Comprehensive Management of Humeral Shaft Fractures: Operative and Nonoperative Strategies

Key Takeaway
Humeral shaft fractures account for approximately 3% of all fractures. While functional bracing remains the gold standard for nonoperative management, operative intervention is indicated for polytrauma, open fractures, and vascular injuries. Plate osteosynthesis is the preferred surgical method, offering high union rates and lower complication profiles compared to intramedullary nailing. This guide details the biomechanics, surgical approaches, and fixation techniques for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Fractures of the humeral shaft represent a significant portion of orthopedic trauma, accounting for approximately 3% to 5% of all fractures. These injuries exhibit a classic bimodal epidemiological distribution. High-energy mechanisms, such as motor vehicle collisions, motorcycle accidents, and high-velocity ballistic trauma, predominantly affect younger male demographics. Conversely, low-energy mechanisms, typically ground-level falls resulting in torsional or bending forces, are the primary etiology in the older, osteoporotic female population. The unique anatomical characteristics of the humerus, combined with the extensive compensatory range of motion provided by the adjacent shoulder and elbow joints, make it highly amenable to nonoperative management in the vast majority of isolated injuries. As Sir John Charnley famously stated, “It is perhaps the easiest of the major long bones to treat by conservative methods.”
Because the upper extremity is not subjected to the weight-bearing demands of the lower extremity, the humerus exhibits a remarkable tolerance for radiographic imperfections. Small amounts of shortening, angulation, and rotation typically result in minimal functional deficit and are exceedingly well tolerated by the patient. However, the paradigm of treatment shifts dramatically in the presence of polytrauma, open injuries, or specific fracture patterns, necessitating a thorough understanding of both conservative and operative principles. Historically, conservative treatment modalities included skeletal traction, abduction casting, Velpeau dressings, and hanging arm casts. While each method has historical significance, functional bracing has essentially rendered them obsolete, emerging as the undisputed "gold standard" for nonoperative treatment.
Initially popularized by Sarmiento in 1977, functional bracing relies on three core biomechanical principles. First, the hydraulic effect: the rigid brace compresses the soft tissues (muscle and fascia) surrounding the fracture, creating a stabilizing hydrostatic column. Second, active muscle contraction: isometric and isotonic contractions of the biceps, triceps, and brachialis align the fracture fragments. Third, gravity: the dependent position of the arm provides a continuous, mild traction force that restores length and corrects angulation. The standard protocol involves the initial application of a coaptation splint or hanging arm cast for the first 7 to 10 days to allow acute swelling and pain to subside. Once the acute phase resolves, the patient is transitioned to a prefabricated functional brace. Pendulum exercises are initiated early, and functional use of the extremity is encouraged as tolerated, though active shoulder abduction should be avoided until clinical stability is achieved.
The brace is maintained until the patient is pain-free and radiographic union is evident. Union rates of 96% to 100% have been consistently reported, even in distal-third fractures. Acceptable radiographic reduction parameters dictate that shortening should be less than 3 cm, angulation less than 20 degrees (varus/valgus or apex anterior/posterior), and rotation less than 30 degrees. Skin maceration is a primary concern with functional bracing; therefore, meticulous daily hygiene must be stressed to the patient. While morbid obesity may increase the risk of varus deformities due to the fulcrum effect of the chest wall, these deformities are primarily cosmetic and rarely impair function.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the osseous and soft-tissue anatomy of the arm is paramount for safe surgical intervention and accurate fracture reduction. The humeral shaft is relatively cylindrical in its proximal and middle thirds, gradually transitioning into a flattened, triangular cross-section in its distal third as it flares to form the medial and lateral supracondylar ridges. This transition zone is a common site for fractures and poses unique biomechanical challenges for plate fixation, often requiring specialized pre-contoured plates or dual-plating techniques to achieve adequate distal purchase.
The deforming forces acting upon a humeral shaft fracture are dictated entirely by the relationship of the fracture line to the major muscular insertions. For fractures occurring proximal to the pectoralis major insertion, the proximal fragment is abducted and externally rotated by the rotator cuff. When the fracture occurs between the pectoralis major and the deltoid tuberosity, the proximal fragment is drawn medially by the pectoralis major, latissimus dorsi, and teres major, while the distal fragment is pulled proximally and laterally by the deltoid. For fractures distal to the deltoid tuberosity, the proximal fragment is abducted by the deltoid, and the distal fragment is drawn proximally by the biceps and triceps. Understanding these vectors is critical for executing closed reductions and planning the trajectory of interfragmentary compression.
