Complex Revision Total Knee Arthroplasty: Addressing Instability, Loosening & Wear
Key Takeaway
A painful and failing total knee arthroplasty often stems from multiple issues. Common causes include aseptic loosening of components, significant polyethylene wear leading to osteolysis, and global ligamentous instability. Other factors like malalignment, patellofemoral issues, and component subsidence also contribute, necessitating complex revision surgery.
Patient Presentation & History
We are presenting a complex case of a 58-year-old male presenting with chronic, debilitating left knee pain, progressive instability, and recurrent effusions, 4 years following a primary total knee arthroplasty (TKA). The patient initially underwent TKA for severe tricompartmental osteoarthritis secondary to a remote history of tibial plateau fracture requiring ORIF 20 years prior. The initial TKA was performed at an outside institution using a posterior-stabilized (PS) design.
His post-operative course after the primary TKA was complicated by persistent discomfort, which was initially attributed to the normal recovery process. However, over the past two years, his pain significantly worsened, described as a dull ache at rest, intensifying with activity and weight-bearing. He reports mechanical symptoms including clunking and giving way, particularly when ambulating on uneven surfaces or descending stairs. He has experienced multiple falls due to perceived knee instability, necessitating the use of a cane for ambulation. The pain is consistently rated 7-8/10 on the Visual Analog Scale (VAS) despite regular use of NSAIDs and opioid analgesics. He reports daily swelling that temporarily improves with rest and elevation but never fully resolves. There has been no reported fever, chills, or systemic signs of infection, although he notes generalized fatigue.
His medical comorbidities include well-controlled Type 2 Diabetes Mellitus (HbA1c 6.8%), hypertension, and a body mass index (BMI) of 34 kg/m². He is an active smoker with a 30-pack-year history, though he claims to be reducing intake. Surgical history includes the aforementioned tibial plateau ORIF and primary left TKA. Allergies include penicillin. He works as an accountant, requiring prolonged sitting but also moderate ambulation. His functional limitations are severe, preventing him from performing routine activities of daily living and significantly impacting his quality of life. Previous non-operative management attempts by referring physicians included cortisone injections, aspiration of effusions (without diagnostic workup on fluid), and extensive physical therapy, all providing only transient or minimal relief.
Clinical Examination
On general inspection, the patient ambulates with a significant antalgic gait, exhibiting a noticeable varus thrust during the stance phase of the left knee. He uses a single point cane contralaterally. The left knee demonstrates chronic moderate effusion, with visible quadriceps atrophy compared to the contralateral limb. The surgical incision scar is well-healed, non-erythematous, and without signs of dehiscence, sinus tracts, or warmth. No superficial breakdown or signs of acute infection are noted.
Palpation reveals moderate warmth over the medial and lateral joint lines, consistent with chronic inflammation. A significant, firm effusion is palpable, but no discrete fluctuance is identified. Tenderness is elicited diffusely around the joint, particularly medially and laterally, and along the patellofemoral articulation. The posterior aspect of the knee is soft and non-tender.
Range of motion (ROM) of the left knee reveals a painful arc from 5 degrees of flexion contracture to 85 degrees of active flexion. Passive flexion achieves 90 degrees with significant end-range pain. Patellar tracking is notable for lateral tilt and mild subluxation with knee flexion, consistent with patellofemoral malalignment.
Ligamentous stability testing demonstrates significant findings. Varus stress testing at 0 degrees and 30 degrees of flexion elicits substantial laxity, graded as 2+ with a firm but indistinct endpoint, suggesting medial collateral ligament (MCL) insufficiency or elongation. Valgus stress testing reveals mild laxity at 0 degrees, but 1+ laxity at 30 degrees, suggesting some lateral collateral ligament (LCL) compromise or laxity, possibly secondary to the overall instability. Anterior-posterior stability testing shows 1+ anterior translation and 2+ posterior translation, indicating possible posterior cruciate ligament (PCL) compromise or tibial insert subluxation in this PS TKA, compounded by global instability. The Jobe test for posterolateral corner integrity is equivocal but suggests increased external rotation recurvatum.
Neurological examination of the left lower extremity reveals intact sensation to light touch in the L2-S1 dermatomes. Motor strength is 4/5 for knee extension and flexion, likely limited by pain and disuse atrophy. Distal pulses (dorsalis pedis and posterior tibial) are bilaterally palpable and symmetric. Capillary refill is brisk. There are no signs of deep vein thrombosis.
