Pediatric Distal Radius Salter-Harris Type II Fracture: Diagnosis & Management Case Study

Key Takeaway
A pediatric Salter-Harris Type II distal radius fracture involves the distal radius metaphysis extending through the physis, often from a FOOSH injury. Diagnosis includes clinical examination for "dinner fork" deformity and localized tenderness, confirmed by PA, lateral, and oblique X-rays revealing the metaphyseal and physeal components, often with a "Thurston Holland fragment."
Patient Presentation & History
A 10-year-old right-hand dominant male presented to the emergency department after sustaining a fall during a soccer game. The mechanism of injury involved a direct impact to the wrist followed by a fall onto an outstretched hand (FOOSH) as he attempted to brace himself. He reported immediate, severe pain and deformity of the left wrist. There was no direct head trauma or loss of consciousness.
His past medical history is unremarkable, with no known allergies or previous fractures. He is pre-pubertal, with no diagnosed skeletal dysplasias or metabolic bone conditions. The patient's parents report that he is active in multiple sports.
Clinical Examination
Upon initial assessment, the patient was in acute distress due complaining of severe pain in his left wrist.
- Inspection: Gross deformity of the distal forearm and wrist was evident, consistent with an apex volar angulation and dorsal displacement of the distal fragment, often described as a "dinner fork" deformity. Significant swelling was observed circumferentially around the wrist and distal forearm. No open wounds, skin tenting, or signs of impending compartment syndrome were appreciated at this initial presentation.
- Palpation: Diffuse tenderness was elicited over the entire distal radius and ulna, maximal at the distal radial metaphysis and physis. Palpation of the distal ulna revealed minimal tenderness, suggesting involvement primarily of the radius. No crepitus was noted with gentle manipulation. The ulnar styloid was non-tender.
- Range of Motion (ROM): All active and passive wrist ROM (flexion, extension, radial/ulnar deviation, pronation, supination) was severely limited due to pain and guarding.
- Neurological Assessment: Sensation to light touch was intact in the median, ulnar, and radial nerve distributions. Motor function of the intrinsic hand muscles and extrinsic digital flexors/extensors was grossly intact, although limited by pain.
- Vascular Assessment: Radial and ulnar pulses were strong and symmetric bilaterally. Capillary refill was brisk (<2 seconds) in all digits. No pallor or paresthesias were reported.
Imaging & Diagnostics
Initial radiographic evaluation of the left wrist included standard posteroanterior (PA), lateral, and oblique views.
-
X-ray Findings:
-
PA View:
Demonstrated a transverse fracture line through the distal metaphysis of the radius, extending proximally from the radial cortex and exiting through the physis on the ulnar side. This pattern is consistent with a Salter-Harris Type II fracture of the distal radius. There was significant dorsal displacement of the distal fragment relative to the metaphysis.
-
Lateral View:
Confirmed the Salter-Harris Type II fracture with marked dorsal displacement and apex volar angulation of approximately 35 degrees. There was significant overriding of the fracture fragments, with approximately 75% dorsal cortical translation. The distal radio-ulnar joint (DRUJ) appeared congruent, with no evidence of associated ulnar shaft fracture.

- Oblique View: Further delineated the metaphyseal component and confirmed the physeal extension, highlighting the "Thurston Holland fragment" (a triangular metaphyseal fragment on the compression side, pathognomonic for Salter-Harris Type II).
- No obvious associated carpal fractures or acute ligamentous injuries were identified on these initial views. The growth plate of the distal ulna appeared intact.
-
PA View:
Demonstrated a transverse fracture line through the distal metaphysis of the radius, extending proximally from the radial cortex and exiting through the physis on the ulnar side. This pattern is consistent with a Salter-Harris Type II fracture of the distal radius. There was significant dorsal displacement of the distal fragment relative to the metaphysis.
-
CT/MRI Indications: For typical, non-comminuted pediatric distal radius physeal fractures, CT or MRI is generally not indicated. However, specific indications include:
- CT: Suspected intra-articular extension in Salter-Harris Type III or IV injuries, significant comminution precluding adequate assessment on plain films, evaluation of irreducible fractures, or planning for complex open reduction. In this specific case, the plain radiographs clearly defined the fracture pattern, making CT unnecessary.
- MRI: Rarely indicated in acute settings, but can be useful for evaluating soft tissue injuries (ligamentous, TFCC in adolescents), suspected avascular necrosis (late presentation), or subtle physeal bar formation in cases of growth arrest.
-
Templating: Pre-operative templating is not typically performed for routine pediatric distal radius fractures managed by closed reduction and percutaneous pinning (CRPP) or casting, as implant size (K-wire diameter) is determined intraoperatively based on patient size and bone quality. For complex cases requiring open reduction and internal fixation with plates, pre-operative templating would be more relevant to determine plate length and screw positions.
