Anterior Tibial Osteotomy: Stable Fix for Osteochondral Lesions
Key Takeaway
This topic focuses on Anterior Tibial Osteotomy: Stable Fix for Osteochondral Lesions, Anterior trap door osteotomy is a stable surgical technique for treating osteochondral lesions of the talus (OLT). This osteotomy for osteochondral defects provides adequate exposure for cartilage grafting procedures, such as allograft or autograft reconstruction. It offers a stable alternative to traditional malleolar osteotomies, which can be unstable and require extended non-weight bearing.
Introduction and Epidemiology
Osteochondral lesions of the talus (OLT) represent a spectrum of pathologies affecting the articular cartilage and underlying subchondral bone of the talus. These lesions can cause significant pain, mechanical symptoms such as catching or locking, and functional impairment of the involved ankle joint, ultimately leading to degenerative changes if left untreated. The etiology of OLTs is multifactorial, commonly attributed to trauma (e.g., ankle sprains or fractures), osteonecrosis, or idiopathic causes. Epidemiological data suggests a prevalence ranging from 0.05% to 1.5% in the general population, with a higher incidence in younger, active individuals. While smaller, stable lesions may respond to non-operative management, larger, unstable, or symptomatic OLTs often necessitate surgical intervention.
A primary challenge in the surgical management of OLTs stems from the unique anatomy of the ankle joint. The talar articular surface is enclosed within the rigid osseous structures of the ankle mortise, formed by the distal tibia and fibula. This inherent anatomical constraint often limits direct visualization and access to central, posterior, or larger OLTs, particularly those requiring extensive debridement or cartilage grafting procedures. Historically, various approaches have been described to gain adequate exposure, including ankle arthroscopy, extended arthrotomies, and osteotomies of the malleoli.
Traditional malleolar osteotomies, specifically medial or lateral malleolar osteotomies, have been employed to provide comprehensive access to the talar dome. While effective in achieving exposure, these osteotomies are biomechanically less stable due to their cortical discontinuity and often involve disruption of the syndesmosis (in lateral malleolar osteotomy). Consequently, they typically necessitate an extended period of non-weight-bearing postoperatively to ensure adequate osseous healing and minimize the risk of complications. Nonunion rates for malleolar osteotomies, though variable, remain a concern and can lead to persistent pain, ankle instability, and potentially require revision surgery.
In response to the limitations of malleolar osteotomies, the anterior tibial "trap door" osteotomy was developed as a stable alternative. As described by Sammarco and Makwana, this technique allows for direct visualization and treatment of OLTs, often facilitating the harvesting and placement of autogenous talar autografts from non-weight-bearing portions of the talus. The anterior tibial osteotomy is designed to be intrinsically stable, offering a larger surface area for bone-to-bone contact and healing, thereby potentially allowing for earlier weight-bearing and reducing the risk of nonunion compared to malleolar approaches. Its fixation with absorbable pins further simplifies postoperative imaging and avoids issues associated with retained metallic hardware. This review aims to provide a comprehensive academic overview of the anterior tibial osteotomy, focusing on its indications, surgical technique, and clinical outcomes.
Surgical Anatomy and Biomechanics
A thorough understanding of the ankle's complex anatomy and biomechanics is paramount for safe and effective execution of the anterior tibial osteotomy. The ankle joint, a synovial hinge joint, is formed by the articulation of the distal tibia and fibula with the talus.
Bony Anatomy
The talus is unique in lacking muscular attachments and is almost entirely covered by articular cartilage. Its dome, the superior articulating surface, is wider anteriorly than posteriorly. OLTs can occur on any portion of the talar dome, but the anterior tibial osteotomy is particularly suited for lesions in the anterior two-thirds.
The distal tibia forms the roof and medial wall of the ankle mortise. The tibial plafond, its inferior articular surface, articulates directly with the talar dome. The anterior aspect of the distal tibia, where the osteotomy is performed, presents a relatively flat surface suitable for a stable bony cut.
The fibula forms the lateral malleolus, contributing to the lateral wall of the mortise. The integrity of the tibiofibular syndesmosis is crucial for ankle stability. Unlike malleolar osteotomies, the anterior tibial osteotomy preserves the syndesmosis.