Imaging & Diagnostics
Initial diagnostic workup commenced with standard weight-bearing radiographs of the left knee, including AP, lateral, and skyline patellar views. Long-leg alignment views were also obtained.
Radiographic Findings:
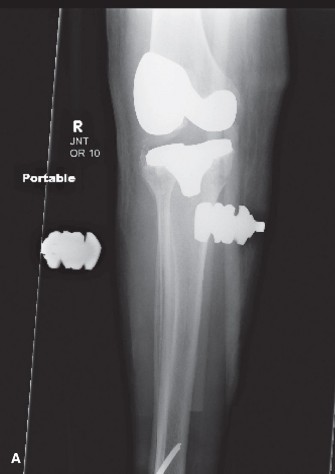
The AP view demonstrates evidence of polyethylene wear, with notable narrowing of the medial joint space. A small radiolucent line is observed at the cement-bone interface along the medial tibial plateau, extending into the metadiaphysis, consistent with potential aseptic loosening of the tibial component. There is evidence of subtle subsidence of the tibial component. The femoral component appears well-fixed, though there is a hint of slight femoral component internal rotation. The patellar component shows evidence of lateral tilt and mild superior subluxation. There are lucencies noted around the patellar component.
The lateral view confirms the tibial component subsidence and suggests posterior translation of the tibia relative to the femur, possibly related to PCL insufficiency or advanced polyethylene wear affecting the PS post-cam mechanism. Significant osteolysis is visible on the posterior aspect of the distal femur, consistent with particle disease.
The skyline patellar view confirms significant lateral patellar tilt and subluxation.
The long-leg alignment films reveal a persistent varus mechanical axis of 8 degrees, which is a significant deviation from neutral and potentially contributes to the medial compartment overload and instability. The previous tibial plateau fracture fixation hardware (screws) is noted, but not directly impinging on the TKA components.

(Fig 1. Representative anteroposterior radiograph demonstrating findings consistent with aseptic loosening of the tibial component, polyethylene wear, and varus malalignment.)
Given the chronic pain, effusion, and radiographic signs suggestive of loosening, a detailed workup to rule out periprosthetic joint infection (PJI) was initiated. Erythrocyte Sedimentation Rate (ESR) was elevated at 45 mm/hr (normal <20 mm/hr), and C-reactive Protein (CRP) was 12 mg/L (normal <5 mg/L).
A knee aspiration was performed under fluoroscopic guidance. Synovial fluid analysis revealed:
* White Blood Cell (WBC) count: 3,500 cells/µL
* Polymorphonuclear (PMN) percentage: 78%
* Alpha-defensin test: Negative
* Gram stain: No organisms observed
* Cultures (aerobic, anaerobic, fungal, acid-fast bacilli): Pending at the time of initial evaluation, but subsequently reported as negative after 14 days.
Based on the MSIS (Musculoskeletal Infection Society) criteria, the elevated ESR/CRP combined with the synovial fluid WBC and PMN percentage were concerning but did not meet definitive criteria for chronic PJI given the negative alpha-defensin and cultures. This highlights the diagnostic challenge in differentiating aseptic loosening from low-grade PJI.
A computed tomography (CT) scan with metal artifact reduction protocol was obtained to further assess component rotation, bone loss, and patellofemoral kinematics.
CT Findings:
The CT scan confirmed 7 degrees of internal rotation of the femoral component relative to the surgical epicondylar axis and 10 degrees of internal rotation of the tibial component relative to the transmalleolar axis. Significant bone loss was identified: a Type 2A defect on the medial tibial metaphysis (AORI classification) due to stress shielding and osteolysis, and a Type 1 femoral defect posteriorly. The patellar component demonstrated significant lateral tilt and subluxation, with erosion of the lateral facet of the patella. The posterior PS post-cam mechanism showed significant wear.
(Fig 2. Representative axial CT scan image demonstrating significant internal rotation of the femoral component and lateral patellar subluxation.)
Templating for revision components was initiated using the patient's contralateral knee as a reference and scaling techniques, anticipating the need for stemmed components, augments, and potentially a more constrained implant.
