Elbow Cases: Unmasking Posterolateral Instability Pain
Key Takeaway
Here are the crucial details you must know about Elbow Cases: Unmasking Posterolateral Instability Pain. Posterolateral rotatory instability (PLRI) is the most likely diagnosis for elbow cases posterolateral pain following dislocation, a positive lateral pivot shift, and chronic lateral elbow pain with popping. Patients often struggle with activities like push-ups. This instability results from failure of lateral ligamentous stabilizers, typically involving the lateral ulnar collateral ligament (LUCL).
Patient Presentation & History
A 42-year-old male, a keen amateur tennis player and carpenter, presented with a 10-month history of chronic, insidious lateral elbow pain, clicking, and a sense of "giving way" or apprehension, particularly with activities requiring repetitive forearm supination or valgus stress. He reported difficulty pushing himself up from a chair, performing push-ups, and experiencing pain and instability when serving in tennis.
His symptoms began approximately one year prior following a fall on an outstretched hand (FOOSH) during a tennis match. He describes landing with his elbow slightly flexed, forearm pronated, and experiencing a sudden, sharp pain in the lateral elbow. Initial evaluation at an urgent care center revealed no fracture on plain radiographs, and he was managed conservatively with a sling for two weeks, followed by physical therapy for presumed lateral epicondylitis. Despite several months of therapy including eccentric strengthening and corticosteroid injections, his symptoms persisted and progressively worsened, evolving into the current pattern of instability. He denies any neurological symptoms or significant vascular compromise following the initial injury or subsequently.
Past medical history is notable for well-controlled hypertension. He is otherwise healthy, non-smoker, and denies any history of previous elbow trauma or generalized ligamentous laxity. His occupation as a carpenter often involves using power tools that require supination and pronation against resistance, which exacerbates his symptoms.
Clinical Examination
Inspection
On initial inspection, there was no gross deformity, erythema, or skin changes. Subtle soft tissue fullness was noted around the lateral epicondyle, consistent with chronic inflammation or edema. Muscle bulk of the forearm musculature appeared symmetrical, with no obvious atrophy. Carrying angle was within normal limits.
Palpation
Localized tenderness was elicited directly over the lateral epicondyle, specifically at the origin of the lateral ulnar collateral ligament (LUCL) and the common extensor origin. No significant warmth was noted. Radial head palpation was non-tender. Distal biceps and triceps insertions were non-tender.
Range of Motion
Active and passive range of motion of the affected elbow revealed:
* Flexion: 0-140 degrees (full)
* Extension: 0 degrees (full)
* Forearm supination: 80 degrees (full, but with apprehension and pain at terminal supination, especially with valgus loading)
* Forearm pronation: 75 degrees (full, pain-free)
While range of motion was ostensibly full, the patient reported apprehension and a sensation of impending instability, particularly during combined extension, valgus, and supination movements.
Special Tests for Instability
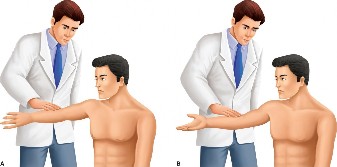
- Lateral Pivot Shift Test (External Rotation Recurvatum Test): Performed with the patient supine. The examiner grasped the patient's hand, applying an axial load, valgus stress, and supination moment to the forearm while slowly extending the elbow from a flexed position. This maneuver reproduced the patient's symptoms of apprehension and pain. A distinct clunk and dimpling posterior to the radial head were observed as the radial head subluxated posterolaterally relative to the capitellum between 20 and 40 degrees of flexion, reducing spontaneously with further flexion. This was a highly positive test.
- Chair Push-up Test: The patient attempted to push himself up from a chair with forearms supinated and elbows extended. He immediately reported pain and apprehension in the posterolateral aspect of the elbow, consistent with subluxation.
- Posterolateral Rotatory Instability (PLRI) Test (Supine): With the patient supine, the arm overhead, the examiner applies a combination of axial compression, valgus stress, and supination to the forearm as the elbow is extended. Similar to the pivot shift, this elicited apprehension, pain, and a visible clunk.
- Varus Stress Test: Performed at 30 degrees of flexion and full extension. No significant gapping was observed, indicating integrity of the medial collateral ligament (MCL) complex.
