Comprehensive Guide to Pediatric Upper Extremity Fractures: Assessment & Management
Key Takeaway
Pediatric upper extremity fractures require specialized assessment due to unique bone properties like open physes and remodeling potential. Key considerations include understanding age-related biomechanics, common patterns such as supracondylar humerus and distal radius fractures, and meticulous neurovascular evaluation. Management strategies prioritize optimal growth, function, and preventing long-term sequelae through appropriate non-operative or surgical intervention.
Introduction & Epidemiology
Pediatric fractures present unique challenges and considerations distinct from adult orthopedic trauma, primarily due to the presence of open physes, thicker periosteum, and significant remodeling potential. The title "Pediatric Fractures: When to Trust a Warm and Wellperfused Hand" encapsulates a critical diagnostic and decision-making dilemma, particularly pertinent to upper extremity injuries where neurovascular compromise can lead to devastating sequelae. This review will focus on the principles of assessment and management, with particular emphasis on scenarios demanding meticulous neurovascular evaluation.
Upper extremity fractures are among the most common injuries in children, accounting for approximately 40-50% of all pediatric fractures. The distal radius is the most frequently fractured bone in children, followed by the supracondylar humerus, forearm shaft, and phalanges. Mechanism of injury often involves falls onto an outstretched hand (FOOSH), leading to various fracture patterns including greenstick, torus (buckle), complete, and physeal injuries. Age-related differences in bone elasticity, periosteal thickness, and remodeling capacity significantly influence treatment strategies and acceptable reductions. A thorough understanding of pediatric anatomy, fracture patterns, and their implications for growth and function is paramount for optimal outcomes.
Surgical Anatomy & Biomechanics
Effective management of pediatric upper extremity fractures necessitates a precise understanding of the intricate regional anatomy and the unique biomechanical properties of growing bone.
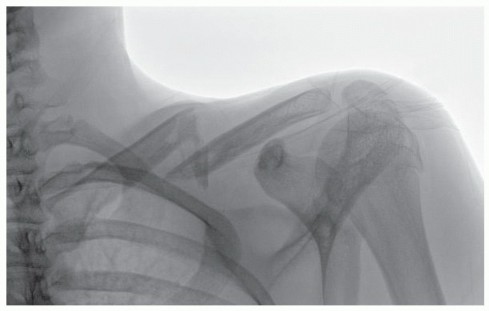
Distal Humerus (Supracondylar Region)
The distal humerus is a complex region, particularly susceptible to injury leading to neurovascular compromise.
*
Anatomy:
The supracondylar region narrows superior to the epicondyles, forming a relatively thin cortical cylinder. The anterior aspect is bordered by the brachial artery and the median nerve, running in close proximity to the bone. The radial nerve courses anterior to the lateral epicondyle and then bifurcates into superficial and deep branches. The ulnar nerve lies posteriorly in the cubital tunnel, vulnerable to entrapment or injury with medial column displacement or hyperflexion.
*
Biomechanics:
Supracondylar humerus fractures (SCHF) are typically extension-type injuries (95-98%), resulting from a FOOSH mechanism. The distal fragment is displaced posteriorly and proximally. This displacement can directly impinge upon or lacerate the anterior neurovascular bundle. The periosteum often remains intact on one side, contributing to fracture stability but also hindering reduction or serving as a tether.
Forearm (Radius & Ulna)
- Anatomy: The radius and ulna articulate proximally at the elbow and distally at the wrist, connected by the interosseous membrane. The radial artery lies volar to the distal radius, while the ulnar artery and nerve are located medially. The median nerve traverses the forearm proximally, deep to the flexor digitorum superficialis, emerging more superficially distally. The radial nerve's superficial branch is vulnerable dorsally at the distal forearm.
- Biomechanics: Pediatric forearm bones are prone to plastic deformation (bowing), greenstick, and complete fractures. The strong interosseous membrane dictates that isolated shaft fractures are rare, implying high-energy trauma if present. Remodeling potential is significant, especially in younger children, but rotational deformities remodel poorly.
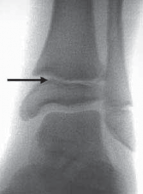
Distal Radius & Ulna
- Anatomy: The distal radial physis is the most active growth plate in the upper limb and is highly susceptible to injury. The median nerve passes through the carpal tunnel volar to the distal radius, and the radial artery passes volarly and radially.