Soft Tissue Structures and Neurovascular Anatomy
The anterior ankle is densely packed with crucial neurovascular and tendinous structures.
The deep peroneal nerve and the anterior tibial artery and veins run directly over the anterior aspect of the distal tibia, typically between the tibialis anterior and extensor hallucis longus tendons proximally, and superficial to the anterior ankle capsule distally. Meticulous dissection and careful retraction are imperative to prevent iatrogenic injury.
Tendons: From medial to lateral, the tendons of the tibialis anterior (TA), extensor hallucis longus (EHL), and extensor digitorum longus (EDL) cross the anterior ankle. These provide important landmarks and must be protected or retracted appropriately.
Ankle Biomechanics and Osteotomy Stability
The ankle mortise provides inherent stability, but its tight configuration limits surgical access. Direct visualization of large or central OLTs without an osteotomy is challenging, often necessitating extensive capsulotomies that can destabilize the joint or lead to prolonged swelling and stiffness.
Malleolar osteotomies, while providing access, disrupt critical stabilizers. A medial malleolar osteotomy severs the deltoid ligament attachments, while a lateral malleolar osteotomy, particularly if extending proximally, can violate the syndesmosis. Both approaches can lead to issues with stability, nonunion, and delayed rehabilitation.
The anterior tibial osteotomy offers a biomechanically superior alternative for several reasons:
1. Large Surface Area: The osteotomy creates a broad, rectangular or trapezoidal bone fragment from the anterior distal tibia. This large surface area for bony apposition promotes robust healing.
2. Intrinsic Stability: When properly designed as a "trap door" with a posterior hinge, the osteotomy fragment retains some inherent stability, reducing shear forces at the osteotomy site.
3. Preservation of Syndesmosis: Crucially, this osteotomy does not involve the syndesmosis or major ligamentous stabilizers of the ankle, preserving the mortise integrity.
4. Fixation: The use of absorbable pins or small screws allows for stable internal fixation without the need for removal and minimizes imaging artifacts. The inherent stability of the osteotomy design often allows for earlier weight-bearing compared to malleolar osteotomies. The larger bony surface area, protected neurovascular bundle, and preservation of joint stability are key biomechanical advantages.
Indications and Contraindications
The decision to proceed with an anterior tibial osteotomy for OLT is based on a comprehensive evaluation of the lesion characteristics, patient symptoms, and functional demands. The primary purpose of this osteotomy is to facilitate superior exposure for direct treatment of talar dome lesions that are otherwise inaccessible.
Indications
The anterior tibial osteotomy is indicated for exposure during surgical treatment of OLT, particularly for cartilage grafting procedures.
* Lesion Location and Size: Typically, this approach is necessary for OLTs located in the anterior two-thirds of the talar dome, irrespective of their medial, central, or lateral position. While anterior lesions might sometimes be accessible arthroscopically, larger anterior lesions (e.g., >1.5 cm²), or those with significant subchondral cysts, often require direct open access for adequate debridement, curettage, and precise graft placement.
* Depth and Morphology: Lesions classified as Berndt and Harty Stage III or IV, or Ferkel and Cheng Stage IV or V, often benefit from an open approach via osteotomy. This includes lesions with significant subchondral bone loss, cysts, or necrotic bone requiring extensive debridement and bone grafting.
* Surgical Strategy: When cartilage grafting procedures, such as osteochondral autograft transfer systems (OATS), mosaicplasty, or osteochondral allograft reconstruction (OCA), are planned, direct, unobstructed visualization is paramount for accurate graft sizing, harvesting, and secure press-fit insertion. The anterior tibial osteotomy provides an optimal panoramic view for such reconstructive efforts.
* Failed Prior Treatment: Patients with persistent symptoms despite prior arthroscopic debridement and microfracture may be candidates for this approach, particularly if residual lesions are large or deep.
* Recurrent Lesions: For recurrent OLTs, especially if previous attempts at treatment have failed due to inadequate access, the osteotomy provides a reliable alternative.