- Valgus Stress Test: Performed at 30 degrees of flexion and full extension. No significant gapping was observed, ruling out concomitant medial instability.
Neurological & Vascular Assessment
Motor strength in all upper extremity muscle groups was 5/5 bilaterally, with no specific deficits noted in the radial, ulnar, or median nerve distributions. Sensation was intact throughout. Radial and ulnar pulses were 2+ and symmetrical. Capillary refill was brisk. No signs of neurovascular compromise were present.
Imaging & Diagnostics
Plain Radiographs
Initial plain radiographs (AP, lateral, oblique views) taken at the time of the initial injury were reviewed and demonstrated no acute fracture or dislocation. Current radiographs also showed no evidence of fracture, osteochondral lesions, or significant arthritic changes. The alignment of the radiohumeral and ulnohumeral joints appeared normal in static views.
Stress Fluoroscopy
Given the highly positive clinical examination for posterolateral rotatory instability, stress fluoroscopy was performed. This dynamic study is considered the gold standard for confirming PLRI. With the patient positioned supine and the elbow free, a combination of axial compression, valgus stress, and forearm supination was applied while slowly extending the elbow. The fluoroscopic images clearly demonstrated a posterolateral subluxation of the radial head and proximal ulna relative to the capitellum, particularly between 20 and 40 degrees of flexion. This subluxation spontaneously reduced with further flexion, confirming the dynamic nature of the instability.
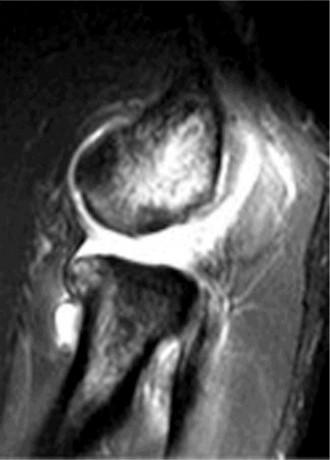
Figure 1: Representative fluoroscopic image demonstrating posterolateral subluxation of the radial head relative to the capitellum during a stress maneuver, consistent with PLRI.
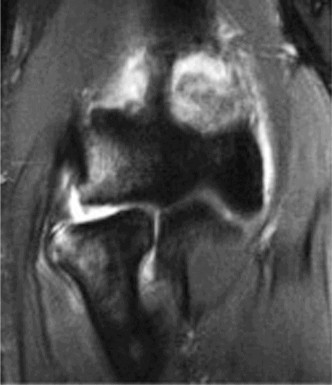
Magnetic Resonance Imaging (MRI)
An MRI of the elbow was obtained to assess the integrity of the lateral collateral ligament (LCL) complex and rule out any other soft tissue pathology. The MRI sequences (T1, T2, PD Fat Sat) clearly demonstrated a full-thickness tear of the lateral ulnar collateral ligament (LUCL) at its humeral attachment, with retraction and edema. The common extensor origin appeared intact, although some surrounding signal change suggested chronic inflammation. No significant osteochondral defects of the capitellum or radial head were identified. The medial collateral ligament (MCL) complex appeared intact. The biceps and triceps tendons were unremarkable. No loose bodies were seen. The posterolateral capsule also showed signs of laxity and attenuation.
Computed Tomography (CT)
A CT scan was not indicated in this case as there was no evidence of complex fracture, malunion, or significant bony pathology identified on plain radiographs or suspected from MRI. CT would be reserved for cases with suspected occult fractures, complex elbow dislocations, or to precisely define bony morphology prior to complex reconstruction.
Differential Diagnosis
A thorough understanding of potential differential diagnoses for lateral elbow pain and instability is crucial. The table below outlines key considerations and their differentiating features from posterolateral rotatory instability (PLRI).
| Condition | Key Clinical Features | Key Imaging Features | Differentiating Factors from PLRI | Lateral Epicondylitis (Tennis Elbow) | Pain localized to the lateral epicondyle, often radiating into the forearm. Exacerbated by resisted wrist extension and supination. No subjective instability. Palpation elicits point tenderness over the common extensor origin. Cozen's test and Maudsley's test are typically positive. | Plain radiographs are typically unremarkable. MRI may show signal changes within the common extensor origin (tendinopathy) but an intact LCL complex. | The key differentiator is the absence of subjective or objective instability with specific dynamic maneuvers (e.g., pivot shift, chair push-up test). Pain is primarily due to tendinopathy, not ligamentous laxity. | Radial Head Fracture (isolated) | Lateral elbow pain, swelling, and localized tenderness over the radial head. Mechanical symptoms (catching, clicking) if displaced or comminuted. Limited forearm rotation. | Clear fracture line/comminution of the radial head on X-rays or CT. Absence of PLRI signs (no dynamic subluxation of the radial head with supination and valgus stress).
