Elbow Calcific Tendonitis: Comprehensive Diagnosis, Clinical Presentation & Phases

Key Takeaway
Elbow calcific tendonitis is diagnosed by evaluating severe, localized pain, often disproportionate to trauma, with activity or at rest. Key findings include pinpoint tenderness over specific elbow tendons (e.g., triceps, epicondyles) during clinical examination. Understanding the distinct phases, especially the acute resorptive phase, is crucial, as it typically correlates with the most intense symptoms and guides diagnostic imaging.
Patient Presentation & History
Calcific tendonitis, while most commonly affecting the rotator cuff, can manifest in various tendons around the elbow, presenting a diagnostic challenge due to its relative infrequency compared to other elbow pathologies. Typically, patients present with acute or subacute onset of severe, localized pain, often disproportionate to any preceding trauma. The pain is usually activity-related but can become constant and disturb sleep, especially during the acute resorptive phase.
Demographics often reveal individuals between 30 and 60 years of age, though it can occur at any age. There is no strong gender predilection. Unlike traumatic injuries, there is no specific mechanism of injury; rather, it's an idiopathic process of calcium hydroxyapatite crystal deposition. Patients may report a sudden worsening of chronic, mild elbow discomfort or a de novo, excruciating pain episode. A history of previous episodes in the same or contralateral elbow, or in other joints (e.g., shoulder), should be inquired about.
Comorbidities typically are not directly linked to the etiology of calcific tendonitis, which is largely idiopathic. However, systemic conditions such as diabetes mellitus, thyroid disorders (hypothyroidism), and chronic kidney disease have been anecdotally associated with an increased incidence or more recalcitrant cases. A thorough review of systems is pertinent to rule out inflammatory arthropathies or crystalline deposition diseases (e.g., gout, pseudogout) that might mimic or co-exist with calcific tendonitis. Occupational history involving repetitive elbow movements or strenuous activity may be a contributing factor to the underlying tendinopathy but not directly to the calcification process itself.
The patient's history should detail:
*
Onset and Duration:
Acute vs. insidious, specific date if possible.
*
Character of Pain:
Sharp, aching, burning, throbbing; severity (VAS score).
*
Location:
Precise localization by the patient (e.g., lateral epicondyle, medial epicondyle, olecranon, antecubital fossa).
*
Aggravating/Alleviating Factors:
Movements, rest, medications, heat/cold.
*
Associated Symptoms:
Swelling, warmth, redness, stiffness, weakness, paresthesias.
*
Prior Treatment:
Any non-operative measures attempted (NSAIDs, physical therapy, injections) and their efficacy.
*
Functional Impact:
Limitations in ADLs, work, and recreational activities.
Specific to the elbow, calcifications can occur in:
1.
Triceps tendon:
Typically at the olecranon insertion, mimicking olecranon bursitis or triceps tendinopathy.
2.
Common extensor origin:
Mimicking lateral epicondylitis.
3.
Common flexor origin:
Mimicking medial epicondylitis.
4.
Biceps tendon:
Rarely, at its radial tuberosity insertion or even proximally.
5.
Brachialis muscle/tendon:
Less common, can cause anterior elbow pain.
The "phases" of calcific tendonitis are crucial to understanding the clinical presentation:
*
Pre-calcific Phase:
Asymptomatic. Metaplastic changes in tenocytes leading to chondrocyte transformation.
*
Formative Phase:
Calcium deposition begins. May be asymptomatic or cause mild, chronic ache due to local tissue irritation. Deposits appear dense and homogeneous on imaging.
*
Resorptive Phase:
Spontaneous resorption of calcium, often mediated by phagocytic activity. This is the most symptomatic phase, characterized by severe, acute pain, inflammation, and local swelling. Deposits on imaging may appear amorphous and ill-defined.
*
Post-calcific Phase:
Absence of calcium deposits. Tendon healing, potentially with residual scarring. Pain usually resolves.
Understanding these phases guides both diagnostic interpretation and management strategy. The acute, severe pain typically aligns with the resorptive phase, demanding prompt pain control.
Clinical Examination
A systematic and thorough clinical examination is paramount in localizing the pathology and differentiating calcific tendonitis from other potential causes of elbow pain.