Contraindications
- Active Infection: Absolute contraindication due to high risk of osteomyelitis and systemic spread.
- Severe Ankle Arthritis: Patients with advanced, symptomatic tibiofibular or talonavicular arthritis may not benefit from OLT treatment alone. Ankle fusion or total ankle arthroplasty might be more appropriate.
- Poor Bone Quality: Severe osteoporosis or other metabolic bone diseases that compromise bone healing may contraindicate osteotomy and fixation.
- Critical Neurovascular Compromise: Pre-existing severe peripheral neuropathy or vascular insufficiency in the operative limb.
- Patient Non-Compliance: Patients unable or unwilling to adhere to postoperative weight-bearing restrictions and rehabilitation protocols.
- Lesion Location: Posterior talar dome lesions are generally better approached via posterior osteotomies (e.g., posterior malleolar osteotomy) or specialized posterior arthroscopic techniques.
- Small, Asymptomatic Lesions: Non-operative management is typically indicated for small, stable, and minimally symptomatic OLTs.
Operative vs. Non-Operative Indications
The decision pathway for OLT management can be summarized:
| Indication Type | Characteristics | Management Strategy |
|---|---|---|
| Non-Operative | Small lesion (<1.0-1.5 cm²), stable appearance on MRI/CT, minimal/intermittent symptoms, no mechanical symptoms, acute injury with minimal displacement, no subchondral cyst, failed previous non-operative treatment with persistent pain/mechanical symptoms. | Initial immobilization (boot/cast), activity modification, NSAIDs, physical therapy, corticosteroid injections (controversial for cartilage). Close monitoring with imaging. |
| Operative | Persistent pain and mechanical symptoms (locking, catching) despite 3-6 months of non-operative management, larger lesions (>1.0-1.5 cm²), unstable or displaced fragments, subchondral cysts, significant bone edema, chondral flap or loose body, location hindering natural healing, failed prior arthroscopy. | Arthroscopic: Debridement, microfracture (for small, contained lesions). Open (via Anterior Tibial Osteotomy): Cartilage grafting (OATS, OCA), extensive debridement, bone grafting for large/deep defects in the anterior 2/3 of the talar dome. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is crucial for optimizing surgical outcomes and minimizing complications associated with the anterior tibial osteotomy.
Preoperative Imaging
- Standard Radiographs: Anteroposterior, lateral, and mortise views of the ankle are essential to assess overall ankle alignment, identify associated bony pathologies (e.g., osteophytes, degenerative changes), and provide an initial assessment of the OLT if it has a bony component.
- Magnetic Resonance Imaging (MRI): Considered the gold standard for characterizing OLTs. MRI provides detailed information regarding lesion size (length, width, depth), location (medial, central, lateral, anterior-posterior), integrity of the overlying cartilage, presence of subchondral edema, bone marrow lesions, and cyst formation. This information is critical for determining the need for osteotomy and guiding the choice of cartilage repair technique.
- Computed Tomography (CT) Scan: Highly valuable for assessing the bony architecture of the talus and distal tibia, particularly for quantifying subchondral bone loss and delineating the precise margins of osteochondral defects. CT with 3D reconstruction aids in visualizing the extent of the lesion in relation to the ankle mortise and planning the optimal trajectory and dimensions of the anterior tibial osteotomy. It also helps identify any pre-existing hardware or bony spurs that might complicate the approach.
Lesion Localization and Osteotomy Planning
Precise localization of the OLT is paramount. Based on MRI and CT findings, the surgeon must determine the exact coordinates of the lesion on the talar dome. This guides the placement and dimensions of the anterior tibial osteotomy. The osteotomy can be tailored to be more medial, central, or lateral on the anterior tibia to optimize direct line-of-sight to the OLT. Consideration should be given to the length of the osteotomy fragment required to create adequate exposure without compromising stability or involving neurovascular structures.
Patient Counseling
While this is not "patient education" as per the rules, the surgeon must have a comprehensive understanding of the discussion required with the patient regarding the procedure. This includes outlining the nature of the OLT, the rationale for an anterior tibial osteotomy versus other approaches, potential benefits, risks (e.g., nerve injury, nonunion, infection, prolonged recovery), alternatives, and the expected postoperative rehabilitation course. Realistic expectations regarding pain management, weight-bearing restrictions, and return to activity must be set.