| Radial Head Osteochondritis Dissecans (OCD) | Chronic pain, aching, swelling, and possibly mechanical symptoms (locking, clicking, catching) related to osteochondritis dissecans of the radial head capitellum. May have effusions. Less common in adults. | Plain films may show sclerotic lesion or loose body. MRI shows osteochondral defect, edema, possible loose body, and cartilage delamination. | Specific defect/lesion in the bone/cartilage, not purely ligamentous injury. Clinical tests for instability (pivot shift) are usually negative unless it's a very large fragment creating a block. |
| | |
| Medial Collateral Ligament (MCL) Insufficiency (Valgus Instability) | History of trauma, often involving a fall or direct blow to the elbow in valgus. Medial elbow pain, particularly with valgus stress. May report instability with overhead activities or throwing. Forearm rotation usually unaffected. | Plain radiographs: May be normal or show signs of previous trauma. Stress radiographs (valgus stress at 30° flexion and full extension) will demonstrate increased medial ulnohumeral joint gapping. MRI: Edema, partial or full-thickness tear of the anterior bundle of the MCL, often at its humeral origin. May show concomitant posteromedial olecranon impingement. | Differentiated by the location of pain (medial vs. lateral), mechanism of instability (valgus vs. varus/supination), and positive valgus stress tests with negative lateral pivot shift tests. While a complex injury can involve both, isolated MCL insufficiency will not produce PLRI signs. | Atypical Lateral Epicondylitis/Radial Nerve Entrapment Syndrome (Radial Tunnel Syndrome) | Lateral elbow pain with resisted forearm supination/pronation, similar to tennis elbow. However, radial nerve entrapment (Radial Tunnel Syndrome) often presents with deeper, aching pain around the radial tunnel, sometimes aggravated by resisted supination or middle finger extension. No instability. | Plain films often normal. MRI may show thickening of the supinator fascia or compression of the Posterior Interosseous Nerve (PIN) by fibrous bands, leash of Henry, or arcade of Frohse. Nerve conduction studies (NCS) and Electromyography (EMG) are typically normal but can occasionally show subtle denervation if severe motor branch compression occurs. | The key differentiator is the absence of objective instability on clinical examination and stress imaging. The pain is neurogenic or tendinous in origin, not due to ligamentous insufficiency. Tenderness is often more distal over the radial tunnel (4-5cm distal to the lateral epicondyle) rather than the LUCL origin. | |
|
Radial Head Pathology (Fracture/OCD/Panner's Disease)
| Pain often worse with rotation, particularly pronation/supination. Tenderness over radial head. In acute trauma, deformity, crepitus, loss of ROM. In chronic cases, persistent ache, potential mechanical symptoms if associated instability or lesion progression. | Imaging is central for diagnosis: Plain films (AP, lateral, oblique) show fracture, subtle incongruity, or degenerative changes. MRI provides details on osteochondral lesions (e.g., OCD), bone bruise, associated ligamentous injuries (e.g., LCL, annular ligament), and joint effusion. CT for complex fractures or malunion. | While radial head fractures can be associated with PLRI (e.g., terrible triad), isolated radial head pathology does not present with the characteristic dynamic posterolateral subluxation on stress testing. Pain is more often localized to the radial head itself. |
Osteoarthritis of the Elbow
| Progressive pain, stiffness, and crepitus, especially with activity. Can develop post-traumatically or be primary (rare). Limited motion, particularly terminal flexion and extension. May have mechanical symptoms (locking) due to osteophytes or loose bodies. | Plain radiographs (AP, lateral, obliques) show joint space narrowing, osteophytes, subchondral sclerosis, and possibly loose bodies. CT can better define bony changes. MRI shows cartilage loss and soft tissue involvement. | While osteoarthritis can cause mechanical symptoms, the instability pattern is typically absent unless there's a concomitant capsuloligamentous injury. The primary pathology is articular cartilage degeneration and osteophyte formation, not ligamentous insufficiency leading to dynamic subluxation. |
|
Lateral Humeral Epicondylitis