Inspection
- Skin: Assess for erythema, warmth, or swelling, which can be prominent during an acute resorptive phase, especially with superficial deposits (e.g., near olecranon or epicondyles).
- Deformity: Look for any gross deformity, although typically absent in calcific tendonitis.
- Muscle Atrophy: Chronic pain and disuse can lead to mild muscle atrophy in the forearm or arm.
Palpation
-
Localized Tenderness:
This is a hallmark finding. The exact point of maximal tenderness directly over the calcific deposit is crucial. Palpate systematically around the entire elbow joint:
- Lateral Epicondyle: Common extensor origin (extensor carpi radialis brevis, extensor digitorum).
- Medial Epicondyle: Common flexor origin (pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, flexor carpi ulnaris).
- Olecranon: Triceps tendon insertion. Palpate superiorly along the triceps aponeurosis.
- Anterior Elbow: Biceps tendon insertion (radial tuberosity), brachialis muscle/tendon.
- Swelling/Induration: Localized soft tissue swelling or a palpable mass may be present, particularly during an acute inflammatory phase, suggesting a superficial deposit.
- Crepitus: Rarely, fine crepitus might be appreciated with movement if the deposit is large and superficial.
Range of Motion (ROM)
- Active and Passive ROM: Assess flexion, extension, pronation, and supination.
- Painful Arc: Patients may demonstrate a painful arc during specific movements that load the affected tendon. For instance, triceps tendon calcification would likely cause pain with resisted elbow extension. Extensor origin calcification would cause pain with resisted wrist extension and supination, and passive wrist flexion with the elbow extended. Flexor origin calcification would cause pain with resisted wrist flexion and pronation, and passive wrist extension with the elbow extended.
- Limitations: Significant ROM limitation is uncommon unless the calcification is very large, impinges on the joint, or there is significant pain-induced guarding. Pain typically limits the end ranges of motion.
Neurological & Vascular Assessment
- Neurological: Perform a complete neurological examination of the upper extremity, assessing motor strength, sensation (light touch, pinprick), and deep tendon reflexes (biceps, brachioradialis, triceps). This is vital to rule out nerve entrapment syndromes (e.g., radial tunnel syndrome mimicking lateral epicondylitis, cubital tunnel syndrome mimicking medial epicondylitis, median nerve entrapment). Pain from calcific tendonitis is typically localized and does not follow a dermatomal or peripheral nerve distribution unless secondary nerve irritation occurs.
- Vascular: Palpate radial and ulnar pulses. Assess capillary refill. Vascular compromise is not expected in calcific tendonitis.
Special Tests
While not specific for calcific tendonitis, provocation tests for epicondylitis can be positive if the calcification is within the common extensor or flexor origins (e.g., Cozen's test, Maudsley's test for lateral epicondylitis; Golfer's elbow test for medial epicondylitis). These tests help localize the involved tendon.
Imaging & Diagnostics
Imaging is crucial for confirming the diagnosis of calcific tendonitis, localizing the deposits, assessing their morphology, and ruling out other pathologies.
X-ray Findings
- Modality of Choice: Plain radiographs (AP, lateral, oblique views of the elbow) are the initial and often definitive diagnostic tool.
- Findings: They will demonstrate areas of radiodensity (calcification) within the soft tissues adjacent to the bone, specifically in the suspected tendon.
-
Characteristics:
- Location: Crucial for correlating with clinical findings (e.g., triceps insertion on olecranon, common extensor/flexor origins on epicondyles).
- Size and Shape: Can vary from small, punctate deposits to large, amorphous collections.
-
Morphology (Phases):
- Formative Phase: Typically well-defined, dense, homogeneous, and discrete calcifications.
- Resorptive Phase: Often ill-defined, fluffy, hazy, and amorphous, indicating active calcium resorption and inflammation. This phase correlates with acute, severe pain.
- Dynamic Imaging: Repeat radiographs over time can show progression, regression, or changes in morphology, correlating with the phases of the condition.