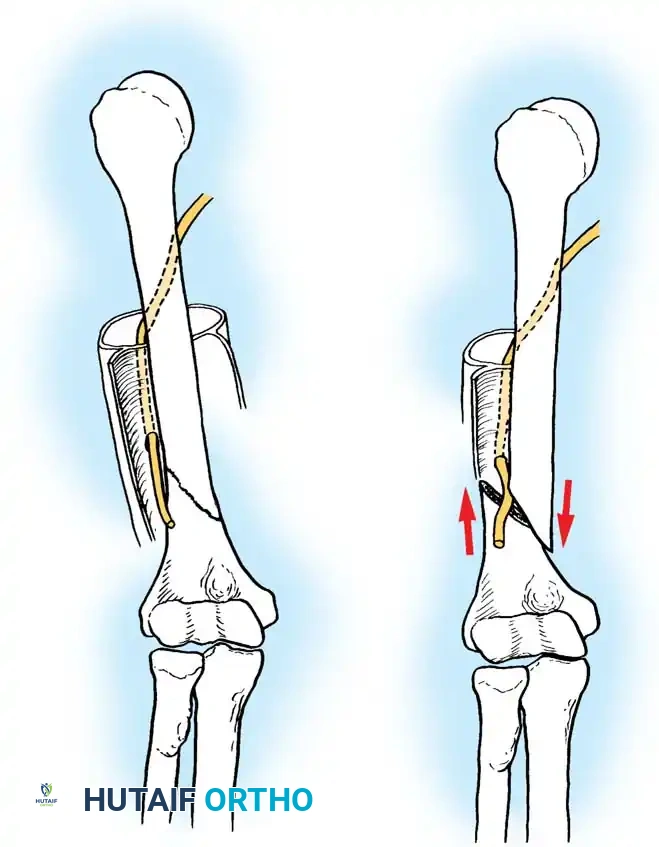
The neurovascular anatomy of the arm is arguably the most critical consideration in humeral shaft surgery, with the radial nerve commanding the utmost respect. The radial nerve originates from the posterior cord of the brachial plexus and courses posterior to the proximal humerus before entering the spiral groove (radial sulcus). It travels obliquely across the posterior humerus from medial to lateral, accompanied by the profunda brachii artery. Landmark cadaveric studies have demonstrated that the radial nerve lies directly on the periosteum of the posterior humerus, traversing the spiral groove approximately 20 cm distal to the acromion and 14 cm proximal to the lateral epicondyle. It pierces the lateral intermuscular septum to enter the anterior compartment approximately 10 cm proximal to the radiocapitellar joint. This anatomical course makes the nerve highly susceptible to injury during middle and distal third fractures (the classic Holstein-Lewis fracture), as well as during lateral and posterior surgical approaches.
Biomechanically, the humeral shaft is subjected to complex torsional, bending, and compressive forces during activities of daily living. Plate osteosynthesis provides superior resistance to torsional forces compared to intramedullary nailing. The application of a broad 4.5-mm limited-contact dynamic compression plate (LC-DCP) acts as a tension band when applied to the tension side of the bone. In transverse fractures, dynamic compression achieves primary bone healing through absolute stability. In oblique or spiral fractures, an interfragmentary lag screw provides absolute stability, while the plate functions in a neutralization mode. In highly comminuted fractures, bridge plating preserves the soft-tissue envelope and periosteal blood supply, adhering to the principles of relative stability and secondary bone healing via callus formation.


Exhaustive Indications and Contraindications
The decision to proceed with operative intervention is multifactorial and requires a nuanced assessment of the fracture pattern, associated soft-tissue injuries, and the patient's overall physiological status. While conservative management with functional bracing remains the gold standard for isolated, closed humeral shaft fractures, there are distinct absolute and relative indications for surgical stabilization. McKee systematically categorized the indications for surgery into three distinct domains: Fracture Indications, Associated Injuries, and Patient Indications.
Fracture indications include the failure to obtain or maintain adequate closed reduction that falls within the previously defined acceptable parameters. Segmental fractures represent a high risk of nonunion due to the severe disruption of the endosteal blood supply to the intercalary segment, making surgical stabilization highly favorable. Pathological fractures inherently require stabilization, often augmented with polymethylmethacrylate (PMMA) or tumor resection and reconstruction. Furthermore, fractures with displaced intra-articular extension into the shoulder or elbow joints demand anatomical reduction and rigid fixation to prevent post-traumatic arthrosis and joint stiffness.