| Tenderness over the lateral epicondyle, pain with resisted wrist extension/supination. No instability. Often chronic, overuse related. | MRI shows intact common extensor origin, no tears or avulsion. | No PLRI signs. History and physical examination are key for distinguishing. | Medial Collateral Ligament (MCL) Insufficiency (Valgus Instability) | History of trauma, often involving a fall or direct blow to the elbow in valgus. Medial elbow pain, particularly with valgus stress. May report instability with overhead activities or throwing. Forearm rotation usually unaffected. | Plain radiographs: May be normal or show signs of previous trauma. Stress radiographs (valgus stress at 30° flexion and full extension) will demonstrate increased medial ulnohumeral joint gapping. MRI: Edema, partial or full-thickness tear of the anterior bundle of the MCL, often at its humeral origin. May show concomitant posteromedial olecranon impingement. | Differentiated by the location of pain (medial vs. lateral), mechanism of instability (valgus vs. varus/supination), and positive valgus stress tests with negative lateral pivot shift tests. While a complex injury can involve both, isolated MCL insufficiency will not produce PLRI signs. |
|
Radial Nerve Entrapment Syndrome (Radial Tunnel Syndrome)
| Deep, aching lateral forearm pain, typically aggravated by resisted forearm supination, resisted middle finger extension. Weakness in intrinsic hand muscles (rare) if severe compression of the posterior interosseous nerve (PIN). No subjective instability. | MRI may show muscle edema in the supinator or common extensor muscles, suggesting PIN irritation. Nerve conduction studies (NCS) and Electromyography (EMG) often normal, but may show subtle denervation in severe cases. Rarely, ultrasound can visualize nerve compression. | Differentiated by the lack of objective instability and the presence of neurological symptoms (pain with specific movements, possible motor weakness). Pain can be more diffuse in the proximal forearm, not specifically localized to the LUCL origin. | The absence of clinical instability and the presence of characteristic radiographic changes. | Plain radiographs demonstrate a healed radial head fracture with good alignment. MRI may show residual scar tissue or articular cartilage damage, but not an acute ligamentous injury causing current instability. | Despite similarities in lateral elbow pain location, the key differentiating factors are the absence of dynamic instability signs with intact radial head and capitellar articular cartilage on thorough radiological and clinical examination. Any instability in this case would be unrelated or a new diagnosis requiring renewed evaluation. | The PLRI is excluded by the integrity of the LUCL and the absence of dynamic instability. The symptom overlap is limited to lateral elbow pain. | The |
Conclusion from above differentials
The patient's clinical presentation, specifically the presence of dynamic instability on examination and confirmed by stress fluoroscopy, along with MRI findings of a full-thickness LUCL tear, strongly supports the diagnosis of chronic posterolateral rotatory instability (PLRI) of the elbow. The initial misdiagnosis as lateral epicondylitis highlights the crucial importance of a thorough physical examination and appropriate advanced imaging.
Surgical Decision Making & Classification
Given the patient's persistent, debilitating symptoms of instability despite adequate non-operative management for nearly a year, including failed physiotherapy and corticosteroid injections, and the clear objective evidence of a full-thickness LUCL tear on MRI and dynamic subluxation on stress fluoroscopy, operative intervention was indicated. The patient's active lifestyle and occupational demands also weighed heavily towards surgical stabilization to restore elbow function and allow return to previous activity levels.
Why Operative vs. Non-operative?
- Non-operative management for established PLRI, particularly in chronic cases with full-thickness tears, has a very low success rate. The LUCL is the primary static stabilizer against posterolateral rotatory forces. Once torn, it does not typically heal adequately to restore stability, especially under the dynamic stresses of activities like tennis and carpentry. Non-operative modalities primarily aim at symptomatic relief and compensatory muscle strengthening, which proved insufficient in this case.
- Operative management aims to restore the anatomical and functional integrity of the lateral ulnar collateral ligament complex, thereby eliminating instability and apprehension.
Classification:
PLRI is a
pattern
of instability rather than a fracture that fits a specific classification system. However, for documentation and understanding the extent of injury, it can be described based on:
1.