Operating Room Setup and Equipment
- Anesthesia: General anesthesia is typically employed, often supplemented with a regional ankle block for postoperative pain control.
- Tourniquet: A pneumatic thigh tourniquet is applied to provide a bloodless field, which is critical for precise dissection and visualization.
- Imaging: Fluoroscopy may be used to confirm the precise location of the lesion and to guide osteotomy placement if necessary, although careful preoperative planning often mitigates this need.
- Instrumentation: Standard orthopedic instrumentation, including a small oscillating saw with fine blades, small osteotomes, curettes, dental picks, retractors (e.g., Hohmann retractors, slender blunt retractors), bone hooks, and specialized instruments for cartilage grafting (e.g., OATS harvest kit, allograft preparation tools) are required. Fixation typically involves small, absorbable pins or cannulated screws (e.g., 2.7 mm or 3.5 mm).
Patient Positioning
The patient is positioned supine on the operating table under appropriate anesthesia, with thigh tourniquet control. A beanbag patient positioner is invaluable to facilitate positioning of the extremity.
* For medial lesions, the patient can be rolled slightly laterally toward the operative extremity. This allows for improved access to the medial aspect of the anterior tibia and subsequently the medial talar dome.
* For central and lateral lesions, the patient can be rolled slightly medially. This provides better exposure to the central or lateral anterior tibia.
The leg, ankle, and foot are then prepared and draped from below the knee, ensuring full access to the anterior ankle and adequate sterile field for potential graft harvesting sites if an autograft is planned.

Figure 1: Intraoperative setup with the patient positioned supine, leg prepared and draped, and thigh tourniquet applied. A leg holder or beanbag facilitates appropriate extremity positioning.
Detailed Surgical Approach and Technique
The anterior tibial osteotomy requires meticulous surgical technique to ensure adequate exposure, preserve neurovascular structures, and achieve stable osseous healing.
Incision and Dissection
- Skin Incision: A straight longitudinal incision approximately 6-8 cm in length is made over the anterior aspect of the distal tibia, centered over the planned osteotomy site. The incision extends from approximately 2 cm proximal to the ankle joint line to 4-5 cm distal. Careful attention is paid to avoid the superficial peroneal nerve branches, which cross subcutaneously.

Figure 2: Skin incision marked over the anterior distal tibia, centered on the planned osteotomy site, taking care to avoid neurovascular structures. - Subcutaneous Dissection: The incision is deepened through the subcutaneous tissues. Meticulous hemostasis is achieved. Superficial veins are ligated or coagulated.
- Identification of Neurovascular Structures: The deep peroneal nerve and anterior tibial artery/veins lie in the fascial plane between the tibialis anterior and extensor hallucis longus tendons. These structures are carefully identified and protected. They are typically retracted either medially or laterally, depending on the osteotomy's specific location, usually medially with the tibialis anterior muscle belly.

Figure 3: Dissection deepened to identify and protect the anterior neurovascular bundle (deep peroneal nerve and anterior tibial artery/veins), typically retracted medially with the tibialis anterior tendon. - Extensor Tendons and Capsule: The tendons of the tibialis anterior, extensor hallucis longus, and extensor digitorum longus are identified. The ankle joint capsule is then visualized. A longitudinal capsulotomy may be performed anteriorly, or the capsule may be elevated in continuity with the periosteum overlying the proposed osteotomy.
Osteotomy Planning and Execution
The anterior trap door osteotomy is characterized by a precisely cut bone block from the anterior distal tibia, hinged distally to avoid disruption of the anterior ankle joint capsule and allow for controlled elevation.
1. Periosteal Incision and Marking: The periosteum over the anterior distal tibia is incised longitudinally and reflected slightly to expose the bone. The precise dimensions of the osteotomy are marked on the cortex using a surgical pen. This is typically a rectangular or trapezoidal segment of bone, approximately 2-3 cm wide and 2.5-3.5 cm long. The distal hinge should be positioned superior to the anterior ankle capsule attachment to prevent disruption and facilitate stable elevation.