- Biomechanics: Distal radius fractures are very common, typically from FOOSH. Patterns include buckle (torus) fractures (stable compression), greenstick fractures, and complete fractures, often with dorsal angulation and displacement. Physeal injuries (Salter-Harris types I and II predominantly) are also frequent. The thick periosteum often hinges dorsally, allowing for closed reduction but requiring careful assessment of stability. Remodeling is excellent for sagittal plane deformities, particularly in younger children.
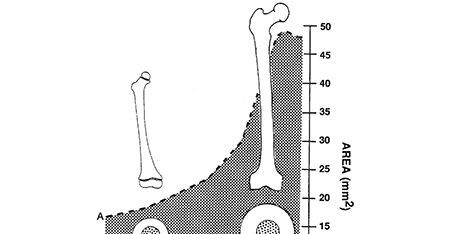
Physeal Considerations
- Growth Plate Structure: Physes are cartilaginous structures susceptible to shear, tensile, and compressive forces. The Salter-Harris classification system describes five primary types of physeal injury, with increasing risk of growth disturbance from type I to type V.
- Remodeling: Pediatric fractures possess remarkable remodeling potential, which decreases with age and distance from the physis. Rotational deformities remodel poorly, regardless of age. Angulatory deformities remodel best when in the plane of motion of the joint and closer to the physis.
Indications & Contraindications
Management of pediatric fractures spans a spectrum from simple immobilization to complex surgical intervention. The decision-making process is guided by fracture characteristics, patient age, associated injuries, and, critically, neurovascular status.
Non-Operative Indications
The majority of pediatric fractures are managed non-operatively. Key considerations include:
*
Minimally Displaced/Undisplaced Fractures:
Stable fractures with acceptable alignment for age and skeletal maturity.
*
Acceptable Angulation/Translation:
Pediatric bones, particularly in younger children, tolerate significant malalignment due to remodeling potential. Age-specific and fracture-specific guidelines exist (e.g., 20-30° angulation for distal radius in children <10 years, decreasing with age). Rotational deformities are poorly tolerated and are a relative indication for reduction.
*
Stable Fractures After Closed Reduction:
Fractures that are reduced manually and demonstrate stability in a functional cast or splint.
*
Greenstick & Torus Fractures:
These are inherently stable fracture patterns that typically heal well with immobilization.
*
Intact Neurovascular Status:
A warm, well-perfused hand with no neurological deficit, absent signs of impending compartment syndrome, and no severe displacement predisposing to secondary neurovascular compromise, favors non-operative management if other criteria are met.
Operative Indications
Surgical intervention is reserved for fractures that cannot be managed non-operatively or carry a high risk of complications with non-operative treatment.
*
Open Fractures:
All open fractures require surgical debridement and appropriate stabilization to prevent infection and promote healing.
*
Neurovascular Compromise:
*
Pulseless Pale Hand:
An absolute surgical emergency requiring immediate reduction. If perfusion does not return, arterial exploration and repair are mandatory.
*
Pulseless Pink Hand (Supracondylar Humerus):
Controversial. If good capillary refill and no neurological deficits, initial observation for a short period (1-2 hours) after reduction and stabilization may be considered by some, followed by urgent angiography if pulse does not return. However, persistent pulselessness or evolving neurological signs typically warrant urgent surgical exploration and possible vascular repair.
*
Acute Neurological Deficit:
New or worsening neurological deficit after reduction, or severe initial deficit, may warrant exploration.
*
Impending or Manifest Compartment Syndrome:
Requires immediate fasciotomy.
*
Irreducible Fractures:
Due to soft tissue interposition (e.g., periosteum, muscle, nerve) or gross instability after closed attempts.
*
Unstable Fractures After Closed Reduction:
Fractures that cannot be maintained in an acceptable position with casting.
*
Displacement Exceeding Acceptable Limits:
Persistent displacement or angulation beyond age- and fracture-specific thresholds.
*
Polytrauma:
Where fracture stabilization facilitates overall patient management and mobility.
*
Specific Physeal Injuries:
Salter-Harris type III and IV fractures, particularly intra-articular ones, require anatomical reduction to prevent growth arrest and articular incongruity.