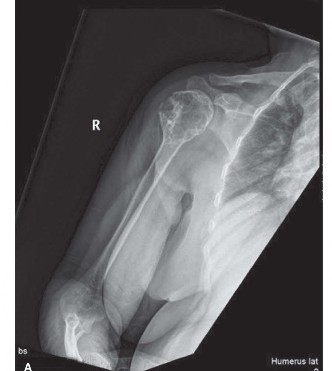
Figure 1: Plain radiograph demonstrating calcific deposits adjacent to the olecranon, consistent with triceps tendon calcific tendonitis.
Ultrasound (US)
- Role: Excellent for dynamic assessment, localization, guiding interventions, and evaluating soft tissue changes.
-
Findings:
- Calcific Deposits: Highly echogenic foci with posterior acoustic shadowing within the tendon.
- Tendon Changes: Thickening, loss of normal fibrillar pattern, hypoechogenicity indicative of tendinosis.
- Inflammation: Peritendinous fluid, hyperemia on Doppler imaging (especially in the resorptive phase).
- Dynamic Assessment: Can assess tendon integrity and movement relative to adjacent structures.
- Interventional Guidance: US is invaluable for guiding corticosteroid injections, needling, and barbotage procedures directly into or around the calcific deposit.
Magnetic Resonance Imaging (MRI)
- Indications: Typically reserved for cases where the diagnosis is uncertain, to rule out other pathologies (e.g., partial tendon tears, nerve entrapment, osteochondral lesions, inflammatory arthritis), or when symptoms are recalcitrant.
-
Findings:
- Calcific Deposits: Appear as areas of low signal intensity on all sequences (due to lack of mobile protons).
- Inflammation: High signal intensity on T2-weighted and STIR sequences within and surrounding the tendon, indicating edema and inflammation, particularly prominent during the resorptive phase.
- Tendon Integrity: Evaluates for associated tendinosis or full-thickness tears (though less common with calcific tendonitis).
- Adjacent Structures: Assesses for bursitis, nerve impingement, or joint effusions.
- Limitations: While useful for soft tissue assessment, MRI is less sensitive than X-ray for detecting small calcifications and can sometimes overestimate the size of inflammatory changes relative to the actual calcium deposit.
Computed Tomography (CT)
- Indications: Rarely indicated for routine diagnosis of calcific tendonitis. May be useful in cases of complex anatomy, atypical locations, or if surgical planning requires precise 3D localization of very large, intra-articular, or juxta-articular deposits that might be causing impingement. It offers superior bone detail and precise localization of calcium.
Laboratory Investigations
- Routine blood tests: Not typically required.
- Specific blood tests: If there is suspicion of underlying systemic disease (e.g., rheumatological conditions like gout or pseudogout, thyroid dysfunction, diabetes), then ESR, CRP, uric acid, thyroid stimulating hormone (TSH), and blood glucose levels may be warranted. Synovial fluid aspiration and analysis for crystals may be indicated if there is suspicion of inflammatory arthritis or septic joint.
Differential Diagnosis
The presentation of elbow pain, especially acute and severe, necessitates a broad differential diagnosis to ensure accurate management. Calcific tendonitis must be distinguished from other common and uncommon pathologies of the elbow.