Figure 4: Periosteum incised and reflected, and the precise outline of the anterior tibial osteotomy is marked on the cortex, ensuring adequate dimensions for exposure.
2. Cortical Cuts: Using a fine oscillating saw with copious irrigation to prevent thermal necrosis, the proximal, medial, and lateral cortical cuts are made. These cuts should be precisely aligned and perpendicular to the bone surface. The distal cut is initially partial, serving as the hinge.

Figure 5: An oscillating saw is used to make the proximal, medial, and lateral cortical cuts for the osteotomy. Copious irrigation is critical to prevent thermal injury.
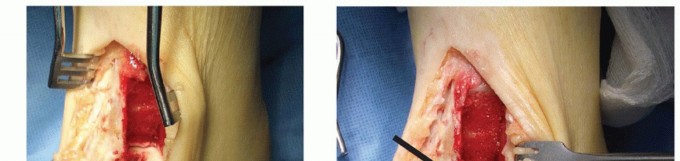
3. Completion of Osteotomy and Elevation: Small, thin osteotomes are then carefully introduced into the saw cuts. The osteotomy fragment is gently mobilized and "trapped-doored" open distally, hinging on its inferior cortex and periosteal attachments. This creates a stable opening, providing excellent direct visualization of the talar dome. The anterior neurovascular bundle and extensor tendons are carefully protected and retracted.

Figure 6: Thin osteotomes are carefully inserted into the saw cuts to complete the osteotomy, gently elevating the anterior tibial bone block distally, creating a "trap door" for access.

Figure 7: The anterior tibial osteotomy fragment is elevated on its distal hinge, providing direct, wide access to the talar dome and the underlying osteochondral lesion.
OLT Treatment
Once the osteotomy provides adequate exposure, the osteochondral lesion of the talus is addressed:
1. Lesion Debridement: The OLT is thoroughly debrided of any unstable cartilage, necrotic bone, and fibrous tissue. Subchondral cysts are curetted.
2. Cartilage Restoration: Depending on the lesion's characteristics and the surgeon's preference, various techniques can be employed:
* Microfracture: For smaller, contained lesions, creating microfractures in the subchondral bone to stimulate fibrocartilage formation.
* Osteochondral Autograft Transfer System (OATS): Harvesting healthy osteochondral plugs from a non-weight-bearing portion of the knee (e.g., femoral condyle) or the talus itself (as described by Sammarco and Makwana3 for autogenous talar autograft) and transplanting them into the prepared OLT defect.

Figure 8: After debridement of the OLT, the defect is prepared for cartilage grafting. A measuring guide is used to determine the appropriate size for osteochondral plugs.
* Osteochondral Allograft (OCA): Utilizing pre-sized allograft plugs for larger or more complex defects.

Figure 9: Osteochondral plugs are harvested (either autograft or allograft) and then press-fit securely into the prepared OLT defect, ensuring congruent articulation.
* Autologous Chondrocyte Implantation (ACI) / Matrix-Associated Autologous Chondrocyte Implantation (MACI): A two-stage procedure involving chondrocyte harvest, expansion, and subsequent implantation.
Reduction and Fixation of the Osteotomy
- Anatomical Reduction: After treating the OLT, the anterior tibial osteotomy fragment is carefully reduced back into its anatomical position. Proper alignment is crucial to restore the smooth contour of the anterior tibia and ensure optimal healing.

Figure 10: The anterior tibial osteotomy fragment is carefully reduced back into its anatomical position, ensuring proper alignment of the cortical edges. - Fixation: The osteotomy fragment is typically fixed with two to four absorbable pins (e.g., poly-L-lactide pins) or small, non-absorbable cortical or cannulated screws. Absorbable pins are favored as they do not interfere with postoperative imaging and eliminate the need for subsequent hardware removal. The fixation should provide stable compression across the osteotomy site.