Differential Diagnosis
| Feature | Distal Radius Physeal Fracture (Salter-Harris Type II) | Distal Radius Metaphyseal Fracture (Greenstick/Complete) | Carpal Bone Fracture (e.g., Scaphoid Fracture) | Galeazzi Fracture-Dislocation |
|---|---|---|---|---|
| Etiology | FOOSH, direct trauma. Physeal plate weakest link in growing bone. | FOOSH, direct trauma. Bone failure before physis. | FOOSH, hyperextension/ulnar deviation. Common in adolescents. | Direct blow to ulnar aspect of forearm, FOOSH with pronation. |
| Clinical Presentation | Localized pain, swelling, tenderness over distal radius physis. Deformity common. | Localized pain, swelling, tenderness over distal radial metaphysis. Deformity common. | Radial-sided wrist pain, snuffbox tenderness, pain with axial load of thumb. | Forearm pain, prominent ulnar head (DRUJ dislocation), limited pronation/supination. |
| Imaging | Fracture through physis and metaphyseal fragment (Thurston Holland sign). | Fracture line through metaphysis (cortex often intact on one side for greenstick). | Scaphoid views (PA, Lateral, Oblique, Scaphoid). May be occult on initial films. | Radius shaft fracture (typically distal 1/3) with DRUJ disruption. |
| Treatment Considerations | Closed reduction, casting or CRPP. Prioritize physeal alignment. Growth arrest concern. | Closed reduction, casting. Remodeling potential considered. | Thumb spica cast for 6-12 weeks. ORIF for displaced/unstable. High AVN risk. | Operative fixation of radius, DRUJ reduction, stabilization. Complex injury. |
| Prognosis | Generally excellent with good reduction. Potential for growth disturbance (rare with SH II). | Excellent with good reduction, high remodeling potential. | Variable. Nonunion, AVN risk. Long immobilization. | Good with appropriate fixation. Risk of DRUJ instability. |
Surgical Decision Making & Classification
Given the patient's age (10 years), the degree of displacement, and the significant apex volar angulation (35 degrees), operative intervention was indicated. While children have considerable remodeling potential, particularly in younger age groups and for angulation in the plane of motion, the magnitude of angulation and displacement in this case exceeded acceptable parameters for non-operative management.
Acceptable Reduction Parameters for Distal Radius Fractures in Children:
- Age < 10 years: Up to 20-25 degrees angulation, up to 100% displacement (if reducible and stable). Remodeling potential is high.
- Age > 10 years (or approaching skeletal maturity): Up to 10-15 degrees angulation, <50% displacement. Remodeling potential significantly decreases.
- Rotation: No rotational deformity is acceptable at any age, as remodeling does not correct rotation.
Our patient, at 10 years old, presented with 35 degrees of angulation and significant dorsal displacement. Although technically still young, the extent of the deformity exceeded the generally accepted limits for spontaneous remodeling, especially considering the potential for residual functional deficits and cosmetic deformity.
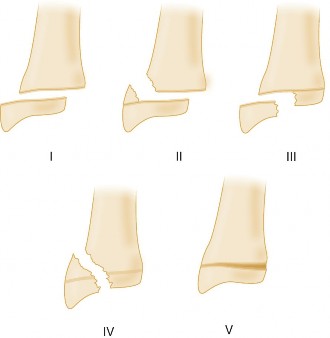
Classification:
The fracture was classified as a
Salter-Harris Type II
fracture of the distal radius. This classification system is crucial for physeal injuries:
*
Type I:
Transverse fracture through the physis, often difficult to see on X-ray.
*
Type II:
Fracture through the physis and metaphysis, leaving the epiphysis intact. Most common type.
*
Type III:
Fracture through the physis and epiphysis, extending into the joint. Requires anatomical reduction.
*
Type IV:
Fracture through the metaphysis, physis, and epiphysis, extending into the joint. Also requires anatomical reduction.
*
Type V:
Crush injury to the physis, rarely seen acutely, high risk of growth arrest.
The decision was made for closed reduction and percutaneous pinning (CRPP) . This approach allows for stable fixation while minimizing surgical morbidity, reducing the risk of iatrogenic physeal damage, and facilitating early rehabilitation compared to open techniques. The primary goal was to achieve an anatomical or near-anatomical reduction, especially correcting rotation and minimizing angulation and displacement, followed by stable K-wire fixation to maintain the reduction until healing.
Surgical Technique / Intervention
The patient was transferred to the operating room for closed reduction and percutaneous pinning.
-
Patient Positioning and Anesthesia:
- The patient was placed supine on the operating table.
- A hand table was used to support the affected limb.
- A high arm tourniquet was applied to the upper arm.