| Feature / Condition | Calcific Tendonitis (Elbow) | Lateral Epicondylitis ("Tennis Elbow") | Medial Epicondylitis ("Golfer's Elbow") | Olecranon Bursitis | Septic Arthritis / Gouty Arthritis | Nerve Entrapment Syndrome |
|---|---|---|---|---|---|---|
| Etiology | Idiopathic hydroxyapatite deposition; metabolic factors. | Overuse/microtrauma of common extensor origin. | Overuse/microtrauma of common flexor origin. | Trauma, repetitive friction, infection, inflammation. | Bacterial infection (septic); Uric acid crystals (gout). | Compression of radial, ulnar, or median nerves. |
| Pain Onset | Acute/subacute (resorptive phase); insidious (formative). | Gradual, insidious. | Gradual, insidious. | Acute (septic, traumatic) or insidious (chronic). | Acute, severe. | Gradual, intermittent. |
| Pain Character | Severe, sharp, localized, often constant (resorptive). | Dull ache, burning, worse with grip/wrist extension. | Dull ache, burning, worse with grip/wrist flexion. | Aching, tenderness with swelling. | Excruciating, throbbing, constant. | Numbness, tingling, burning, shooting; weakness. |
| Pain Location | Localized to calcific deposit (e.g., triceps, epicondyle). | Lateral epicondyle, radiating to forearm. | Medial epicondyle, radiating to forearm. | Posterior elbow over olecranon. | Diffuse joint pain, periarticular (gout). | Dependent on nerve: radial tunnel, cubital tunnel, pronator. |
| Swelling/Erythema | Localized, sometimes pronounced during resorptive phase. | Mild or absent. | Mild or absent. | Prominent swelling over olecranon, +/- erythema (septic). | Marked swelling, erythema, warmth. | Absent. |
| ROM | Painful arc, end-range pain, mild limitation (pain-driven). | Painful with resisted wrist extension/supination. | Painful with resisted wrist flexion/pronation. | Full, but painful if bursa distended. | Markedly limited and painful. | Full, but specific movements may provoke symptoms. |
| Palpation | Exquisite tenderness directly over calcification. | Tenderness at common extensor origin. | Tenderness at common flexor origin. | Fluctuant swelling, tenderness over olecranon. | Diffuse tenderness, warmth, induration. | Tenderness over nerve entrapment site (e.g., cubital tunnel). |
| Radiographs | Pathognomonic calcific deposit. | Usually normal (unless chronic enthesopathy). | Usually normal. | May show soft tissue swelling; possible bone spur. | Joint effusion; periarticular erosions (chronic gout). | Normal. |
| Ultrasound | Highly echogenic deposit with shadowing; tendon changes. | Tendon thickening, hypoechogenicity, neo-vascularity. | Tendon thickening, hypoechogenicity, neo-vascularity. | Fluid collection within bursa; synovial proliferation. | Effusion; synovial thickening; possible crystal detection. | Nerve swelling/compression. |
| MRI | Low signal deposit; T2 high signal in surrounding tissue. | Tendinosis, possible partial tears, bone marrow edema. | Tendinosis, possible partial tears, bone marrow edema. | Bursa fluid, synovial thickening. | Synovitis, effusion, bone edema, cartilage loss. | Nerve edema, signal change, muscle denervation edema. |
| Labs | Usually normal; check for metabolic causes if suspected. | Normal. | Normal. | Normal (unless septic: ↑WBC, ESR, CRP). | ↑WBC, ESR, CRP, Uric Acid (gout). Joint aspiration crucial. | Normal. |
Surgical Decision Making & Classification
The decision-making process for calcific tendonitis of the elbow primarily revolves around the severity of symptoms, the phase of the disease, and the response to non-operative management. Operative intervention is typically reserved for refractory cases. There isn't a specific "classification" system for elbow calcific tendonitis that dictates surgical approach, unlike fracture classifications. Instead, decision-making is guided by the patient's clinical picture and the calcification's characteristics.
Non-Operative vs. Operative Decision
The overwhelming majority of elbow calcific tendonitis cases resolve with non-operative management, especially given the self-limiting nature of the resorptive phase.
Indications for Non-Operative Management (First-Line):
*
Acute Pain (Resorptive Phase):
Initial management focuses on pain control and facilitating calcium resorption.
*
Mild to Moderate Chronic Pain (Formative Phase):
When functional limitation is not severe.
*
No Mechanical Impingement:
Calcifications not causing impingement on neural or vascular structures or joint mechanics.
*
Absence of Tendon Rupture:
Calcifications rarely cause tendon rupture, but this would be a contraindication to solely conservative management.
Non-Operative Modalities:
1.
Rest and Activity Modification:
Avoiding aggravating activities.
2.
Pharmacotherapy:
*
NSAIDs:
Oral or topical, for pain and inflammation, particularly in the acute resorptive phase.
*
Analgesics:
Acetaminophen or stronger opioids for severe pain.
3.
Physical Therapy:
*
Modalities:
Ice, heat, ultrasound, phonophoresis, iontophoresis.
*
Exercises:
Gentle range of motion, stretching, and strengthening (once acute pain subsides) to maintain function and prevent stiffness.
4.
Corticosteroid Injections:
*
Mechanism:
Potent anti-inflammatory effect.