*
Pathologic Fractures:
Fractures through pre-existing bone lesions may require stabilization and biopsy.
*
Floating Elbow/Knee:
Combined ipsilateral long bone fractures that compromise the stability of the limb.
Contraindications
Absolute contraindications to operative management are rare when surgery is indicated. Relative contraindications may include significant medical comorbidities precluding safe anesthesia, or minor, stable fractures where risks of surgery outweigh potential benefits.
TABLE: Operative vs. Non-Operative Indications for Pediatric Upper Extremity Fractures
| Indication Type | Non-Operative Management (Casting/Splinting) | Operative Management (Pinning/ORIF/ESIN) |
|---|---|---|
| Fracture Pattern | Torus/Buckle, Greenstick, Minimally displaced complete | Open fractures, Severely displaced complete, Unstable physeal fractures (SH III/IV articular) |
| Displacement | Undisplaced, Minimally displaced, Within age-specific acceptable limits | Grossly displaced beyond acceptable limits, Irreducible closed reduction |
| Angulation | Within age-specific acceptable limits (e.g., <20-30° distal radius <10yo) | Persistent angulation beyond acceptable limits, Rotational deformity >15-20° |
| Stability | Stable after reduction, Low risk of re-displacement | Unstable after reduction, High risk of re-displacement |
| Neurovascular | Warm, well-perfused hand with normal neurological exam, No signs of compartment syndrome | Pulseless pale hand , Pulseless pink hand (persistent/evolving) , Acute neurological deficit (new/worsening), Impending/Manifest compartment syndrome |
| Physeal Involvement | SH I (most), SH II (most) | SH III/IV (especially articular), SH V, Significant angular deformity from SH II |
| Associated Injuries | Isolated fracture without significant soft tissue injury | Polytrauma, Associated ligamentous injury requiring stabilization |
| Other | Compliant patient/family for cast care | Pathologic fractures, Failed non-operative management |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning is critical to ensure a safe and successful outcome in pediatric fracture surgery.
Clinical Evaluation
- History: Mechanism of injury, hand dominance, previous injuries, medical comorbidities, tetanus status.
-
Physical Examination:
- Neurovascular Assessment: This is paramount. Document capillary refill time, presence and quality of radial and ulnar pulses (palpable and/or Doppler), skin color, temperature, sensation (light touch, two-point discrimination in older children), and motor function of all major nerves (radial, median, ulnar). Compare to the contralateral limb. Document any pre-existing deficits. This is the cornerstone of "trusting a warm and wellperfused hand."
- Soft Tissue Assessment: Open wounds, skin tenting, ecchymosis, swelling. Assess for signs of impending compartment syndrome (pain out of proportion, pain with passive stretch, paresthesia, pallor, paralysis, pulselessness – the 6 Ps, though the latter two are late signs).
- Deformity: Angulation, rotation, shortening.
- Joint Integrity: Assess stability of joints proximal and distal to the fracture site if appropriate.
Imaging
- Plain Radiographs: Standard anteroposterior (AP) and lateral views are mandatory. Obtain true AP and lateral views, often requiring careful positioning. Include the joint above and below the fracture. Oblique views may be helpful for complex patterns (e.g., distal radius, humeral condyles).
- Stress Views: Rarely indicated but can assess ligamentous stability if suspicion for associated injury is high.
- Computed Tomography (CT): Reserved for complex intra-articular fractures (e.g., lateral condyle, capitellum), multi-fragmentary fractures, or when precise anatomical detail is needed for surgical planning. Not routinely used due to radiation exposure.
- Magnetic Resonance Imaging (MRI): Infrequently used in acute trauma; primarily for soft tissue injuries (e.g., ligamentous, meniscal, nerve entrapment), or avascular necrosis.
- Arteriography: Indicated for pulseless pale hands where reduction does not restore perfusion, or for pulseless pink hands where observation fails and vascular injury is suspected.
Anesthesia & Analgesia
- General Anesthesia (GA): Standard for pediatric orthopedic trauma.
- Regional Anesthesia: Adjunctive regional blocks (e.g., supraclavicular, infraclavicular, axillary brachial plexus blocks) can provide excellent post-operative analgesia, reducing GA requirements and systemic opioid use. Consider risks of masking early signs of compartment syndrome with prolonged blocks.