Figure 11: The osteotomy fragment is secured with absorbable pins, providing stable internal fixation. This facilitates healing and avoids hardware-related issues. - Confirmation: The stability of the fixation is tested. Intraoperative fluoroscopy can be used to confirm proper reduction and placement of fixation.
Wound Closure
The surgical site is irrigated thoroughly. The periosteum is closed over the osteotomy if feasible. The capsule and extensor retinaculum are repaired. Subcutaneous layers are closed, followed by skin closure with sutures or staples. A sterile dressing and a posterior splint or controlled ankle motion (CAM) boot are applied for initial immobilization.
Complications and Management
While the anterior tibial osteotomy is designed to be a stable and reliable approach, like all surgical procedures, it is associated with potential complications. Surgeons must be aware of these risks and have strategies for their prevention and management.
General Surgical Complications
- Infection: Superficial or deep wound infection. Incidence is generally low (1-5%). Prevention involves strict aseptic technique, prophylactic antibiotics, and careful wound management. Management may require antibiotics, debridement, or formal irrigation and debridement with potential hardware removal in severe cases.
- Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE): Risk factors include prolonged immobilization and surgery duration. Prophylaxis (mechanical or chemical) is typically employed. Symptomatic DVT/PE requires anticoagulation.
- Neurovascular Injury: The deep peroneal nerve and anterior tibial artery/veins are at risk during dissection and retraction. Incidence of transient paresthesia is low but reported. Prevention relies on meticulous dissection, careful identification, and gentle retraction. Management of nerve injury depends on severity (observation for neuropraxia, direct repair for transection). Vascular injury requires immediate repair.
- Wound Healing Issues: Hematoma, seroma, skin edge necrosis, or dehiscence. Can be influenced by smoking, diabetes, and tension. Management includes wound care, aspiration, or debridement and resuturing.
Osteotomy-Specific Complications
- Nonunion or Delayed Union: Although less common than with malleolar osteotomies due to the larger bone contact area, nonunion can occur. Incidence is generally <5%. Predisposing factors include poor bone quality, inadequate fixation, or premature weight-bearing. Management involves extended immobilization, bone stimulators, or revision surgery with bone grafting and more rigid fixation.
- Malunion: Imperfect alignment of the osteotomy fragment, which can lead to prominence, altered biomechanics, or impingement. Prevention is achieved through precise reduction and stable fixation. Revision osteotomy may be required if symptomatic.
- Pain at the Osteotomy Site: Can be due to irritation from prominent hardware (if non-absorbable) or delayed healing. Absorbable pins mitigate hardware prominence.
- Fracture of the Osteotomy Fragment: Occurs during manipulation or fixation. Prevention involves careful technique, blunt osteotomes, and avoiding excessive force. Management depends on the fragment size and stability, often requiring additional fixation.
- Hardware-Related Issues: If non-absorbable hardware is used, irritation or impingement may necessitate removal. Absorbable pins largely eliminate this complication.
- Intra-articular Penetration: Fixation devices penetrating the joint can damage articular cartilage. Prevention requires careful measurement and fluoroscopic guidance.
OLT-Related Complications
- Graft Failure / Persistent Pain: Despite successful osteotomy, the cartilage graft itself may fail, or the underlying OLT may not heal, leading to persistent symptoms. This can be due to graft resorption, delamination, or incomplete defect fill. Incidence varies significantly based on graft type and patient factors. Management may include further diagnostic imaging and revision surgery (e.g., repeat grafting, microfracture, or salvage procedures like ankle arthrodesis).
- Ankle Stiffness / Arthrofibrosis: Prolonged immobilization or inadequate rehabilitation can lead to restricted ankle range of motion. Prevention involves early, controlled rehabilitation. Management may include aggressive physical therapy, manipulation under anesthesia, or arthroscopic lysis of adhesions.
- Progressive Arthritis: OLTs, even with successful treatment, can predispose to early onset or accelerated progression of ankle osteoarthritis. Long-term follow-up is essential.