*
Technique:
Ultrasound-guided injection of corticosteroid and local anesthetic into the peritendinous space adjacent to the calcification. Direct intratendinous injection should be avoided due to risk of tendon weakening.
*
Efficacy:
Can provide significant short-term pain relief, particularly in the acute inflammatory phase. Repeat injections should be limited.
5.
Extracorporeal Shockwave Therapy (ESWT):
*
Mechanism:
High-energy sound waves are thought to induce microtrauma, stimulate healing, and potentially aid in calcium resorption by increasing vascularity and modulating inflammatory response.
*
Evidence:
Mixed, but some studies show efficacy, particularly for chronic, recalcitrant cases.
*
Protocol:
Typically 3-5 sessions, high or low energy.
6.
Ultrasound-Guided Barbotage (Needling and Lavage):
*
Mechanism:
A needle is used under ultrasound guidance to aspirate, fragment, and lavage the calcium deposits. Local anesthetic and often corticosteroid are then injected.
*
Efficacy:
Highly effective for acute, subacute, and even chronic calcifications, particularly in the resorptive phase where deposits are often amorphous and easily disrupted.
*
Advantages:
Minimally invasive, performed in an outpatient setting, often provides rapid pain relief.
Indications for Operative Management (Second-Line):
Surgical intervention is considered when conservative measures have failed for at least 6-12 months, and the patient continues to experience debilitating pain and functional impairment.
*
Persistent Severe Pain:
Unresponsive to comprehensive non-operative treatment.
*
Large, Recalcitrant Calcifications:
Particularly those causing mechanical impingement or hindering tendon function.
*
Diagnosis of Exclusion:
When other significant pathologies have been ruled out.
*
Acute Flare-ups:
Extremely rare for operative management, as the resorptive phase usually resolves spontaneously or responds to non-operative interventions.
Pre-Operative Planning:
*
Imaging:
Detailed radiographs and ultrasound are essential. MRI may be used to assess tendon integrity and rule out other pathologies.
*
Patient Education:
Discuss potential benefits, risks (infection, nerve injury, persistent pain, stiffness), and expected recovery.
*
Anesthesia:
Regional block (e.g., supraclavicular or interscalene block) combined with general anesthesia is often preferred for optimal post-operative pain control.
Surgical Technique / Intervention
For the rare cases of elbow calcific tendonitis refractory to non-operative management, surgical excision of the calcific deposit is indicated. This can be performed via open or arthroscopic approaches, depending on the location and size of the deposit, surgeon preference, and associated pathology.
Patient Positioning
- Triceps Tendon: Patient is typically positioned prone with the arm draped free and supported on a hand table, or lateral decubitus. A tourniquet is applied high on the arm.
- Epicondylar Regions (Lateral/Medial): Supine position with the arm abducted on a hand table or in a dedicated arm holder, allowing for elbow flexion/extension and pronation/supination. Tourniquet application is standard.
- Biceps Tendon: Supine, arm abducted on a hand table.
Surgical Approach
The choice of approach is dictated by the precise anatomical location of the calcific deposit.
-
Triceps Tendon Calcification (Open Excision):
- Incision: A posterior longitudinal incision centered over the olecranon, extending proximally along the triceps aponeurosis.
- Dissection: Careful dissection through subcutaneous tissue, identifying and protecting the ulnar nerve proximally if it crosses the field. The triceps tendon is exposed.
- Identification: The calcific deposit is typically visible as a hard, whitish-yellow mass within the tendon. Palpation can confirm its exact location. Ultrasound can be used intraoperatively for precise localization if needed.
- Excision: A longitudinal incision is made directly over the calcification within the triceps tendon fibers. The calcific material is carefully curetted and excised using small osteotomes, curettes, or suction. It is crucial to remove all visible calcium while preserving as much healthy tendon tissue as possible. The wound is copiously irrigated.
- Closure: The tendon incision is closed with absorbable sutures if significant defect is created, or left open if small. Subcutaneous layers and skin are closed.
-
Common Extensor/Flexor Origin Calcification (Open Excision):
- Lateral Epicondyle: A small longitudinal or oblique incision centered over the lateral epicondyle. Dissection through subcutaneous tissue. The common extensor origin is identified. A small incision is made in the ECRB tendon fibers. The calcification is identified and meticulously debrided.