Surgical Setup & Equipment
- Team: Surgeon, surgical assistant, anesthesiologist, circulating nurse, scrub technician, radiology technician (for fluoroscopy).
- Radiolucent Operating Table: Essential for fluoroscopic imaging.
- C-arm Fluoroscopy: Crucial for real-time visualization of reduction and hardware placement. Ensure optimal image quality and radiation safety.
- Tourniquet: Applied to the proximal arm, inflated after limb elevation for exsanguination. Time should be carefully monitored.
- Pediatric Instrumentation: Appropriate size K-wires, drills, drivers, small clamps, retractors, and possibly small plating systems or ESINs.
- Microsurgical Tray: Should be immediately available if vascular or nerve exploration/repair is anticipated.
Patient Positioning
- Supracondylar Humerus Fractures: Supine position on a radiolucent table. The affected arm is positioned on a hand table or suspended, allowing full range of motion under fluoroscopy. The C-arm is positioned for easy AP and lateral views. The image intensifier is typically brought in from the side, allowing the surgeon to work around it.
- Forearm/Distal Radius Fractures: Supine position. The arm is draped free or positioned on a hand table, ensuring unimpeded fluoroscopic access.
- Sterile Prep & Drape: Wide prep to allow access to the entire upper extremity. Sterile tourniquet cover.
Prophylactic Antibiotics
- Administer intravenous antibiotics (e.g., Cefazolin) pre-operatively for open fractures, or for closed fractures undergoing internal fixation with significant hardware, typically 30-60 minutes before incision.
Informed Consent
Detailed discussion with parents/guardians regarding the nature of the injury, proposed treatment, alternative treatments, potential complications (including neurovascular injury, infection, malunion, nonunion, growth arrest, re-operation), and expected outcomes. Emphasis on the specific risks related to the fracture pattern (e.g., ulnar nerve injury with medial pinning of SCHF).
Detailed Surgical Approach / Technique
This section will detail the surgical management of two common pediatric upper extremity fractures with significant implications for neurovascular assessment: supracondylar humerus fractures and distal radius fractures.
Supracondylar Humerus Fracture (SCHF) - Gartland Type II, III, IV
Percutaneous pinning is the most common surgical technique for displaced SCHF. Open reduction is reserved for specific indications.
-
Patient Positioning and Preparation:
- Supine on a radiolucent operating table.
- Affected arm on a sterile hand table or suspended. Tourniquet applied proximally.
- Fluoroscopy C-arm positioned for unobstructed AP and lateral views.
- Thorough neurovascular reassessment immediately prior to draping.
-
Closed Reduction (Prerequisite for Percutaneous Pinning):
- Initial Traction: Gentle longitudinal traction in line with the humerus, typically in full elbow extension, to disengage fragments and restore length.
- Correction of Medial/Lateral Shift: Apply direct manual pressure to correct any varus/valgus or medial/lateral displacement while maintaining traction.
- Correction of Rotation: This is crucial. For posteromedial displacement, pronate the forearm. For posterolateral displacement, supinate the forearm. The common type III extension fracture with posteromedial displacement often requires pronation to disengage the radial column.
- Flexion: While maintaining traction and correcting rotation, the elbow is flexed to approximately 90-110 degrees, bringing the olecranon into the olecranon fossa. This maneuver helps reduce the distal fragment anteriorly.
- Fluoroscopic Confirmation: Confirm anatomical or near-anatomical reduction in both AP and lateral views. Assess Baumann's angle (normal 69-75° ± 6°) on AP view and anterior humeral line on lateral view (should intersect the capitellum).
- Post-Reduction Neurovascular Reassessment: Crucially, re-assess radial pulse and neurological function immediately after reduction. If the hand remains warm and well-perfused with a palpable pulse, proceed to pinning. If pulselessness persists, consider open reduction and vascular exploration.
-
Percutaneous Pinning (K-wires):
-
Lateral Entry (Two Crossed Lateral Pins):
This is the preferred method by many due to the lower risk of iatrogenic ulnar nerve injury compared to medial pins.