Associated injuries provide some of the most compelling absolute indications for immediate surgery. Open wounds require urgent formal irrigation, debridement, and skeletal stabilization. Vascular injuries, particularly those involving the brachial artery, necessitate rigid skeletal fixation either prior to or immediately following vascular repair to protect the anastomosis. The "floating elbow" (ipsilateral humeral shaft and forearm fractures) mandates stabilization of at least the humerus, and typically both segments, to allow for early mobilization and prevent severe stiffness. Polytrauma patients, particularly those requiring upper extremity weight-bearing for crutch use due to concomitant lower extremity fractures, benefit immensely from the early mobilization afforded by plate osteosynthesis.
Operative Indications and Contraindications Table
| Category | Absolute Indications | Relative Indications | Absolute Contraindications |
|---|---|---|---|
| Fracture Pattern | Displaced intra-articular extension | Segmental fractures | Undisplaced, stable fractures |
| Pathological fractures | Failure of closed reduction | Acceptable alignment in brace | |
| Associated Injuries | Vascular injury requiring repair | Brachial plexus injury | Active, untreated deep infection |
| Open fractures (Gustilo II, III) | Ipsilateral shoulder/elbow fx | Severe burns over surgical site | |
| "Floating elbow" | Bilateral humeral fractures | ||
| Patient Factors | Polytrauma (Damage Control) | Morbid obesity (poor brace fit) | Medically unfit for anesthesia |
| Severe head injury (GCS ≤ 8) | Patient refusal | ||
| Non-compliance with bracing |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful humeral shaft osteosynthesis. Radiographic evaluation must include high-quality, orthogonal anteroposterior (AP) and lateral radiographs of the entire humerus, extending from the glenohumeral joint to the elbow. In cases of severe comminution, pathological lesions, or suspected intra-articular extension, a computed tomography (CT) scan with 3D reconstructions is highly recommended to delineate the fracture morphology and plan screw trajectories.
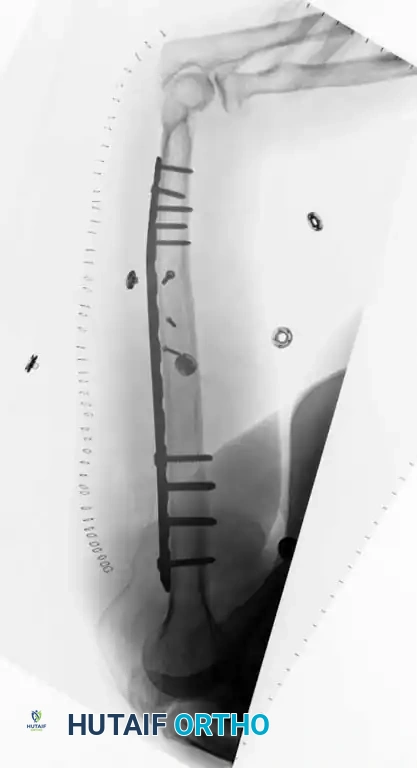
Digital templating is mandatory to determine the appropriate plate length and screw sizes. The biomechanical principle for diaphyseal plating dictates that a minimum of eight cortices (four bicortical screws) of purchase must be obtained both proximal and distal to the fracture zone to prevent hardware failure and screw pullout. In the setting of osteoporotic bone, the working length of the construct should be maximized by utilizing longer plates, and the use of locking screws or methylmethacrylate augmentation should be anticipated. The surgeon must ensure that a full complement of broad and narrow 4.5-mm LC-DCPs, 3.5-mm pelvic reconstruction plates (for dual plating), and pre-contoured extra-articular distal humerus plates are available in the operating theater.
Patient positioning is dictated entirely by the chosen surgical approach, which in turn is determined by the fracture location. For the anterolateral approach, the patient is positioned supine or in a modified beach-chair position. The arm is draped free on an arm board, allowing for full range of motion of the shoulder and elbow to facilitate reduction. A sterile tourniquet may be applied as high as possible on the arm, though many surgeons prefer to operate without a tourniquet to avoid tethering the triceps and impeding distal exposure.