- Medial Epicondyle: A small longitudinal incision centered over the medial epicondyle. Careful identification and protection of the ulnar nerve (subcutaneous or subfascial) are paramount. The common flexor origin is identified and incised to remove the calcification.
- Considerations: Given the common coexistence of tendinosis, concomitant debridement of degenerative tendon tissue (decortication or drilling of the epicondyle) may be considered, similar to standard epicondylitis surgery, but this is secondary to calcification removal.
-
Arthroscopic Excision (Less Common for Elbow Calcific Tendonitis):
- Indications: Can be considered for intra-articular or juxta-articular deposits that are accessible arthroscopically and cause impingement, or when concurrent intra-articular pathology requires attention. This approach is more technically demanding for calcific deposits within the substance of the tendon.
- Portals: Standard elbow arthroscopy portals (e.g., anteromedial, anterolateral, posterolateral, direct posterior) are used, tailored to the location.
- Technique: The joint is distended, and diagnostic arthroscopy is performed. The calcific deposit is localized. Using shavers, burrs, or curettes, the deposit is carefully debrided. Copious irrigation is critical to remove all calcium debris.
- Advantages: Minimally invasive, potentially faster recovery.
- Disadvantages: Risk of nerve/vascular injury, incomplete removal if deposit is deep within tendon.
Fixation Construct
No fixation construct is required as calcific tendonitis excision involves debridement of ectopic calcium, not tendon repair or osteosynthesis. If extensive debridement creates a large tendon defect, a primary repair of the tendon edges using non-absorbable sutures may be performed to restore tendon continuity, especially in the triceps. However, this is uncommon.
Reduction Techniques
No reduction techniques are involved as this is soft tissue debridement, not a fracture or dislocation.
Post-Operative Protocol & Rehabilitation
Post-operative management aims to minimize pain, protect the healing tendon, and restore full elbow function. The protocol is typically less stringent than for tendon repairs but requires careful progression.
Immediate Post-Operative (Day 0-7)
- Pain Management: Oral analgesics (NSAIDs, acetaminophen, opioids as needed). Regional blocks provide excellent initial pain control.
-
Immobilization:
- Open Excision: Often a soft compressive dressing for comfort. For triceps tendon, a removable posterior splint or hinged elbow brace may be used for 1-2 weeks in slight flexion (30-45 degrees) to protect the repair if the tendon was incised significantly.
- Arthroscopic Excision: Soft dressing, early gentle motion.
- Elevation: To reduce swelling.
- Ice: Regular application to the surgical site.
- Gentle Active Range of Motion (AROM): Begin very gentle, pain-free AROM exercises of the elbow and wrist within tolerance, usually starting by day 1-3, under guidance from a therapist.
- Wound Care: Keep incision clean and dry. Monitor for signs of infection.
Early Rehabilitation (Weeks 1-6)
- Focus: Gradual increase in ROM, gentle strengthening, scar management.
-
Physical Therapy:
Initiated early.
- ROM: Progress full passive and active elbow flexion/extension, pronation/supination. Avoid aggressive stretching initially.
- Gentle Isometrics: Start with very light, pain-free isometric exercises for the affected muscle groups (e.g., triceps, wrist extensors/flexors) to maintain muscle tone.
- Scar Mobilization: Gentle massage around the incision once healed to prevent adhesion formation.
- Activity Restrictions: Avoid heavy lifting, pushing, pulling, or repetitive activities that load the surgically treated tendon. No driving if still on opioids or if the dominant arm is affected and mobility is limited.
Intermediate Rehabilitation (Weeks 6-12)
- Focus: Progressive strengthening, endurance, and return to functional activities.
-
Physical Therapy:
- Progressive Resistance Exercises: Gradual increase in resistance for isotonic and isokinetic exercises targeting the entire upper extremity.
- Proprioception and Neuromuscular Control: Exercises to improve coordination and joint stability.
- Functional Training: Incorporate activities that mimic daily tasks and work/sport-specific movements.
- Return to Activity: Gradually reintroduce light recreational activities. Avoid activities that cause pain.
Advanced Rehabilitation & Return to Sport/Work (Weeks 12+)
- Focus: Maximizing strength, power, and endurance; sport/work-specific training.