- Pin 1 (Lateral column): Insert a 1.6-2.0 mm K-wire into the lateral condyle, just proximal to the physis, aiming medially and proximally across the fracture site into the medial humeral cortex. Ensure good purchase in both cortices.
- Pin 2 (Medial column): Insert a second K-wire more anteriorly or posteriorly on the lateral condyle, aiming towards the medial column, crossing the first pin above the fracture. Ensure adequate spread of the pins at the fracture site for rotational stability.
- Fluoroscopic confirmation: Verify pin placement, fracture reduction, and stability in AP, lateral, and oblique views.
-
Medial and Lateral Crossed Pins:
Offers theoretically greater stability, but carries a higher risk of iatrogenic ulnar nerve injury.
- Ulnar Nerve Protection: The elbow must be fully extended to move the ulnar nerve posteriorly, away from the medial epicondyle. Alternatively, a small incision can be made to palpate and protect the ulnar nerve directly (mini-open technique).
- Medial Pin: Insert a K-wire through the medial epicondyle, aiming laterally and proximally into the lateral humeral cortex.
- Lateral Pin: Insert a K-wire as described above, ensuring it crosses the medial pin above the fracture.
-
Pin Configuration Considerations:
- Divergent pins: Provides good rotational stability.
- Pin Purchase: Aim for penetration of the opposite cortex for optimal stability.
- Avoid articular penetration.
- Check for fracture gapping/displacement during pinning.
- Pin Bending & Cutting: Bend pins 90 degrees and cut them flush with the skin, leaving a small exposed portion for removal. Dress pin sites.
-
Lateral Entry (Two Crossed Lateral Pins):
This is the preferred method by many due to the lower risk of iatrogenic ulnar nerve injury compared to medial pins.
-
Open Reduction (If Closed Reduction Fails or for Vascular Exploration):
- Anterior Approach (Henry's/Modified Henry's): Used for vascular exploration/repair and direct fracture reduction. Dissect between the brachioradialis and biceps/brachialis, exposing the brachial artery and median nerve. After vascular repair, reduce the fracture and fix with K-wires or small plates.
- Medial Approach: Incision over the medial epicondyle, protecting the ulnar nerve. Allows direct visualization and reduction of the medial column.
- Lateral Approach: Incision over the lateral epicondyle, dissecting between brachioradialis and triceps. Allows direct visualization of the lateral column.
- Internal Fixation: K-wires are standard. Small dynamic compression plates or pediatric locking plates may be used in select cases (e.g., older children, severe comminution).
Distal Radius Fracture
Most displaced distal radius fractures can be managed with closed reduction and casting, but surgical stabilization is indicated for unstable or irreducible fractures.
-
Patient Positioning and Preparation:
- Supine on a radiolucent table, arm on a hand table. Tourniquet.
- Fluoroscopy C-arm.
- Thorough neurovascular reassessment.
-
Closed Reduction (if indicated):
- Traction: Apply continuous longitudinal traction to overcome muscle spasm and disengage fragments.
- Exaggeration of Deformity: Gently exaggerate the dorsal angulation (if present) to unlock fragments.
- Reduction Maneuver: Apply volar pressure on the distal fragment while simultaneously applying dorsal pressure on the proximal fragment, combined with an opposite force to correct any rotational or translational deformities. Typically, a combination of traction, pronation/supination, and direct pressure.
- Confirmation: Fluoroscopic AP and lateral views. Assess length, angulation, and articular congruity. Acceptable angulation varies significantly with age.
- Neurovascular Reassessment.
-
Surgical Stabilization (for Unstable/Irreducible Fractures):
-
Percutaneous K-wire Fixation:
- Indications: Unstable fractures after reduction, large metaphyseal-diaphyseal angle, significant displacement in older children.
- Technique: After successful closed reduction, insert 1.6-2.0 mm K-wires from the radial styloid, aiming proximally across the fracture into the diaphyseal cortex. One or two pins are typically used, crossing proximal to the physis or obliquely through the metaphysis to avoid the physis if possible (extra-physeal pinning).
- Alternatively: Intrafocal pinning (Kapandji technique) involves inserting a K-wire through the fracture site to leverage and reduce the distal fragment, then driving it into the opposite cortex to stabilize.
- Fluoroscopic Guidance: Essential to confirm placement and stability. Avoid penetrating the articular surface or radial artery.