Differential Diagnosis
The comprehensive workup for a painful total knee arthroplasty requires careful consideration of several etiologies. In this case, the primary differentials revolve around mechanical failure versus infection.
| Feature | Aseptic Loosening / Mechanical Failure | Periprosthetic Joint Infection (PJI) | Instability |
|---|---|---|---|
| Pain Character | Gradual onset, progressive, mechanical, worse with activity, improves with rest. | Constant, throbbing, sometimes at rest or nocturnal. May be inflammatory. | Mechanical symptoms: giving way, buckling, clunking. Pain due to micro-motion. |
| Swelling/Effusion | Chronic, moderate, often sterile. | Chronic or acute, can be inflammatory, purulent. | Recurrent, often associated with episodes of instability. |
| Constitutional Symptoms | Absent. | Fever, chills, fatigue, malaise (especially high-grade). Low-grade PJI may lack these. | Absent. |
| Wound Status | Well-healed, no erythema or drainage. | Erythema, warmth, tenderness, sinus tract formation (pathognomonic). | Well-healed. |
| Radiographs | Radiolucent lines >2mm, subsidence, osteolysis, component migration. | Radiolucent lines (often rapid progression), periosteal reaction, osteolysis. | Component malposition, polyethylene wear, fracture (rarely causes primary instability). |
| ESR/CRP | Mildly elevated, or normal. | Significantly elevated. May be mildly elevated in chronic low-grade PJI. | Normal or mildly elevated. |
| Synovial Fluid (WBC) | <3,000 cells/µL (often), PMN <70%. | >3,000 cells/µL (chronic), >10,000 (acute); PMN >80%. MSIS criteria vary. | <3,000 cells/µL, PMN <70%. |
| Synovial Fluid (Culture) | Negative. | Positive for specific organism (gold standard). | Negative. |
| Alpha-Defensin | Negative. | Positive (high sensitivity/specificity). | Negative. |
| CT Scan | Component malrotation, bone loss, wear. | Can show bone erosion, periosteal reaction. Less specific than other tests. | Component malposition (rotation/alignment), patellar maltracking. |
| Bone Scan | Increased uptake around components (often diffuse). | Increased uptake (often intense, more focal). Less specific for infection vs. loosening alone. | Normal or mild uptake. |
| Intraoperative | Intact synovium, clear fluid, stable components or clear evidence of loosening at interface. | Purulence, fibrin, necrotic tissue, positive frozen section. | Ligamentous laxity, component malposition, polyethylene wear, PCL rupture. |
| Management | Revision arthroplasty. | Two-stage (or one-stage in selected cases) revision arthroplasty with antibiotics. | Revision arthroplasty with appropriate soft tissue balancing, component sizing/type. |
In our patient's case, while the synovial fluid WBC count (3,500 cells/µL) and PMN percentage (78%) were borderline concerning for PJI based on MSIS criteria for chronic infection (WBC >2,500 cells/µL, PMN >80% or two positive cultures), the negative alpha-defensin test, negative cultures, and the absence of definitive radiographic signs of active infection (e.g., rapid lucency progression, periosteal reaction) strongly pointed towards aseptic loosening complicated by component malrotation and mechanical instability as the primary diagnosis. The elevated ESR/CRP was considered reactive to the inflammatory process of aseptic loosening and bone particle disease rather than active infection, especially given the borderline fluid analysis and negative specific markers. The significant laxity on examination and component malrotation on CT further supported the diagnosis of instability secondary to prosthetic failure.
Surgical Decision Making & Classification
The decision for operative intervention was straightforward in this case, given the patient's severe, debilitating pain, significant functional impairment, progressive mechanical instability, and failure of all non-operative measures. The imaging and diagnostic findings strongly indicated a mechanical failure of the primary TKA with significant component malposition and bone loss, leading to aseptic loosening and instability. Continued conservative management would not address the underlying mechanical issues.
Classification:
-
AORI (American Academy of Orthopaedic Surgeons Orthopaedic Research and Education Foundation) Bone Defect Classification:
- Femoral side: Primarily Type 1 defect (contained cavitary defect, typically not involving cortical bone) due to posterior osteolysis. This would likely be managed with cement and potentially small augments.
- Tibial side: Type 2A defect on the medial tibial metaphysis (contained defect with loss of cancellous bone and partial loss of cortical bone), indicating the need for bone grafting or modular augments. The posteromedial defect was more significant, suggesting a larger augment or even a small stem.
-
AAOS Periprosthetic Joint Infection (PJI) Criteria:
- Though PJI was suspected initially, the workup (negative alpha-defensin, negative cultures, and borderline synovial fluid parameters) ultimately ruled it out as the primary etiology, shifting the focus to aseptic mechanical failure. Had criteria been met, a two-stage revision would have been the preferred strategy.
