixation can be achieved with K-wires inserted obliquely across the fracture site or using small pointed reduction clamps.
-
(This image could show an intraoperative view of the fracture exposure and preliminary reduction with clamps or K-wires.)
3. Plate Application and Fixation
- Plate Selection: Choose a pre-contoured locking compression plate (LCP) that matches the anatomy of the superior aspect of the clavicle. Low-profile plates are generally preferred to minimize hardware prominence.
- Plate Positioning: Position the plate centrally on the superior surface of the clavicle. Ensure sufficient length to achieve at least three bicortical screws (or 6 cortices) proximal and distal to the fracture site. Avoid placing the plate too anteriorly or posteriorly, which can increase risk of prominence or inadequate bone purchase.
-
Screw Insertion (General Principles):
- Initial Fixation: Start with a non-locking screw (or a locking screw if direct compression is not possible) in a well-fitting hole on one of the main fragments (often the longest fragment) to provisionally secure the plate. Ensure the plate is centered and the reduction is maintained.
- Lag Screw Principle: For oblique fractures or butterfly fragments, a lag screw can be inserted through the plate or separately (if possible) prior to plating to achieve interfragmentary compression.
- Locking Screws: Fill the remaining holes with locking screws. These provide angular stability, which is particularly beneficial in comminuted fractures or osteopenic bone, preventing loss of reduction even if bone purchase is suboptimal.
- Bicortical Purchase: Aim for bicortical screw purchase in all fragments. Carefully measure screw length to avoid penetration of the posterior cortex into the neurovascular structures. Use a depth gauge judiciously, ensuring it does not over-penetrate.
- Fluoroscopic Guidance: Use intraoperative fluoroscopy in multiple planes (AP, cephalic/caudal tilt) to confirm plate position, fracture reduction, and appropriate screw length, especially for posterior screws.
-
(This image could show an intraoperative view of the plate being applied, with screws being inserted.)
4. Wound Closure
- Irrigation: Copiously irrigate the wound with sterile saline.
- Hemostasis: Ensure meticulous hemostasis.
- Periosteum: Close the periosteum carefully if possible, but avoid excessive tension.
- Platysma: Reapproximate the platysma muscle (if incised) with absorbable sutures.
- Subcutaneous Tissue: Close the subcutaneous layers to obliterate dead space and reduce skin tension.
- Skin: Close the skin with appropriate sutures or staples.
- Dressings: Apply sterile dressings.
-
(This image could show a post-operative radiograph of a well-fixed clavicle fracture.)
Complications & Management
Despite advancements in surgical techniques, midshaft clavicle fracture fixation is not without potential complications. Recognizing these and implementing appropriate management strategies is crucial for optimizing patient outcomes.
Common Complications and Management
| Complication | Incidence | Description & Management Strategy |
|---|---|---|
| Nonunion | 0-10% (operative); 5-15% (non-operative) |
Failure of fracture healing after 4-6 months, often symptomatic (pain, weakness, limited ROM).
Management: Revision surgery with debridement of nonunion site, rigid fixation (often with bone graft, autograft or allograft), and biologically active bone stimulation (e.g., PRP, BMPs). |
| Malunion | ~5% (symptomatic operative); ~30% (non-operative) |
Healing in an unacceptable position (e.g., significant shortening, angulation, rotation) leading to pain, cosmetic deformity, nerve irritation, or functional deficits (e.g., impingement, weakness).
Management: Mild asymptomatic malunion is observed. Symptomatic malunion requires corrective osteotomy, wedge resection, and stable internal fixation. |
| Hardware Prominence/Irritation | 10-30% |
Common due to superficial location of the clavicle. Can cause discomfort, skin irritation, or pain during activities.
Management: Typically managed with elective hardware removal after fracture union (usually 12-18 months post-op) if symptomatic. |
| Infection | 1-5% |
Superficial or deep. Presents with pain, erythema, swelling, warmth, purulent drainage, systemic signs.
Management: Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, thorough irrigation, intravenous antibiotics, potential hardware removal in chronic cases, negative pressure wound therapy. |
| Neurovascular Injury | <1% (iatrogenic) |
Damage to subclavian artery/vein or brachial plexus from fracture fragments or during surgery (e.g., excessive screw length, aggressive dissection).