- Pin Management: Bend, cut, and dress pins.
-
Elastic Stable Intramedullary Nailing (ESIN/TEN):
- Indications: Unstable forearm shaft fractures, significantly displaced distal radius fractures, comminuted patterns, and in older children/adolescents.
- Technique: Typically two small-diameter, pre-bent titanium nails (one for radius, one for ulna) are inserted through small metaphyseal incisions (e.g., radial styloid for radius, distal ulna for ulna) and advanced across the fracture site. The nails gain stability by engaging the cortex on both sides of the fracture.
- Entry Points: For distal radius, radial styloid or Lister's tubercle. For ulna, distal ulna or olecranon.
- Nail Insertion: Advance nails under fluoroscopic guidance, ensuring sufficient length to cross the fracture and good cortical purchase. The elasticity provides stability.
-
Open Reduction Internal Fixation (ORIF):
- Indications: Very rare for isolated distal radius fractures; primarily for open fractures, highly comminuted articular fractures, or irreducibility with soft tissue interposition.
- Approach: Dorsal or volar approach depending on fracture pattern. Dorsal approach (e.g., between ECRL/ECRB and EDC) for dorsal displacement. Volar approach (e.g., through FCR sheath) for volar displacement.
- Fixation: Small pediatric plates and screws or K-wires.
-
Percutaneous K-wire Fixation:
Complications & Management
Complications following pediatric fracture management can range from minor to limb-threatening. Early recognition and appropriate intervention are crucial.
TABLE: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Clinical Presentation | Salvage Strategy / Management |
|---|---|---|---|
| Neurovascular Injury | |||
| Brachial Artery Injury (SCHF) | 1-5% (Pulseless Pink) to 0.5% (Pulseless Pale) | Pulseless Pale: No pulse, pale/cold hand, severe pain, loss of function. Pulseless Pink: No pulse, but good capillary refill, warm hand, normal color. | Pulseless Pale: Emergency! Immediate reduction. If no pulse return, urgent surgical exploration, fasciotomy, and vascular repair (e.g., saphenous vein graft). Pulseless Pink: Controversy. Most advocate immediate reduction and pinning. If no pulse after reduction, observe for 1-2h (some surgeons), then consider urgent exploration/angiography if persistent or signs of ischemia. |
| Nerve Injury (SCHF) | Median/Radial (5-10%), Ulnar (1-5% - often iatrogenic) | Sensory deficit, motor weakness/paralysis in affected nerve distribution. | Initial observation for neurapraxia (most common). If neurological deficit worsens post-reduction/pinning or fails to improve over 3-6 months, consider nerve exploration and neurolysis/repair. Iatrogenic ulnar nerve injury during medial pinning often requires immediate pin removal and nerve exploration. |
| Compartment Syndrome | Rare (0.1-0.7%), but critical (esp. forearm) | Pain out of proportion to injury, pain with passive stretch, paresthesia, tense compartments, weakness. (Pulselessness, pallor are late signs). | Emergency! Immediate four-compartment fasciotomy of the forearm. Delayed wound closure. Aggressive rehabilitation. |
| Malunion | Common (especially minor angulation/rotation) | Angulatory or rotational deformity after healing. | Most remodel, especially in younger children and for sagittal plane deformities. Rotational deformities remodel poorly. Surgical correction (osteotomy) for significant functional impairment, severe cosmetic deformity, or growth disturbance in older children/adolescents. |
| Nonunion | Rare (e.g., 0.1-0.2% in SCHF, higher in lateral condyle, scaphoid) | Persistent pain, motion at fracture site, radiographic lack of healing >3-6 months. | Risk Factors: Open fractures, highly unstable fractures, infection, specific fracture types (e.g., lateral condyle, distal physeal femur, scaphoid). Management involves open reduction, internal fixation, bone grafting (autograft/allograft), and addressing underlying causes. |
| Growth Arrest/Deformity | Varies by physeal injury type (SH I-V), 0-50% | Angular deformity, limb length discrepancy, joint incongruity. | Prevention: Anatomical reduction of SH III/IV. Management: Physeal bar resection (for partial arrest), epiphysiodesis (for complete arrest with significant remaining growth), corrective osteotomy (for angular deformity). |