Complications and Management Table
| Complication | Incidence (Approx.) | Salvage Strategies / Management |
|---|---|---|
| Nonunion / Delayed Union | <5% | Extended immobilization, bone stimulators, revision surgery with bone grafting and more rigid fixation (e.g., plate and screws). |
| Malunion | <2% | Observation for asymptomatic cases. Revision osteotomy for symptomatic malunion leading to impingement or functional impairment. |
| Pain at Osteotomy Site | 5-10% (transient) | NSAIDs, physical therapy. Hardware removal (if non-absorbable and prominent). |
| Deep Peroneal Nerve Injury | 1-3% (transient) | Observation for neuropraxia. Nerve conduction studies. Surgical exploration and neurolysis or repair for persistent deficit. |
| Wound Infection | 1-5% | Oral/IV antibiotics. Incision and drainage. Debridement. |
| Hematoma / Seroma | 2-5% | Aspiration, compression dressings. Surgical evacuation if large or symptomatic. |
| Graft Failure (OLT) | 10-30% | Further diagnostic imaging, revision cartilage repair, debridement, arthroscopic lysis of adhesions, salvage arthrodesis. |
| Ankle Stiffness / Arthrofibrosis | 5-15% | Intensive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic lysis of adhesions. |
| DVT / PE | <1% | Anticoagulation. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is critical for optimizing outcomes following anterior tibial osteotomy and OLT reconstruction. The stability of the anterior tibial osteotomy, particularly when fixed with absorbable pins, often allows for a more accelerated rehabilitation protocol compared to traditional malleolar osteotomies, which is one of its primary advantages. However, the specific protocol must also consider the OLT treatment (e.g., microfracture, autograft, allograft) as this often dictates the weight-bearing progression.
The rehabilitation protocol is typically divided into phases:
Phase 1: Protection and Early Motion (Weeks 0-6)
- Immobilization: The ankle is typically protected in a posterior splint or a controlled ankle motion (CAM) boot.
- Weight Bearing:
- Non-weight-bearing (NWB): For the initial 2-4 weeks, the patient remains strictly non-weight-bearing on the operative extremity. This allows initial soft tissue healing and osteotomy consolidation.
- Touch-down weight-bearing (TDWB) / Partial weight-bearing (PWB): Gradually progressed from 2-4 weeks to 6 weeks, often starting with 10-25% body weight, depending on the OLT treatment type and surgeon preference. The inherent stability of the osteotomy facilitates this earlier progression compared to malleolar osteotomies.
- Range of Motion (ROM): Gentle, passive and active-assisted range of motion exercises for the ankle (dorsiflexion, plantarflexion, inversion, eversion) are initiated cautiously, avoiding excessive stress on the osteotomy site or graft. Subtalar motion should also be addressed.
- Muscle Activation: Isometric exercises for ankle musculature (e.g., plantarflexors, dorsiflexors) are started early to maintain muscle tone and prevent atrophy without stressing the healing structures.
- Pain and Edema Management: Elevation, ice, and analgesics are used to control pain and swelling.
Phase 2: Progressive Weight-Bearing and Strengthening (Weeks 6-12)
- Weight Bearing: Progression to partial weight-bearing (25-50% body weight) in the CAM boot, advancing to full weight-bearing as tolerated by the end of this phase, provided radiographic evidence of osteotomy healing is present and OLT treatment allows. The boot can gradually be weaned, typically by week 8-10, transitioning to supportive shoes.
- Range of Motion: Active and passive ROM exercises are intensified, aiming for full pain-free motion. Manual therapy techniques may be employed by a physical therapist to address any stiffness or capsular restrictions.
- Strengthening: Progressive strengthening exercises for all ankle muscle groups are introduced using resistance bands, light weights, and bodyweight exercises (e.g., heel raises, toe raises).
- Proprioception and Balance: Balance exercises (e.g., single-leg stance, wobble board) are initiated to restore neuromuscular control and stability.
Phase 3: Advanced Strengthening and Return to Activity (Weeks 12+)
- Weight Bearing: Full weight-bearing without assistive devices or boot.
- Advanced Strengthening: Continue with progressive resistance exercises. Introduce sport-specific strengthening, plyometrics, and agility drills as appropriate for the patient's functional goals.
- Functional Training: Running progression, jumping activities, and sport-specific drills are gradually integrated, ensuring proper biomechanics and symptom-free performance.