Management: Immediate vascular/neurosurgical consultation. May require urgent exploration, repair, or reconstruction. Careful pre-op planning and intra-op fluoroscopy are preventive. |
| Supraclavicular Nerve Injury | 10-40% (neuropraxia/dysesthesia) |
Most common nerve complication. Can result in numbness, paresthesias, or hyperesthesia in the dermatome.
Management: Usually resolves spontaneously. Symptomatic cases may benefit from nerve block, gabapentinoids. Rarely requires surgical neurolysis. Meticulous dissection and protection during surgery are key. |
| Refracture | 1-5% (after hardware removal) |
Fracture occurring after union, often following hardware removal.
Management: Revision surgery with repeat fixation, often with a longer plate and potentially bone graft. Patient counseling on post-hardware removal activity restrictions is important. |
| Pneumothorax | Rare |
Iatrogenic injury to the pleura, especially with long screw placement inferiorly or aggressive dissection.
Management: Chest tube insertion. Requires high index of suspicion during surgery, especially with drilling near the inferior border. |
Strategies for Minimizing Complications
- Meticulous Surgical Technique: Gentle tissue handling, minimal periosteal stripping, precise reduction.
- Neurovascular Protection: Careful identification and retraction of supraclavicular nerves. Careful measurement of screw lengths with fluoroscopic confirmation to prevent posterior cortical penetration.
- Appropriate Hardware Selection: Use low-profile, pre-contoured plates to minimize prominence.
- Sterile Field: Strict adherence to sterile technique to minimize infection risk.
- Post-operative Rehabilitation: Adherence to a structured rehabilitation protocol to prevent stiffness and facilitate healing.
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is essential after operative fixation of midshaft clavicle fractures to optimize functional recovery and ensure stable fracture healing. The protocol should be tailored to the individual patient, fracture stability, and fixation strength.
Phase 1: Immediate Post-operative (Weeks 0-4/6)
Goals:
Pain control, protect healing fracture, minimize stiffness, promote soft tissue healing.
*
Immobilization:
Arm sling for comfort and protection. Sling can be removed for hygiene and exercises.
*
Range of Motion (ROM):
*
Elbow, Wrist, Hand:
Active ROM exercises several times daily.
*
Shoulder:
Pendulum exercises initiated early. Passive or active-assisted shoulder flexion (up to 90 degrees) and external rotation (to neutral) within pain tolerance. Avoid shoulder abduction beyond 90 degrees and internal rotation across the body to prevent stress on the healing fracture.
*
Activities of Daily Living (ADLs):
Encourage gentle use of the hand and forearm for light ADLs below shoulder height. Avoid lifting, pushing, or pulling with the affected arm.
*
Precautions:
No lifting objects >1-2 lbs. No excessive shoulder abduction or external rotation. Avoid direct pressure on the clavicle.
Phase 2: Early Mobilization (Weeks 4/6 - 12)
Goals:
Restore full pain-free ROM, initiate gentle strengthening.
*
Clinical and Radiographic Assessment:
Confirm early signs of fracture healing (e.g., callus formation) before progressing aggressively.
*
ROM:
Gradually increase passive and active-assisted ROM, working towards full pain-free range of motion. Begin active ROM as tolerated.
*
Strengthening:
*
Isometrics:
Gentle isometric exercises for the rotator cuff and deltoid, initiated gradually as pain allows.
*
Resistance:
Progress to light resistance exercises using elastic bands or very light weights for shoulder abduction, flexion, and internal/external rotation. Focus on proper scapular mechanics.
*
Activities:
Continue to avoid heavy lifting or high-impact activities. Begin light functional activities.
*
Precautions:
Continue to avoid direct impact or heavy loading on the clavicle.
Phase 3: Advanced Strengthening & Return to Activity (Weeks 12-24+)
Goals:
Maximize strength, power, endurance; facilitate return to sport/work.
*
Clinical and Radiographic Assessment:
Confirm solid union on radiographs.
*
Strengthening:
Progress to more advanced strengthening exercises including eccentric training, plyometrics (if appropriate for sport), and sport-specific drills. Focus on restoring full rotator cuff, deltoid, and periscapular muscle strength.
*
Endurance:
Incorporate cardiovascular and endurance training.