| Infection | Open fractures (5-20%), Closed (0.1-1%) | Localized pain, swelling, erythema, warmth, purulent drainage, fever. | Superficial: Oral antibiotics, local wound care. Deep (Osteomyelitis): Surgical debridement, IV antibiotics (long course), hardware removal (if stable union or after union). |
| Stiffness/Loss of Motion | Common after elbow/intra-articular injuries (e.g., SCHF) | Restricted range of motion (flexion/extension, pronation/supination). | Early gentle active range of motion (AROM) after immobilization. Avoid aggressive passive stretching, which can exacerbate heterotopic ossification. Physical therapy, dynamic splinting. |
| Hardware Complications | Pin migration, breakage, irritation (1-5%) | Pain, skin irritation, prominent hardware, loss of reduction. | Symptomatic hardware removal after fracture healing. Revision fixation for loss of reduction. |
| Refracture | 1-5% (often after early cast removal) | New fracture at or near the original site. | Re-reduction and re-immobilization. Advise parents on activity restrictions until bone is fully consolidated. |
| Complex Regional Pain Syndrome (CRPS) | Rare (0.1-0.5%) | Disproportionate pain, allodynia, hyperalgesia, swelling, skin changes, stiffness. | Aggressive physical therapy, pain management (neuropathic agents, regional blocks), psychological support. Early recognition is key. |
Post-Operative Rehabilitation Protocols
Rehabilitation following pediatric fracture management aims to restore function, prevent stiffness, and facilitate a safe return to activities. Protocols must be tailored to the specific fracture, method of fixation, and patient age.
General Principles
- Immobilization: Maintain stability while healing. Duration depends on age, fracture type, and fixation method.
- Pain Control: Adequate analgesia to facilitate early motion and comfort.
- Early Motion (When Appropriate): Gentle active range of motion (AROM) is generally preferred over passive stretching to minimize risk of stiffness and heterotopic ossification, especially around the elbow.
- Gradual Progression: Slowly increase activity levels and resistance.
- Parent Education: Crucial for compliance with restrictions and recognizing warning signs.
Supracondylar Humerus Fracture (Pinned)
-
Immobilization (0-3 weeks):
- After pinning, a long arm cast or splint is applied, typically with the elbow flexed at 90 degrees and the forearm in neutral rotation (or pronation if medial pins were used to protect the ulnar nerve).
- Strict activity restriction. Close monitoring for neurovascular compromise and compartment syndrome.
-
Pin Removal & Early Motion (3-4 weeks):
- K-wires are typically removed in clinic after radiographic evidence of early callus formation (around 3-4 weeks).
- After pin removal, a posterior splint may be used for comfort, but active range of motion of the elbow and wrist is immediately encouraged.
- Crucial: Avoid forceful passive stretching or manipulation of the elbow joint, as this can increase the risk of heterotopic ossification and myositis ossificans. Gravity-assisted gentle flexion/extension exercises.
-
Strengthening & Return to Activity (4-8+ weeks):
- Gradual progression to strengthening exercises.
- Return to light activities (e.g., school sports without contact) around 6-8 weeks, with full return to contact sports typically not before 3 months, provided full range of motion and strength are recovered.
- Radiographic follow-up to confirm healing and monitor for malunion.
Distal Radius Fracture (Pinned/ESIN)
-
Immobilization (0-4 weeks for pins; 0-6+ weeks for ESIN):
- Short arm cast after pinning.
- For ESIN, immobilization duration varies; often a short arm cast for 4-6 weeks, with nails remaining for 3-6 months.
- Active range of motion of fingers and shoulder should be encouraged during immobilization.
-
Pin/ESIN Removal & Early Motion (4-6 weeks for pins; 3-6 months for ESIN):
- K-wires are typically removed at 4-6 weeks in clinic.
- After pin removal, active range of motion of the wrist and forearm is initiated.
- ESINs are typically removed after full radiographic healing and remodeling, often 3-6 months post-operatively, sometimes longer.
-
Strengthening & Return to Activity (6+ weeks):
- Gradual progression to strengthening exercises for grip and wrist motion.
- Return to non-contact sports typically 8-10 weeks post-injury; contact sports at 3-4 months, or when full strength and pain-free range of motion are achieved.