For the posterior approaches (triceps-splitting or triceps-reflecting), the lateral decubitus position is heavily favored. The patient is secured with a beanbag, and all bony prominences are meticulously padded. The operative arm is draped free over a sterile padded post (such as a Mayo stand or specialized arm holder), allowing the elbow to flex to 90 degrees. This position utilizes gravity to assist with fracture reduction and provides unparalleled, ergonomic access to the posterior aspect of the humerus. Alternatively, the prone position can be utilized, though it complicates airway management and restricts access to the anterior chest and abdomen, making it less ideal for polytrauma patients.
Step-by-Step Surgical Approach and Fixation Technique
The choice of surgical approach is dictated by the fracture location and the planned construct. The anterolateral approach (brachialis-splitting) is ideal for fractures of the proximal and middle thirds of the humeral shaft. The internervous plane lies proximally between the deltoid (axillary nerve) and pectoralis major (medial/lateral pectoral nerves), and distally it splits the brachialis muscle. The lateral half of the brachialis is innervated by the radial nerve, and the medial half by the musculocutaneous nerve, making this a safe, denervation-free split. However, for midshaft fractures extending into the distal third, the posterior approaches are vastly superior.
Modified Posterior Approach (Triceps-Reflecting) [TECHNIQUE 54-6]
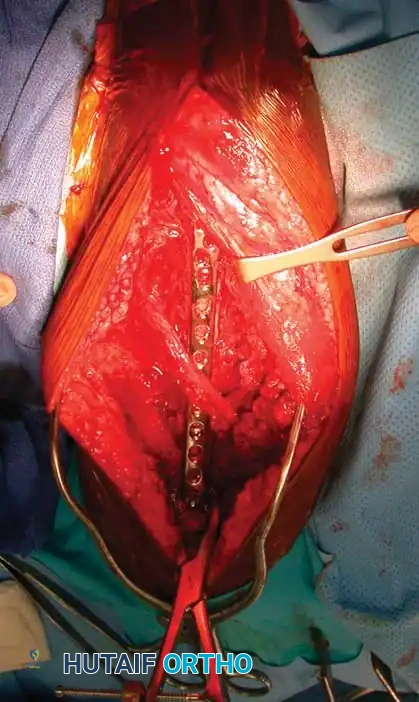
This approach is highly favored for complex mid-to-distal third fractures requiring extensive plating. The patient is placed in the lateral decubitus position with the operative arm draped over a padded post. A wide proximal preparation is performed to allow for the application of a sterile tourniquet if necessary. A longitudinal incision is made starting from the level of the tourniquet, extending distally to the tip of the olecranon, perfectly in line with the posterior axis of the humerus.
The dissection is carried sharply down through the subcutaneous tissue to identify the triceps fascia. The fascia is incised longitudinally, and the fascial dissection is carried laterally to identify the lateral intermuscular septum.
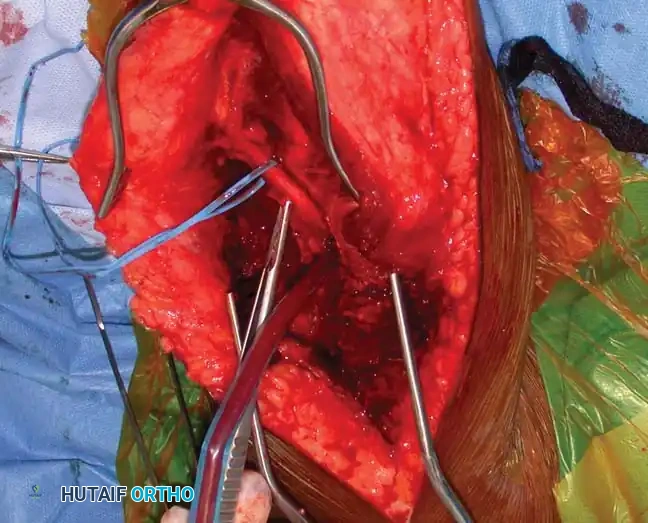
Carefully identify and protect the lateral brachial cutaneous nerve, which serves as a reliable guide to the radial nerve.