- General anesthesia was administered. A regional block (e.g., supraclavicular or axillary block) can be considered as an adjunct for post-operative pain control.
- The entire arm was prepped and draped in a sterile fashion, ensuring adequate visualization of the distal forearm and hand.
-
Closed Reduction:
- Traction and Counter-traction: Gentle traction was applied to the fingers with the elbow flexed to 90 degrees to disengage the fracture fragments and restore length. Counter-traction was applied to the upper arm.
- Manipulation: Once traction was applied, the distal fragment, which was dorsally displaced and apex volar angulated, was reduced. This involved accentuating the deformity, followed by applying dorsal pressure over the distal fragment and simultaneous volar pressure over the proximal fragment (for apex volar angulation), while concomitantly correcting any rotational deformity. Pronation and supination maneuvers were used to assess and correct rotation. The goal was to achieve an apex dorsal alignment and correction of any radial or ulnar deviation.
-
Fluoroscopic Confirmation:
Reduction was confirmed with intraoperative fluoroscopy in PA and lateral views. Adequate reduction was defined as less than 10 degrees of angulation, less than 2mm displacement, and no rotational malalignment.

-
Percutaneous Pinning:
- Once an acceptable reduction was achieved and held manually, fixation was performed using smooth, stainless steel Kirschner wires (K-wires), typically 1.6mm (0.062 inch) or 2.0mm (0.078 inch) in diameter, depending on bone size.
-
Pin Placement Strategy:
- Radial-to-Ulnar Pins (Cross-Pinning): Two K-wires were typically inserted, starting from the radial aspect of the distal radius (near the styloid) and directed across the fracture site into the proximal metaphysis/diaphysis. The pins were inserted under fluoroscopic guidance to avoid the growth plate as much as possible, though crossing the physis is sometimes unavoidable and generally well-tolerated with smooth K-wires for short durations. The entry points were carefully chosen to avoid the superficial radial nerve.
- Kapandji Technique (Intrafocal Pinning): An alternative or supplementary technique involves placing a K-wire directly into the fracture site from the dorsoradial aspect and using it as a joystick to help reduce the dorsal cortical displacement before advancing it across the fracture. This technique is often combined with a more stable cross-pin. For this case, a standard cross-pinning technique was chosen to ensure rigid fixation.
-
Pin Insertion:
- The first K-wire was inserted from the radial styloid, aiming proximally across the fracture site, ensuring good cortical purchase in the proximal fragment.
- The second K-wire was inserted from the dorsal-ulnar aspect of the distal radius, traversing the fracture site obliquely to engage the opposite cortex of the proximal fragment, creating a stable construct. This cross-pinning strategy provided good stability in both sagittal and coronal planes.
- Care was taken to ensure that the K-wires did not excessively violate the articular surface or compromise the DRUJ.
-
Fluoroscopic Verification:
Final PA and lateral fluoroscopic images confirmed satisfactory K-wire placement, fracture reduction, and stability.


- Pin Management: The K-wires were bent and cut externally, leaving enough length to be easily removed in the outpatient clinic. Pin sites were dressed with sterile gauze.
-
Immobilization:
- Following pinning, a well-padded sugar-tong splint was applied to maintain the reduction and provide additional support. This was preferred over a full cast initially to accommodate for post-operative swelling.
-
Final X-rays were taken to confirm continued good reduction and pin position after splint application.

Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Day 0-7):
- Pain Management: Oral analgesics (acetaminophen, ibuprofen, with short-term opioid if necessary) were prescribed.
- Elevation: The patient was instructed to keep the hand elevated above heart level to minimize swelling.
- Neurovascular Checks: Frequent neurovascular checks were performed to monitor for any signs of compartment syndrome or nerve compromise.
- Splint Care: The sugar-tong splint was kept dry and intact.
- Pin Site Care: Parents were instructed on basic pin site care, looking for signs of infection (redness, warmth, drainage).
Early Post-Operative Period (Weeks 1-4):
- Clinic Visit (Week 1): The patient was seen in the clinic. The sugar-tong splint was removed, skin inspected, and a short arm cast applied. The cast was applied in a neutral position (slight wrist extension, neutral forearm rotation), ensuring comfort and avoiding pressure points.
- Activity Restrictions: Patient was advised to avoid strenuous activities, contact sports, and immersing the cast in water.
- Pin Removal (Week 3-4): K-wires were typically removed in the outpatient clinic at 3-4 weeks post-operatively. For Salter-Harris Type II fractures, 3-4 weeks is often sufficient for initial bony stability while minimizing the risk of physeal irritation.
Mid-Term Post-Operative Period (Weeks 4-8):
- Cast Removal (Week 4-6): The short arm cast was typically removed at 4-6 weeks post-operatively, depending on radiographic evidence of healing.