- Physical Therapy: Advanced strengthening, plyometrics, and agility drills if applicable.
- Gradual Return to Sport/Work: A structured, progressive return to full activity is crucial. This is highly individualized and depends on the specific demands of the sport or occupation.
- Patient Education: Emphasize the importance of warm-up, cool-down, proper technique, and listening to their body to prevent recurrence or new injuries.
Key Considerations:
*
Individualized Protocol:
Rehabilitation must be tailored to the patient's individual progress, pain levels, and the specific tendon involved.
*
Pain-Limited Progression:
Pain should always be the guiding factor for progression. Pushing through significant pain can lead to setbacks.
*
Compliance:
Patient adherence to the rehabilitation program is critical for optimal outcomes.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls
- X-ray is Diagnostic: For calcific tendonitis, plain radiographs are the initial and often definitive imaging modality. A well-localized calcification on X-ray correlating with clinical tenderness is usually sufficient for diagnosis.
- Acute Pain = Resorptive Phase: Severe, acute onset pain typically signifies the resorptive phase, which is generally self-limiting and highly responsive to conservative management, particularly NSAIDs and corticosteroid injections (often ultrasound-guided).
- Ultrasound for Localization & Intervention: Ultrasound is invaluable for precise localization of calcific deposits, assessing their inflammatory activity (Doppler signal), and guiding injections or barbotage (needling and lavage). Barbotage is highly effective and minimally invasive.
- Elbow-Specific Locations: Remember triceps tendon at the olecranon is a common elbow site, often mistaken for olecranon bursitis or simple triceps tendinopathy. Also consider common extensor/flexor origins.
- Conservative Management First: Over 90% of cases respond to non-operative treatment. Surgical intervention is a last resort for chronic, refractory cases.
- Thorough Differential: Always consider other common elbow pathologies, especially nerve entrapment, epicondylitis, and inflammatory/crystalline arthropathies, as their management differs significantly.
- Patient Education: Explain the idiopathic nature and self-limiting course of the condition to manage patient expectations regarding symptom duration and potential for resolution.
- Phases of Calcific Tendonitis: Understand the formative and resorptive phases, as they dictate clinical presentation, imaging characteristics, and treatment strategies. Formative calcifications are typically dense and well-defined; resorptive calcifications are fluffy and ill-defined.
Pitfalls
- Misdiagnosis of Olecranon Bursitis: Triceps calcific tendonitis can present with posterior elbow pain and swelling, mimicking olecranon bursitis. X-rays are crucial to differentiate. Bursitis fluid can be drained, calcific tendonitis cannot.
- Over-reliance on MRI: While useful for soft tissue assessment and ruling out other pathology, MRI is less sensitive for detecting subtle calcifications than X-ray and can overestimate inflammatory changes. It's an adjunctive, not primary, diagnostic tool for calcific tendonitis.
- Premature Surgical Intervention: Operating too early for calcific tendonitis is a pitfall. The condition often resolves spontaneously or with simple interventions. A minimum of 6-12 months of failed comprehensive conservative management should typically precede surgical consideration.
- Incomplete Calcium Removal: During surgery, failure to remove all calcific material, especially if deeply embedded or widely dispersed, can lead to persistent symptoms. Intraoperative fluoroscopy or ultrasound can aid in confirming complete removal.
- Tendon Damage During Injection: Direct intratendinous injection of corticosteroids can weaken the tendon and increase the risk of rupture. Peritendinous injection, guided by ultrasound, is the safer and more effective approach.
- Ignoring Underlying Metabolic Conditions: While largely idiopathic, neglecting to screen for metabolic conditions (e.g., diabetes, hypothyroidism) in recurrent or atypical cases can be a pitfall, as addressing these may influence prognosis.
- Nerve Injury During Surgery: Particularly around the medial epicondyle (ulnar nerve) or lateral epicondyle (radial nerve branches), meticulous dissection is required to avoid iatrogenic nerve injury during open excision.
- Post-Operative Stiffness: While rare, aggressive early rehabilitation after extensive debridement or if significant tendinopathy was also addressed can lead to scar formation and stiffness. A balanced approach to early motion and protection is key.
You Might Also Like