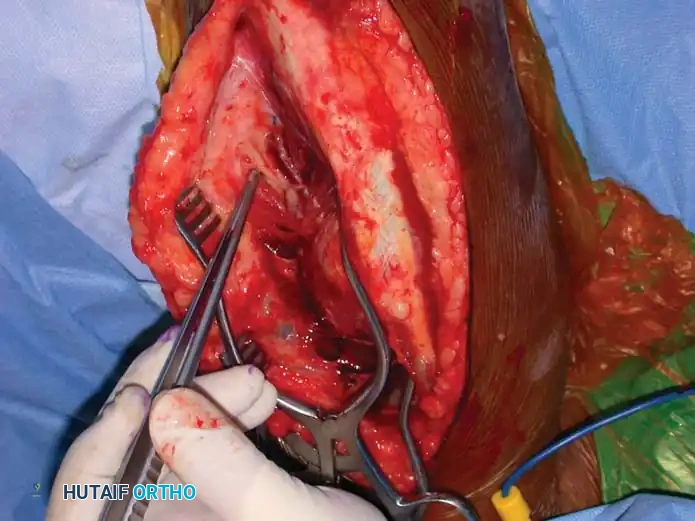
Elevate the lateral head of the triceps off the lateral intermuscular septum. Identify the radial nerve and the profunda brachii artery as they pierce the lateral intermuscular septum to enter the anterior compartment. Carefully mobilize the radial nerve. Use vessel loops for gentle retraction. Never apply excessive traction to the radial nerve, as it is exquisitely sensitive to stretch injuries, which can precipitate an iatrogenic neuropraxia.
Once the radial nerve is safely identified and protected, the triceps muscle is mobilized. In the traditional triceps-splitting approach, the long and lateral heads are separated, and the medial head is split longitudinally. However, in the modified triceps-reflecting approach described by Gerwin et al., the entire triceps muscle mass is reflected medially off the lateral intermuscular septum and the posterior humerus. This reflection provides an average of 10 cm more of continuous distal exposure compared to the standard split, allowing for the placement of extensive plates without compressing the radial nerve beneath the hardware.



Fracture Reduction and Plate Osteosynthesis
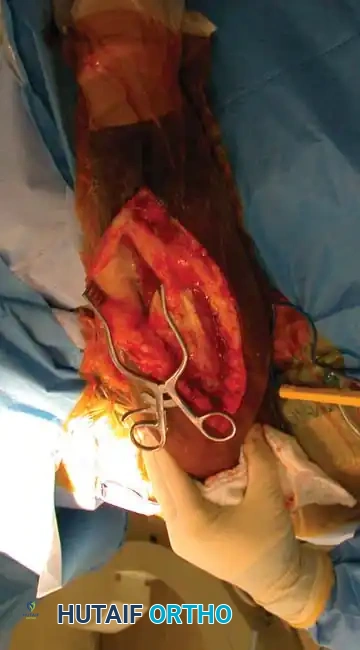
Following adequate exposure, the fracture ends are debrided of interposed soft tissue and hematoma. For spiral or oblique fractures, the Eglseder technique is employed: provisional reduction is achieved and held with a pointed reduction forceps, and an interfragmentary lag screw (typically 3.5 mm or 4.5 mm) is placed perpendicularly across the fracture plane to achieve absolute stability and anatomical reduction. A broad 4.5-mm LC-DCP is then contoured to the posterior aspect of the humerus and applied as a neutralization plate.

For transverse fractures, the plate is applied using dynamic compression principles. The plate is fixed to one main fragment, and the articulated tension device or eccentrically placed screws are utilized to axially compress the fracture site. For comminuted fractures, a bridge plating technique is utilized. The fracture zone is left relatively undisturbed to preserve the periosteal blood supply. A long plate is applied spanning the comminution, secured with at least four bicortical screws proximal and distal to the fracture, restoring length, alignment, and rotation.


Alternative Modalities: Intramedullary Nailing and External Fixation
While plating remains the gold standard, intramedullary (IM) nailing has specific indications, particularly for pathological fractures or severe segmental injuries where extensive soft-tissue stripping is contraindicated. Antegrade nailing requires a rotator cuff-splitting approach, which has been strongly associated with postoperative shoulder pain and impingement. Retrograde nailing avoids the rotator cuff but carries a significant risk of iatrogenic supracondylar fractures and requires meticulous identification of the distal entry portal just proximal to the olecranon fossa.