-
Initiation of Rehabilitation:
- Passive and Active ROM: Gentle active and passive range of motion exercises for the wrist and forearm were initiated immediately after cast removal. These included wrist flexion/extension, radial/ulnar deviation, pronation/supination.
- Finger ROM: Patients were encouraged to maintain full finger ROM throughout the immobilization period.
- Light Strengthening: As pain subsided and ROM improved, light isometric strengthening exercises for the wrist flexors and extensors were introduced.
- Activity Progression: Gradual return to activities of daily living. Avoidance of heavy lifting or high-impact activities for several more weeks.
Long-Term Post-Operative Period (Months 2-6 and beyond):
- Full Return to Activity: Most children can return to full unrestricted activity, including sports, by 3-4 months post-injury, provided they have regained full range of motion, strength, and confidence.
- Follow-up: Long-term follow-up (up to 1-2 years) is crucial for pediatric physeal fractures, especially in younger children or higher-grade Salter-Harris injuries (Type III, IV, V), to monitor for potential growth disturbance (physeal arrest, angular deformity, limb length discrepancy). Regular clinical assessment and radiographs (PA and lateral views) were performed at 6-month intervals to assess for physeal bridging or angular changes.
Potential Complications:
- Loss of Reduction: Can occur if initial reduction is unstable or fixation is inadequate.
- Pin Site Infection: Localized infection at the K-wire entry sites, typically managed with oral antibiotics or, in severe cases, pin removal.
- Malunion: Persistent angulation or rotational deformity, which may require corrective osteotomy in severe cases or if it causes functional impairment.
- Growth Arrest: A potential complication of physeal fractures, particularly with Type III, IV, and V injuries, or if reduction is not anatomical. Can lead to angular deformity or limb length discrepancy.
- Re-fracture: Although less common, re-fracture can occur, especially shortly after cast removal if activity is initiated too aggressively.
- Compartment Syndrome: Rare after distal radius fractures but must always be considered, especially in high-energy trauma or during reduction maneuvers.
- Nerve Injury: Superficial radial nerve irritation from K-wires or during reduction.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Thorough Neurovascular Assessment: Always document pre- and post-reduction/fixation neurovascular status. Compartment syndrome, though rare, is a devastating complication.
- Rotation is Key: While children remodel angulation well, they do not remodel rotational deformity. Ensure anatomical or near-anatomical rotational alignment. Pronation-supination assessment is critical.
- Acceptable Reduction Parameters are Age-Dependent: Younger children have greater remodeling potential. Be more stringent with reduction goals in adolescents.
- Salter-Harris Classification: Understand the implications of each type, especially Type III and IV which require anatomical articular reduction to prevent arthritis, and Type V which has a high growth arrest risk.
- Smooth K-wires: Use smooth K-wires for physeal fixation to minimize iatrogenic growth plate damage. Removing them at 3-4 weeks for simple physeal fractures also minimizes this risk.
- Avoid DRUJ Impingement: Ensure K-wires do not cross or impinge upon the distal radio-ulnar joint, which can lead to limited forearm rotation.
- Post-Reduction Stability: Test the stability of the reduction fluoroscopically before and after pinning. If unstable after closed reduction, pinning is indicated.
- Long-Term Follow-up for Physeal Injuries: Monitor for growth disturbance, especially in younger patients or higher-grade Salter-Harris injuries, for at least 1-2 years.
Pitfalls:
- Missing Subtle Injuries: Overlooking associated injuries such as carpal fractures (e.g., scaphoid in adolescents), distal ulnar physeal fractures, or DRUJ instability (rare in simple distal radius fractures, but possible).
- Inadequate Reduction: Accepting residual angulation or, critically, rotational deformity beyond acceptable parameters for the patient's age can lead to functional impairment and cosmetic deformity.
- Inadequate Fixation: Using too few pins, pins that are too small, or poorly placed pins can lead to loss of reduction and re-displacement.
- Pin Site Infection: Poor pin site care or prolonged retention of K-wires can lead to infection.
- Premature K-wire Removal: Removing pins before adequate healing has occurred can lead to re-fracture or loss of reduction.
- Iatrogenic Physeal Damage: Though rare with smooth K-wires, multiple passes or threaded pins across the physis can increase the risk of growth arrest.
- Over-reduction/Volkmann's Ischemia: Excessive force during reduction or tight casting/splinting can lead to compartment syndrome or acute carpal tunnel syndrome, particularly in highly displaced fractures. Always maintain vigilance and re-check neurovascular status.
- Failure to Counsel on Growth Arrest: Not discussing the potential (though low) risk of growth arrest with parents/guardians following a physeal injury.
Clinical & Radiographic Imaging


You Might Also Like