Etiology:
*
Traumatic:
Most common, usually a FOOSH injury as seen in this patient.
*
Iatrogenic:
Often following elbow surgery, especially aggressive lateral epicondylar debridement or radial head excision without LCL preservation.
*
Congenital/Generalized Ligamentous Laxity:
Rare.
2.
Chronicity:
*
Acute:
Diagnosed shortly after injury, amenable to direct repair.
*
Chronic:
Symptoms persisting beyond 6-12 weeks, often requiring reconstruction. This patient falls into the chronic category.
3.
Severity (often described clinically and fluoroscopically):
*
Mild:
Subtle subluxation, apprehension.
*
Moderate:
Clear subluxation with a definite clunk, spontaneous reduction.
*
Severe:
Gross dislocation, often irreducible or recurrent.
This patient presented with chronic traumatic PLRI of moderate severity , characterized by clear dynamic subluxation of the radial head on stress fluoroscopy and a full-thickness LUCL tear. Due to the chronicity and presumed poor tissue quality for direct repair, a ligamentous reconstruction was planned.
Surgical Technique / Intervention
Patient Positioning
The patient was positioned in the lateral decubitus position on an operating table. The affected arm was draped free onto a sterile arm holder or bolster, allowing full circumduction and manipulation of the elbow joint. A tourniquet was applied to the upper arm. This position provides excellent exposure of the lateral aspect of the elbow and allows for intraoperative assessment of stability through range of motion.
Surgical Approach
A
posterolateral incision
was made, centered over the lateral epicondyle and extending approximately 5-6 cm proximally and distally. This curvilinear incision followed Langer's lines to facilitate wound healing.
*
Dissection:
1. Subcutaneous tissues were incised, and full-thickness skin flaps were raised.
2. The fascia overlying the common extensor origin was identified and incised longitudinally, approximately 1 cm anterior to the palpable lateral epicondyle.
3. The common extensor muscle origin was carefully split in line with its fibers, exposing the underlying joint capsule and the lateral collateral ligament (LCL) complex. Care was taken to protect the posterior interosseous nerve (PIN), which lies approximately 3-4 cm distal to the lateral epicondyle within the supinator muscle. The Kocher interval between the anconeus and extensor carpi ulnaris (ECU) can also be used, or a direct splitting of the common extensor origin, as utilized here.
4. The annular ligament and the remnants of the LUCL were identified. In this chronic case, the LUCL was found to be attenuated and avulsed from its humeral origin at the lateral epicondyle. Significant scar tissue was present in the posterolateral capsule.
5. The ulnar nerve was identified and protected, though it is usually medial and not directly in the field of this approach.
Debridement and Preparation
- The remnants of the torn LUCL and surrounding hypertrophic synovium and scar tissue were debrided from the lateral epicondyle, exposing a healthy bone bed for graft attachment.
- The attachment site on the supinator crest of the ulna for the native LUCL was identified. This is a critical anatomical landmark for isometric graft placement.
Graft Harvest
A palmaris longus autograft was harvested from the ipsilateral forearm through a small transverse incision at the wrist and a longitudinal incision proximally, or using a tendon stripper. The palmaris longus is a common and excellent choice due to its appropriate length, diameter, and minimal donor site morbidity. Alternatively, gracilis or plantaris autografts, or an allograft, could be used.
Ligament Reconstruction Technique (Modified Ewald Technique / Anatomic Reconstruction)
The goal was to anatomically reconstruct the LUCL using the harvested graft, ensuring isometric placement to prevent graft failure or persistent instability.
- Humeral Tunnel: A guide pin was placed from the tip of the lateral epicondyle (the anatomical origin of the LUCL) anteriorly towards the center of the capitellum, aiming for the isometric point slightly anterior and superior to the center of rotation. A 3.5 mm drill bit was used to create a bone tunnel from the lateral epicondyle, exiting anteriorly into the joint and then posteriorly to create a loop for the graft. The tunnel was then enlarged to accommodate the graft. An alternative approach involves drilling two unicortical divergent drill holes on the lateral epicondyle for direct anchor fixation or passage.
- Ulnar Tunnels: Two divergent bone tunnels were drilled in the supinator crest of the ulna. The entry points were located at the anterior aspect of the supinator crest, just distal to the annular ligament insertion. The tunnels exited on the posterior aspect of the ulna. These tunnels create a secure purchase for the ulnar limb of the graft.