External fixation is strictly reserved for damage-control orthopedics in the hemodynamically unstable polytrauma patient, or in cases of massive soft-tissue defects, high-energy gunshot wounds, or gross contamination where internal hardware would pose an unacceptable risk of deep infection. Unilateral half-pin frames are typically utilized, with pins placed safely in the proximal lateral humerus and the distal lateral humerus, carefully avoiding the course of the radial nerve.

Minimally Invasive Plate Osteosynthesis (MIPO)
MIPO techniques have gained traction to minimize soft-tissue disruption. However, cadaveric studies by Apivatthakakul et al. demonstrated that the plate sits an average of 3.2 mm from the radial nerve. Pronation of the forearm moves the nerve even closer (by 3 mm). Due to these severe risks of iatrogenic nerve injury, anterior MIPO techniques must be executed with extreme caution and are generally reserved for highly experienced surgeons utilizing meticulous fluoroscopic guidance.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and adherence to biomechanical principles, complications following the management of humeral shaft fractures can and do occur. The most widely discussed and feared complication is radial nerve palsy. Primary radial nerve palsy presents at the time of injury and occurs in approximately 11% to 18% of all humeral shaft fractures, with the highest incidence seen in middle-to-distal third spiral fractures (the Holstein-Lewis pattern). The vast majority of these primary palsies represent neuropraxias or axonotmesis and will recover spontaneously within 3 to 6 months. Therefore, expectant management with a dynamic wrist extension splint is the standard of care for closed fractures with primary palsy.
However, secondary radial nerve palsy—which presents after a closed reduction attempt or post-operatively—demands a different algorithm. If a palsy develops immediately following closed reduction, it may indicate nerve entrapment within the fracture site, necessitating prompt surgical exploration. Iatrogenic nerve palsy following plate osteosynthesis requires careful review of the intraoperative events; if the nerve was directly visualized and protected, expectant management is appropriate. If the nerve was not visualized (such as in MIPO or blind nailing), early exploration is heavily advised. Electromyography and nerve conduction studies (EMG/NCS) should be obtained at 6 weeks post-injury to establish a baseline and assess for early signs of reinnervation (fibrillation potentials).
Nonunion is another significant complication, occurring in 2% to 10% of cases treated nonoperatively, and up to 15% in some operative series, particularly following IM nailing of transverse fractures. Hypertrophic nonunions indicate adequate biology but insufficient mechanical stability, and are typically salvaged with rigid plate osteosynthesis. Atrophic nonunions indicate a failure of biology and require rigid stabilization combined with biological augmentation, most commonly utilizing autologous iliac crest bone graft (ICBG). In recalcitrant cases, the use of dual plating or a vascularized free fibular graft may be necessary.
Complications and Management Table
| Complication | Incidence Rate | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Radial Nerve Palsy (Primary) | 11% - 18% | Trauma (Holstein-Lewis fx, penetrating injury) | Expectant management; dynamic splinting; EMG at 6 wks. Explored if no recovery at 4-6 mos. |
| Radial Nerve Palsy (Secondary) | 2% - 5% | Entrapment post-reduction, iatrogenic stretch/ligation | Early surgical exploration if entrapment or ligation is suspected. |
| Nonunion | 2% - 15% | Segmental fx, poor stability, smoking, IM nailing | Rigid plate osteosynthesis + autologous ICBG (for atrophic). |
| Infection (Deep) | 1% - 3% | Open fractures, prolonged surgical time, diabetes | Serial I&D, hardware removal if loose, external fixation, targeted IV antibiotics. |
| Hardware Failure | < 2% | Inadequate plate length, early weight-bearing, osteopenia | Revision osteosynthesis with longer plate, locking screws, PMMA augmentation. |
| Shoulder Impingement | 10% - 30% (IM Nails) | Prominent proximal hardware, rotator cuff splitting | Hardware removal after union, rotator cuff repair/debridement. |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of humeral shaft fracture management, whether operative or nonoperative, relies heavily on a structured, phased rehabilitation protocol. The primary goal is to restore full, painless range of motion and strength to the shoulder and elbow while protecting the healing fracture or osteosynthesis construct.
Phase I: Acute Protective Phase (0 to 2 Weeks)
In the immediate post-operative period, the extremity is immobilized in a sling or coaptation splint for comfort. The primary focus is on edema control, wound healing, and pain management. Active and active-assisted range of motion of the wrist and digits is initiated immediately to prevent distal stiffness and encourage venous return. Gentle, passive pendulum exercises for the shoulder are introduced within the first few days, provided the fracture fixation is deemed mechanically stable. Strict avoidance of active shoulder abduction and external rotation is enforced to prevent excessive torsional stress on the plate or intramedullary nail.