-
Insall Classification for Patellofemoral Complications:
- The severe lateral patellar tilt and subluxation seen on imaging and examination would be addressed through component rotation correction and potentially patellar resurfacing if not previously done, or revision patellar component with lateral release as needed.
Pre-operative Planning:
Extensive pre-operative planning was crucial.
*
Component Selection:
Based on the significant bone loss and anticipated instability, a constrained condylar knee (CCK) system was selected. This system allows for increased varus/valgus stability and often provides a higher posterior constraint than a PS design, compensating for soft tissue deficits and potential PCL insufficiency. Stemmed components for both femur and tibia were planned to provide metaphyseal and diaphyseal fixation, bypassing areas of bone loss and ensuring long-term stability. Modular augments (medial tibial and posterior femoral) were included in the plan.
*
Bone Grafting:
Autograft or allograft material was prepared for addressing larger bone defects, if needed, beyond the capacity of augments.
*
Surgical Approach:
Anticipating a difficult exposure due to previous surgery and potential scarring, a standard medial parapatellar approach was chosen initially, with contingency plans for an extensile approach (e.g., quadriceps snip or V-Y quadriceps plasty) if necessary.
*
Logistics:
Ensuring availability of a full revision set, including various sizes of stems, augments, and different levels of constraint (from CCK to rotating hinge knee, RHK) was paramount.
The surgical plan focused on explantation of the failed components, thorough debridement, meticulous assessment and reconstruction of bone defects, precise component positioning to restore mechanical alignment and rotational control, and robust soft tissue balancing to achieve a stable, well-tracking knee.
Surgical Technique / Intervention
The patient was positioned supine on the operating table. General anesthesia was administered, and a tourniquet was applied to the proximal thigh. Pre-operative prophylactic antibiotics (cefazolin) were administered intravenously.
1. Exposure and Capsulotomy:
The previous medial parapatellar incision was reopened. A standard medial parapatellar arthrotomy was performed. Significant scar tissue and adhesions were encountered, requiring careful sharp and blunt dissection to mobilize the patella and gain adequate exposure. The quadriceps mechanism was stiff and foreshortened. Due to the difficulty in everting the patella and to gain sufficient exposure for component removal and bone preparation, a small quadriceps snip was deemed necessary to prevent avulsion of the patellar tendon.
2. Synovectomy and Debridement:
Gross examination of the joint revealed a moderate, dark, serous effusion with evidence of dark polyethylene debris and synovitis. A thorough debridement and synovectomy were performed to remove all inflammatory tissue and loose bodies. Intraoperative frozen section analysis of synovial tissue was sent to pathology, which subsequently confirmed no evidence of acute inflammation or infection, further supporting the aseptic etiology.
3. Component Explantation:
The patellar component was found to be loose and was carefully removed. The tibial polyethylene insert exhibited severe medial wear and posterior dislocation from the tibial tray, contributing to the instability. The tibial component was found to be grossly loose with significant cement mantle compromise and substantial osteolysis on the medial side. Specialized extraction tools were utilized to carefully remove the tibial component without further compromising the bone stock. The femoral component was found to be slightly internally rotated but well-fixed, necessitating careful removal using an osteotome at the cement-bone interface, followed by gentle extraction. The posterior femoral condyles showed significant erosions from the PS post. All cement was meticulously removed from both the femur and tibia.
4. Bone Defect Management and Preparation:
Upon component removal, the extent of bone loss was clearly visible. On the medial tibial metaphysis, a contained AORI Type 2A defect was confirmed, requiring a 10mm modular tibial augment. The distal femur presented a posterior AORI Type 1 defect, which was managed with a small posterior femoral augment. The femoral and tibial canals were reamed for stemmed components, ensuring adequate diaphyseal engagement. The remaining bone surfaces were prepared using standard revision cutting blocks to achieve precise bone resections for the new components, targeting restoration of the mechanical axis.