*
Return to Sport/Work:
*
Gradual Return:
A gradual, progressive return to full activity is recommended.
*
Contact Sports/Heavy Labor:
Typically delayed until 4-6 months post-operatively, after clinical and radiographic evidence of robust union and restoration of full strength.
*
Hardware Removal:
If symptomatic hardware is anticipated, it is usually removed after 12-18 months. Refracture risk following hardware removal should be discussed, and a brief period of activity modification or protection may be warranted.
*
Precautions:
Educate patients on potential risks of refracture and the importance of continued strengthening.
Throughout all phases, patient education, adherence to the protocol, and regular clinical follow-up are critical for successful rehabilitation. Physical therapy should be guided by the orthopedic surgeon and tailored to individual patient needs and progress.
Summary of Key Literature / Guidelines
The landscape of midshaft clavicle fracture management has evolved significantly over the past two decades, largely driven by pivotal clinical trials and meta-analyses comparing operative and non-operative strategies.
-
The Canadian Orthopaedic Trauma Society (COTS) Study (2007): This landmark prospective, randomized controlled trial compared plate fixation with non-operative treatment for displaced midshaft clavicle fractures. It found that operative fixation resulted in a significantly lower rate of malunion and nonunion, and improved functional outcome scores (Constant score) at 1-year follow-up. This study was instrumental in shifting the treatment paradigm, providing strong evidence for operative intervention in significantly displaced fractures.
-
Meta-analyses and Systematic Reviews: Numerous subsequent meta-analyses have largely supported the findings of the COTS study. They consistently demonstrate that surgical fixation (primarily plate osteosynthesis) of displaced midshaft clavicle fractures leads to:
- Lower nonunion rates: Surgical fixation consistently reduces the risk of nonunion compared to non-operative treatment, particularly for significantly displaced or comminuted fractures.
- Improved functional outcomes: While the absolute difference in functional scores may be small in some studies, statistically significant improvements in Constant, DASH, and other shoulder-specific scores are often observed in the operative groups.
- Higher complication rates (hardware-related): Operative treatment inherently carries risks such as infection, hardware prominence, and the need for subsequent hardware removal. However, these are often outweighed by the benefits of improved union rates and function.
-
Specific Fracture Characteristics:
- Shortening: The threshold for clinically significant shortening remains debated, but evidence suggests that >1.5-2 cm of shortening correlates with poorer functional outcomes with non-operative management. This metric, combined with displacement, is a strong driver for surgical consideration.
- Comminution: Severely comminuted fractures, especially those with a Z-type pattern, are inherently unstable and often benefit significantly from operative stabilization due to high rates of nonunion with conservative management.
- Fragment Displacement: Complete displacement (>100% cortical apposition) is a key indicator for surgical intervention, as it is highly correlated with nonunion.
-
Plate Fixation vs. Intramedullary Nailing: While intramedullary nailing (IMN) offers advantages such as smaller incisions and potentially less soft tissue dissection, plate osteosynthesis remains the gold standard for midshaft clavicle fractures due to:
- Superior rotational stability: Plates provide rigid multiplanar fixation, which is crucial for controlling rotational forces on the clavicle.
- Higher union rates: Studies have shown slightly higher union rates and lower reoperation rates with plate fixation compared to IMN for complex patterns.
- Broader applicability: Plates can accommodate a wider range of fracture patterns, including comminuted fractures and those requiring length restoration.
-
Hardware Prominence and Removal: Due to the subcutaneous location of the clavicle, hardware prominence is a common concern post-operatively. While often asymptomatic, approximately 10-30% of patients may require hardware removal due to irritation or pain. This should be discussed pre-operatively as a potential additional procedure.
Current Guidelines and Recommendations:
Based on the current body of evidence, the consensus in academic orthopedic surgery leans towards
operative fixation for significantly displaced (>100% cortical apposition) or severely shortened (>1.5-2 cm) midshaft clavicle fractures, especially in active, high-demand individuals.
Non-operative management remains appropriate for minimally displaced, stable fractures. The decision-making process must be individualized, considering patient factors, fracture characteristics, and the surgeon's expertise. Continued research is focused on refining indications, optimizing implant design, and enhancing rehabilitation protocols to further improve outcomes.