- Return to Activity: Gradual return to light recreational activities is typically allowed around 4-6 months, with full return to competitive sports or high-impact activities often taking 6-12 months, depending on the extent of the OLT and its treatment. Clinical and radiographic healing of both the osteotomy and the OLT must be confirmed prior to full clearance.
Monitoring
Regular clinical follow-up and radiographic assessment are essential throughout rehabilitation to monitor osteotomy healing, evaluate graft integration, and adjust the protocol as needed. Any signs of delayed healing, increased pain, or mechanical symptoms warrant re-evaluation and potential modification of the rehabilitation plan.
Summary of Key Literature and Guidelines
The anterior tibial osteotomy, particularly the "trap door" technique, has gained recognition as a valuable approach for managing difficult-to-access osteochondral lesions of the talus. Its evolution stemmed from the recognized limitations and complications associated with traditional malleolar osteotomies.
The foundational work for this approach often references Sammarco and Makwana (2005), who described the "trap door" osteotomy to access OLTs, allowing for the harvest of autogenous talar autografts from non-weight-bearing regions. Their work highlighted the stability of this approach and its suitability for cartilage grafting procedures. This seminal contribution underscored the biomechanical advantages of preserving the ankle mortise and syndesmosis, distinguishing it from malleolar approaches.
Subsequent literature has further explored the efficacy and outcomes of the anterior tibial osteotomy. Studies comparing various osteotomy techniques for OLT access often emphasize:
* Stability: Multiple biomechanical and clinical studies have reinforced the intrinsic stability of the anterior tibial osteotomy. It offers a larger bone-to-bone contact area and typically uses robust fixation (e.g., absorbable pins or small screws), leading to lower rates of nonunion compared to malleolar osteotomies. This enhanced stability is a key factor enabling earlier, albeit controlled, weight-bearing postoperatively.
* Access: While medial and lateral malleolar osteotomies offer wider exposure, the anterior tibial osteotomy provides excellent, direct perpendicular access to the anterior two-thirds of the talar dome, which is precisely where many larger, symptomatic OLTs are located. This direct line of sight is crucial for precise debridement, cyst curettage, and accurate placement of osteochondral grafts (autograft or allograft).
* Complication Profile: The anterior tibial osteotomy generally reports a favorable complication profile. While neurovascular injury (deep peroneal nerve, anterior tibial artery) remains a risk, careful surgical technique mitigates this. Rates of nonunion, while possible, are lower than reported for malleolar osteotomies. The use of absorbable fixation often eliminates the need for hardware removal, a common issue with traditional metallic fixation.
Current guidelines for OLT management generally advocate a stepped approach:
1. Conservative Management: Initial treatment for smaller, stable, and less symptomatic lesions (activity modification, immobilization, NSAIDs, physical therapy).
2. Arthroscopic Debridement and Microfracture: For failed conservative treatment or smaller, accessible lesions.
3. Open Techniques with Osteotomy: Reserved for larger, deeper, or more complex OLTs, especially those requiring osteochondral grafting or extensive debridement, and those that are inaccessible arthroscopically. The anterior tibial osteotomy is increasingly recognized as a preferred open approach for anterior and central talar dome lesions due to its superior stability and rehabilitation potential.
Literature reviews and meta-analyses on cartilage repair in the ankle, while not exclusively focused on osteotomies, often highlight the importance of adequate lesion access. The anterior tibial osteotomy facilitates the gold standard techniques for large OLTs, such as osteochondral allograft transplantation (OCA), which has shown promising long-term results for these challenging defects.
Future Directions: Research continues to focus on optimizing osteotomy techniques, refining fixation methods, and improving the long-term outcomes of cartilage repair for OLTs. Advances in biological adjuncts, scaffold-based repair, and patient-specific implant design may further enhance the efficacy of these procedures. The role of 3D printing and navigation in preoperative planning for precise osteotomy execution is also an evolving area. However, the anterior tibial osteotomy remains a robust and critical component of the armamentarium for the comprehensive surgical management of significant OLTs.
Clinical & Radiographic Imaging


You Might Also Like