5. Trial Reduction and Soft Tissue Balancing:
A trial reduction was performed using a revision CCK system with appropriately sized stemmed components and augments. This system was chosen to provide increased constraint to compensate for the ligamentous laxity identified pre-operatively and intraoperatively. Sequential soft tissue releases were performed to balance the knee. A persistent varus imbalance was present, despite initial bony cuts. This required a deep release of the MCL insertion from the tibia and partial release of the semimembranosus tendon to achieve balanced flexion and extension gaps. The flexion and extension gaps were meticulously assessed, ensuring symmetry and stability throughout the range of motion. The patella was again assessed for tracking; given the correction of component rotation and improved balance, its tracking was significantly improved, and a lateral release was not required at this stage.
6. Definitive Component Implantation:
The trial components were removed. The bone surfaces were thoroughly irrigated and dried. The revision femoral component, with its posterior augment and long stem, was cemented in appropriate rotation and varus/valgus alignment. Care was taken to ensure optimal fill of the femoral canal and augment seating. Similarly, the revision tibial component, with its medial augment and long stem, was cemented into place, ensuring correct rotational alignment, coronal and sagittal alignment, and full seating of the augment. A new constrained polyethylene insert was placed. The patella was resurfaced with a new component, carefully centered to optimize patellofemoral tracking. All cement was meticulously cleaned from the joint.
7. Closure:
The knee was taken through a full range of motion, confirming excellent stability, tracking, and no impingement. The quadriceps snip was repaired with strong interrupted sutures. The medial parapatellar capsule and retinaculum were closed in layers. A subcutaneous drain was placed. The skin was closed with staples. A sterile dressing and a compressive soft bandage were applied.
Post-Operative Protocol & Rehabilitation
Immediate Post-Operative Period (Day 0-3):
*
Pain Management:
Multimodal analgesia protocol including opioid patient-controlled analgesia (PCA) or scheduled oral opioids, NSAIDs (if no contraindications), acetaminophen, and gabapentinoids. Adductor canal nerve blocks were utilized pre-operatively for initial pain control.
*
Deep Vein Thrombosis (DVT) Prophylaxis:
Low molecular weight heparin (LMWH) initiated on post-operative day 1 and continued for 4-6 weeks, alongside mechanical compression devices.
*
Weight-Bearing:
Touch-down weight-bearing (TDWB) of 10-20% body weight on the operated limb using a walker or crutches was initiated immediately. This restriction was critical due to the stemmed components, augments, and extensive bone defects.
*
Range of Motion (ROM):
Continuous Passive Motion (CPM) machine initiated at 0-60 degrees, gradually increasing to patient tolerance. Active and passive ROM exercises encouraged within pain limits, focusing on gentle flexion and extension.
*
Wound Care:
Drain typically removed on post-operative day 1 or 2 if output is minimal. Dressing changes every 48 hours, monitoring for signs of infection.
*
Physical Therapy (PT):
Initial focus on quad sets, gluteal sets, ankle pumps, gentle knee flexion/extension exercises, and transferring techniques.
Early Rehabilitation (Week 1-6):
*
Weight-Bearing:
Progression to partial weight-bearing (PWB) of 50% by week 2-3, gradually increasing towards full weight-bearing (FWB) by week 6, contingent on radiographic evidence of bone healing and clinical stability.
*
ROM:
Continue to work on achieving functional ROM (0-120 degrees). Focus on gentle stretching and mobilization.
*
Strengthening:
Progressive resisted exercises for quadriceps, hamstrings, and gluteal muscles. Isometric holds, straight leg raises, mini-squats (within limits of pain and weight-bearing status).
*
Gait Training:
Continue with gait training, focusing on proper mechanics, balance, and reducing assistive device dependence.
*
Scar Mobilization:
Gentle massage around the incision once healed to prevent adhesions.
Intermediate Rehabilitation (Week 7-12):
*
Weight-Bearing:
Full weight-bearing as tolerated.
*
Strengthening:
Increase intensity of resistance exercises. Introduce balance and proprioception exercises. Cycling (stationary bike) and elliptical training without resistance.
*
Functional Training:
Progress to single-limb stance, step-ups, step-downs. Focus on endurance and functional activities related to daily living.
*
ROM:
Continue stretching to maintain and improve flexibility.
Advanced Rehabilitation (Month 3-6+):
*
Return to Activity:
Gradual return to low-impact activities such as walking, swimming, golfing (if appropriate). Avoid high-impact sports.
*
Strengthening:
Advanced strengthening with higher resistance, plyometric exercises if appropriate for the patient and implant.
*
Proprioception & Agility:
Sport-specific drills if applicable, focusing on dynamic stability and control.