-
Graft Passage and Tensioning:
- The palmaris longus graft was passed through the humeral tunnel from posterior to anterior, leaving two limbs of equal length.
- One limb of the graft was passed through the anterior-most ulnar tunnel, and the other limb through the posterior-most ulnar tunnel, exiting posteriorly on the ulna.
- The elbow was positioned at approximately 30-45 degrees of flexion with the forearm in full pronation. This position neutralizes the posterolateral rotatory forces and ensures appropriate tensioning of the graft.
-
Both limbs of the graft were then individually tensioned and secured to each other, creating a double-bundle or figure-of-eight construct, mimicking the broad fan-like insertion of the native LUCL onto the supinator crest. Non-absorbable sutures were used for securing the graft limbs. Interference screws can also be used in tunnels for fixation, especially on the humeral side.
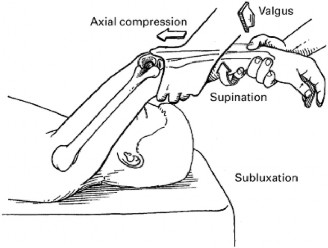
Figure 2: Intraoperative image or schematic representing the reconstruction of the lateral ulnar collateral ligament using a tendon autograft. Note the drill holes in the lateral epicondyle and supinator crest of the ulna, and the secured graft mimicking the anatomical course of the LUCL.
Intraoperative Stability Assessment
After graft fixation, the tourniquet was deflated. The elbow was taken through a full range of motion.
* The
lateral pivot shift test
was performed again. There was no longer any visible or palpable subluxation of the radial head, and the clunk was abolished. The elbow felt stable through all arcs of motion and with stress.
* Passive flexion and extension, as well as pronation and supination, were assessed to ensure no impingement or restriction. The forearm was held in pronation during terminal extension to protect the graft.
Wound Closure
The common extensor origin was approximated over the graft. The subcutaneous tissues were closed with absorbable sutures, and the skin was closed with non-absorbable sutures. A sterile dressing was applied.

Figure 3: Postoperative view of the lateral elbow incision following LUCL reconstruction. The cosmetic closure is evident, and a functional hinged brace is applied for controlled rehabilitation.
Post-Operative Protocol & Rehabilitation
Rehabilitation after LUCL reconstruction is critical for successful outcomes and to protect the healing graft. The protocol is typically phased over several months.
Phase I: Immediate Post-operative (Weeks 0-2/3)
- Immobilization: The elbow is immediately placed in a hinged elbow brace in 90 degrees of flexion with the forearm in neutral or slight pronation . The brace is locked to prevent full extension and supination, typically allowing motion from 30-90 degrees of flexion. Some surgeons prefer to lock out terminal extension (e.g., allow 30-100 degrees of flexion).
- Pain Management: Opioids, NSAIDs, and acetaminophen as needed.
- Wound Care: Incision kept clean and dry. Sutures removed at 10-14 days.
-
Early Motion (supervised):
- Passive and active-assisted flexion-extension within the brace limits.
- Active wrist and hand range of motion.
- Shoulder range of motion exercises (pendulum, circumduction).
-
Precautions:
- NO active supination against resistance.
- NO valgus stress.
- NO terminal extension with supination.
- Avoid lifting, pushing, or pulling.
Phase II: Early Motion and Light Strengthening (Weeks 3-6)
- Brace Adjustment: Gradual increase in range of motion of the brace, typically allowing full flexion but still blocking terminal extension and supination. For example, allowing 15-120 degrees of flexion. The forearm pronation restriction is maintained.
-
Physical Therapy:
- Continue passive and active-assisted elbow flexion-extension.
- Gentle active supination and pronation, with emphasis on pronation.
- Initiate isometric strengthening for biceps and triceps.
- Begin light isometric wrist flexion/extension.
- Precautions: Continue avoiding terminal extension with supination and valgus stress. No heavy lifting.
Phase III: Progressive Strengthening (Weeks 6-12)
- Brace Weaning: Gradually discontinue brace use as comfort and stability improve, typically around 6-8 weeks. Full elbow range of motion is encouraged, but avoidance of terminal extension with combined supination and valgus stress is paramount throughout this phase.