Post-Fasciotomy Rehabilitation
- Wound Care: Initial focus on wound management, dressing changes, and staged closure (often skin grafting).
- Early Motion: As soon as wounds are stable, aggressive physical therapy is initiated to prevent contractures and restore range of motion and strength. This is often a prolonged and intensive process.
Summary of Key Literature / Guidelines
Current practice in pediatric fracture management is largely guided by consensus from major orthopedic organizations, clinical experience, and evolving evidence. The central tenet remains the restoration of function with minimal morbidity, while accounting for growth potential.
Supracondylar Humerus Fractures
- Gartland Classification: Universally accepted for guiding treatment (Type I: undisplaced, Type II: displaced with intact posterior cortex, Type III: completely displaced, Type IV: multidirectionally unstable with intact periosteum allowing severe instability).
- Pinning Configuration: A 2017 meta-analysis published in JBJS supported lateral-entry bicortical pinning for Gartland Type II and III fractures, demonstrating similar stability to crossed pins with a lower risk of iatrogenic ulnar nerve injury. However, crossed medial and lateral pins may be biomechanically superior for highly unstable fractures (Type III/IV). Medial pinning should be performed with direct ulnar nerve visualization or elbow extension to minimize injury risk.
-
Pulseless Pink Hand Controversy:
There is no universal consensus on the management of a pulseless pink hand (with good perfusion) after reduction of a SCHF.
- The traditional approach was immediate vascular exploration.
- More recent literature, particularly from the 2000s onwards (e.g., studies by Campbell et al. in J Bone Joint Surg Am , 2009), suggests that if the hand remains warm and well-perfused with normal capillary refill and no neurological deficit after successful closed reduction and pinning, observation for pulse return may be appropriate, with exploration reserved for signs of ischemia or evolving neurological deficits. The key is strict observation.
- Pulseless Pale Hand: Remains an unequivocal surgical emergency requiring immediate exploration and vascular reconstruction if perfusion does not return after fracture reduction.
- Volkmann's Ischemic Contracture: While rare, it remains the most feared complication, emphasizing the critical importance of timely diagnosis and management of vascular compromise and compartment syndrome.
Distal Radius Fractures
- Acceptable Parameters: Guidelines vary by age and skeletal maturity. Younger children have greater remodeling potential. For distal radius, 20-25 degrees of dorsal angulation is often acceptable in children under 10, decreasing to 10-15 degrees in adolescents. Rotational deformity is poorly tolerated at any age. Shortening up to 1 cm can remodel.
- ESIN vs. K-wires: For unstable diaphyseal and metaphyseal forearm fractures, ESINs have gained popularity for their stability, ease of removal, and allowing earlier rehabilitation. For distal radius, K-wires remain a common and effective fixation method.
- Growth Plate Injuries: Salter-Harris classification remains the standard. Type I and II injuries generally have good prognoses, with Type III and IV requiring anatomical reduction to prevent articular incongruity and growth arrest.
General Guidelines
- Neurovascular Assessment: Repeated neurovascular checks are essential both pre- and post-reduction/fixation. Any change warrants immediate re-evaluation and potential intervention.
- Radiation Safety: Fluoroscopy should be used judiciously, adhering to ALARA (As Low As Reasonably Achievable) principles, especially in the pediatric population.
- Pain Management: Multimodal analgesia is encouraged to optimize comfort and facilitate rehabilitation.
- Role of Periosteum: The thick pediatric periosteum plays a crucial role in healing and can often act as a hinge, aiding in reduction but sometimes hindering it by interposition.
- Involvement of Societies: Guidelines from organizations such as the Pediatric Orthopaedic Society of North America (POSNA) and the American Academy of Orthopaedic Surgeons (AAOS) are invaluable resources for best practices in pediatric trauma.
In conclusion, managing pediatric upper extremity fractures requires a nuanced understanding of growth, biomechanics, and the inherent risks associated with specific injury patterns. While a "warm and well-perfused hand" is a reassuring sign, it must be considered within the broader clinical context, with a low threshold for investigation and intervention when other signs suggest impending compromise. Vigilance, meticulous assessment, and adherence to established surgical principles are paramount to preserving limb function and minimizing long-term disability in our young patients.
You Might Also Like