*
Long-term Monitoring:
Regular follow-up appointments with the surgeon, yearly radiographs to monitor for implant integrity, lucency, or subsidence. Education on activity modification and early recognition of potential complications.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Thorough Pre-operative Workup: Never assume aseptic loosening without rigorously ruling out PJI. Borderline ESR/CRP and synovial fluid values always warrant a thorough investigation, including alpha-defensin and prolonged cultures. Intraoperative frozen section is critical.
- Comprehensive Imaging: Standard radiographs are a start, but long-leg alignment films are paramount for assessing overall limb alignment. CT scans with metal artifact reduction are invaluable for component rotational alignment and precise assessment of bone loss. MRI is less useful due to artifact, but can aid in soft tissue assessment for specific indications.
- Detailed Pre-operative Templating: This is non-negotiable for revision TKA. Understand the anticipated bone defects (AORI classification), the required implant constraint, stem length, and augment needs. Have a full revision tray available.
- Extensile Exposure: Be prepared for a difficult exposure. A quadriceps snip or V-Y quadriceps plasty should be in your armamentarium to prevent extensor mechanism complications and ensure adequate visualization.
- Meticulous Cement Removal: Residual cement can lead to third-body wear, inflammation, and interfere with new component seating.
- Bone Defect Management: Address bone loss systematically. Use augments, impaction grafting, or custom implants as dictated by the AORI classification. Ensure a stable foundation for the new components.
- Soft Tissue Balancing: In revision TKA, soft tissues are often scarred, contracted, or incompetent. Achieving balanced flexion and extension gaps in a stable fashion often requires sequential releases and judicious choice of implant constraint (e.g., CCK or RHK). Varus/valgus and rotational stability are critical.
- Restoration of Mechanical Axis: The primary goal of TKA, especially revision, is to restore a neutral mechanical axis. This minimizes polyethylene wear and improves long-term implant survival.
- Extensor Mechanism Protection: The extensor mechanism is the Achilles' heel of TKA. Protect it throughout the procedure. Any compromise (patellar fracture, patellar tendon avulsion) is devastating.
- Post-Operative Rehabilitation: A structured and progressive rehabilitation protocol is crucial for achieving optimal outcomes, managing pain, improving range of motion, and regaining strength and function. Emphasize weight-bearing restrictions based on fixation.
Pitfalls:
- Missing a Low-Grade Infection: The most dangerous pitfall. Misdiagnosing PJI as aseptic loosening can lead to catastrophic failure of a subsequent revision and prolonged morbidity for the patient. A high index of suspicion and complete workup are essential.
- Inadequate Exposure: Forcing components into place or making incomplete cuts due to poor exposure dramatically increases the risk of malposition, component impingement, and subsequent failure.
- Ignoring Bone Loss: Failure to adequately address bone defects leads to unstable components, subsidence, and early failure. Using standard primary TKA techniques in a revision setting with bone loss is a recipe for disaster.
- Inadequate Soft Tissue Balancing: Not achieving stable and balanced flexion and extension gaps will result in ongoing instability, pain, and premature wear.
- Component Malrotation: This is a common cause of persistent pain and patellofemoral issues post-TKA, especially in revision. Utilize anatomical landmarks (surgical epicondylar axis, Whiteside's line for femoral rotation; tibial tubercle for tibial rotation) and intraoperative assessment.
- Extensor Mechanism Complications: Patellar fracture, patellar tendon rupture, or quadriceps rupture are severe complications that can lead to permanent functional deficits. Over-resection of the patella or aggressive soft tissue releases can predispose to these.
- Over-Constraining the Knee: While constraint is often necessary in revision, excessive constraint (e.g., unnecessarily using an RHK) can lead to increased stress at the implant-bone interface, limiting ROM, and transferring stress to adjacent joints. Use the minimum constraint required for stability.
- Poor Patient Selection or Expectation Management: Unrealistic patient expectations regarding pain relief, functional return, or activity levels after complex revision TKA can lead to patient dissatisfaction despite a technically successful surgery. Pre-operative counseling is vital.
- Inadequate Fixation: Failure to achieve appropriate press-fit or cement mantle in stemmed components, particularly bypassing bone defects, can lead to early aseptic loosening of the revision components.
- Pre-existing Comorbidities: Uncontrolled diabetes, smoking, and obesity significantly increase the risk of wound complications, infection, and poor healing, impacting the overall success of the revision. Rigorous pre-optimization is crucial.
You Might Also Like