-
Physical Therapy:
- Progress elbow and forearm strengthening with light resistance (e.g., elastic bands, light weights). Focus on pronator and flexor muscle groups.
- Initiate rotator cuff strengthening.
- Begin proprioceptive exercises.
- Precautions: No forceful supination, heavy lifting, or impact activities.
Phase IV: Advanced Strengthening and Return to Activity (Months 3-6+)
- Continue Strengthening: Progressive resistance exercises for all upper extremity muscle groups. Incorporate functional tasks specific to patient's occupation or sport.
- Sport-Specific Training: For athletes, begin gradual return to sport-specific drills, starting with low-impact activities and progressing to full activity. This includes controlled throwing programs for overhead athletes.
- Return to Work: Gradual return to light duty, progressing to full duties based on strength and stability.
- Full Return to Unrestricted Activity: Typically around 6-9 months post-surgery, depending on individual progress and demands. This timeframe allows for complete graft maturation and remodeling.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- High Index of Suspicion: Always consider PLRI in patients with chronic lateral elbow pain and subjective instability, especially following a FOOSH injury or prior elbow surgery. It is frequently misdiagnosed as lateral epicondylitis.
- Thorough Clinical Examination: The Lateral Pivot Shift Test (external rotation recurvatum test) and the Chair Push-up Test are the most sensitive clinical tests. A positive dynamic test is the cornerstone of diagnosis.
- Dynamic Imaging is Key: While MRI is excellent for anatomical delineation of the LUCL tear, stress fluoroscopy is invaluable for confirming the dynamic subluxation pattern, which cannot be fully appreciated on static imaging. This confirms the functional instability.
- Anatomic Reconstruction: Success hinges on restoring the anatomical attachments of the LUCL. The isometric point on the lateral epicondyle is slightly anterior and superior to the center of capitellar rotation. The ulnar attachment is on the supinator crest. Recreate this trajectory faithfully.
- Forearm Pronation During Reconstruction: Graft tensioning and fixation should be performed with the elbow at 30-45 degrees of flexion and the forearm in full pronation . This position closes the posterolateral joint, reducing the subluxation and allowing for proper graft tensioning, avoiding overtensioning or undertensioning.
- Protection in Pronation Post-Op: The reconstructed LUCL must be protected from supination and valgus stress during rehabilitation, particularly in early extension. Immobilization in pronation or neutral and a hinged brace preventing full extension and supination is critical for graft healing and maturation.
Pitfalls
- Misdiagnosis: The most common pitfall is mistaking PLRI for lateral epicondylitis, leading to inappropriate and ineffective treatment. Always rule out instability in chronic lateral elbow pain.
- Inadequate Surgical Exposure: Failure to adequately identify the torn LUCL remnants and clear the anatomical attachment sites can lead to a suboptimal repair or reconstruction.
- Non-Isometric Graft Placement: Placing the graft non-isometrically can lead to graft laxity in some parts of the range of motion or graft impingement/overtensioning in others, ultimately resulting in failure of reconstruction or restricted motion.
- Overtensioning of Graft: Excessive tension can lead to stiffness, restricted motion (especially flexion), and potential iatrogenic compartment syndrome, particularly if the posterior interosseous nerve is compressed.
- Undertensioning of Graft: Insufficient tension will lead to persistent instability and recurrence of symptoms.
- Iatrogenic Nerve Injury: The posterior interosseous nerve (PIN) is at risk during the lateral approach, especially if dissection is carried too far distally or if excessive retraction is used in the supinator muscle. Constant awareness of its course is vital.
- Failure to Address Concomitant Pathology: Overlooking associated injuries, such as radial head fractures (in acute settings) or capitellar osteochondral lesions, can compromise the outcome.
- Non-Compliance with Rehabilitation Protocol: Premature or aggressive range of motion, particularly into supination and extension, or failure to protect the graft, can lead to graft failure or recurrent instability. Patient education on these restrictions is paramount.
- Incomplete Capsular Release: In chronic cases with significant scarring, a limited posterior capsular release may be necessary to restore full flexion-extension without undue tension on the graft, while preserving anterior capsule integrity. However, extensive capsular release should be avoided as it can destabilize the joint further.
Clinical & Radiographic Imaging
You Might Also Like