Phase II: Early Mobilization Phase (2 to 6 Weeks)
Once the surgical incisions have healed and early soft callus formation is evident radiographically (or clinical stability is achieved in braced patients), the rehabilitation protocol advances. Active-assisted range of motion for the shoulder (using pulleys or a wand) and elbow is initiated. Isometrics for the deltoid, biceps, and triceps can begin, but heavy resistance is strictly prohibited. The patient is instructed to use the arm for light activities of daily living, keeping the elbow close to the body to minimize the lever arm effect on the humerus.
Phase III: Strengthening Phase (6 to 12 Weeks)
Progression to Phase III requires radiographic evidence of bridging callus and an absence of pain at the fracture site upon palpation or stress. Active range of motion is advanced to achieve full functional arcs of the shoulder and elbow. Progressive resistance exercises using elastic bands or light weights are incorporated to rebuild the atrophied musculature. Scapular stabilization exercises are critical during this phase to correct any dyskinesia that may have developed during the period of relative immobilization.
Phase IV: Return to Function (>12 Weeks)
In the final phase, the focus shifts to work-hardening or sport-specific training. Heavy lifting, pushing, and pulling are gradually reintroduced. Full radiographic union (bridging of at least three out of four cortices on orthogonal views) must be confirmed prior to clearing the patient for contact sports or heavy manual labor. Patients who underwent antegrade intramedullary
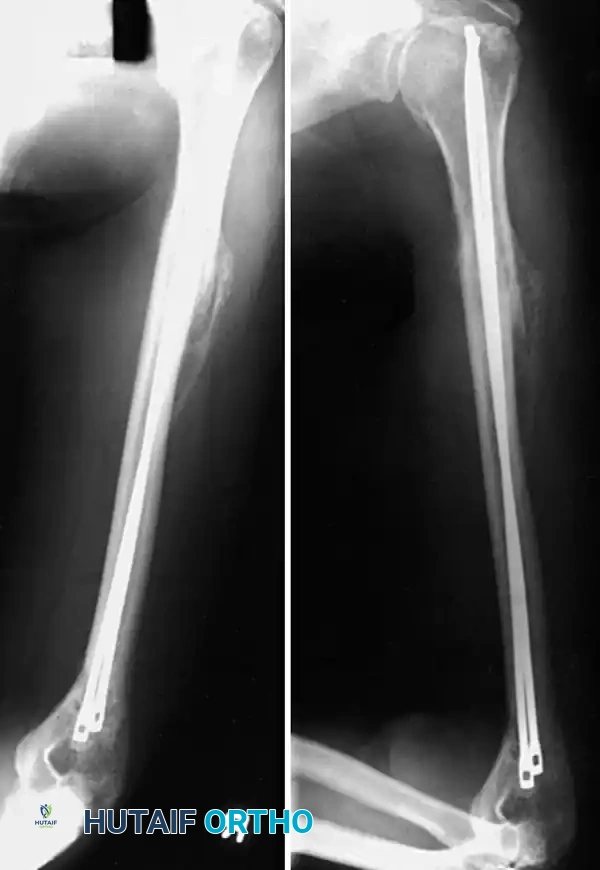
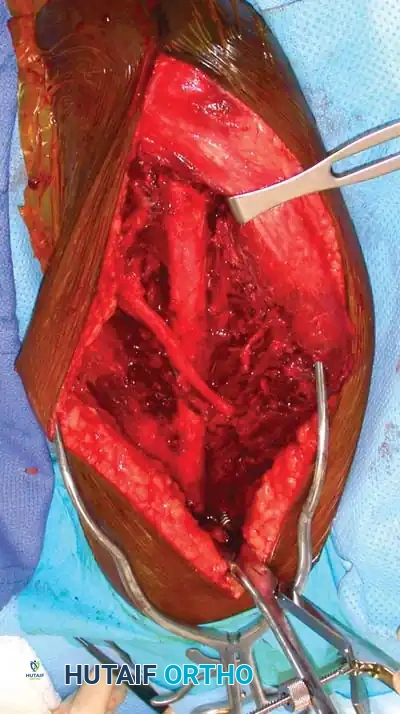
Clinical & Radiographic Imaging Archive