Proximal Humerus Cartilaginous Tumors: Navigating the Enchondroma-Chondrosarcoma Dilemma

Key Takeaway
Differentiating enchondroma from low-grade chondrosarcoma in the proximal humerus involves assessing progressive pain, clinical findings, and detailed imaging. Key diagnostic indicators on X-ray and CT include chondroid matrix calcifications and the depth of endosteal scalloping. Significant scalloping (e.g., 3-4mm) with persistent pain strongly suggests potential for low-grade chondrosarcoma.
Patient Presentation & History
A 48-year-old male presented to our clinic with a chief complaint of insidious onset, dull aching pain in his left proximal humerus for the past 6 months. The pain was initially intermittent, localized to the deltoid region, and exacerbated by overhead activities. Over the last 2 months, the pain has become more constant, dull, and occasionally wakes him from sleep, though he denies any acute traumatic event. He reports no associated numbness, tingling, or weakness in the extremity. He has noted a mild, diffuse swelling over the proximal arm but no erythema or warmth.
His past medical history includes well-controlled hypertension and dyslipidemia, for which he takes lisinopril and atorvastatin. He has no known history of previous fractures or bone tumors. Surgical history is limited to an appendectomy at age 20. He is a non-smoker, drinks alcohol socially, and works as an accountant. Family history is negative for any genetic bone disorders or malignancies. He denies any constitutional symptoms such as fever, chills, night sweats, or unexplained weight loss. Of note, he reports no history of prior radiation exposure.
The primary concern, given the persistent and progressively worsening pain in the absence of trauma, was to rule out an underlying neoplastic process, particularly in a region commonly affected by cartilaginous tumors. This presentation immediately raises the diagnostic dilemma between benign lesions like enchondromas and potentially malignant transformations or de novo low-grade chondrosarcomas.
Clinical Examination
On general inspection, the patient appeared comfortable and in no acute distress. There was a subtle, diffuse fullness appreciated over the lateral aspect of the left proximal humerus, but no overt deformity, skin changes, or muscle atrophy. Active range of motion (ROM) of the left shoulder revealed mild discomfort at the extremes of abduction (>120°) and external rotation. Internal rotation was full and pain-free. Passive ROM was generally well-preserved but elicited mild pain at end-range abduction.
Palpation revealed deep tenderness over the lateral aspect of the left humeral shaft, approximately 5 cm distal to the greater tuberosity. The area of fullness felt firm but not hard, and there was no palpable mass with distinct margins. No warmth or erythema was noted. There was no demonstrable crepitus with shoulder movement. Axillary lymph nodes were non-palpable.
Neurological examination of the left upper extremity revealed intact motor function (Medical Research Council grade 5/5) in all myotomes, including deltoid, biceps, triceps, wrist extensors/flexors, and intrinsic hand muscles. Sensory examination to light touch and pinprick was normal in the C5-T1 dermatomes. Reflexes (biceps, triceps, brachioradialis) were 2+ and symmetrical bilaterally.
Vascular examination demonstrated palpable radial, ulnar, and brachial pulses that were 2+ and symmetrical. Capillary refill was brisk (<2 seconds) in all digits. No bruits were appreciated.
Special tests for rotator cuff pathology (e.g., Neer, Hawkins, Jobe's) were mildly positive for pain but not indicative of a discrete tear. These findings, particularly the progressive nature of the pain and the localized tenderness without significant mechanical symptoms or overt inflammatory signs, further underscored the need for comprehensive imaging to evaluate for an underlying osseous pathology.
Imaging & Diagnostics
Initial diagnostic workup commenced with plain radiographs, which are the cornerstone for evaluating primary bone lesions.
Plain Radiographs
Anteroposterior and lateral radiographs of the left humerus were obtained. These revealed a well-circumscribed, intramedullary lytic lesion within the diaphysis of the proximal humerus, approximately 6 cm in length. The lesion exhibited classic characteristics of a cartilaginous tumor, including:
*
Punctate and arc-like calcifications:
Described as "popcorn" or "ring-and-arc" calcifications, highly suggestive of chondroid matrix.
*
Endosteal scalloping:
Mild to moderate cortical thinning and erosion from the medullary side were observed along the medial and lateral cortices, particularly pronounced on the medial aspect. The endosteal scalloping measured approximately 3-4 mm in depth at its deepest point.
*
No aggressive periosteal reaction:
Absence of lamellated, spiculated, or Codman's triangle periosteal reaction. The cortex appeared largely intact, without clear signs of cortical breakthrough.
*
No soft tissue mass:
No obvious associated soft tissue component.
The radiographic features, while compatible with an enchondroma, specifically the presence of endosteal scalloping and persistent pain, raised suspicion for a low-grade chondrosarcoma.
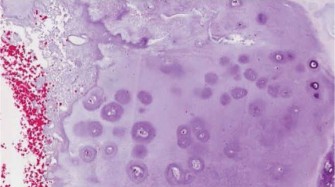
Figure 1: Initial AP radiograph of the left humerus demonstrating an intramedullary lytic lesion with punctate calcifications and mild endosteal scalloping.
Figure 2: Lateral radiograph showing the extent of the lesion within the medullary canal, reaffirming the presence of chondroid matrix calcifications.
Computed Tomography (CT)
Given the equivocal nature of distinguishing between enchondroma and low-grade chondrosarcoma based on plain films alone, a non-contrast CT scan of the left humerus was performed. The CT provided superior detail regarding cortical integrity and matrix mineralization.
*
Cortical Evaluation:
The CT scan confirmed mild to moderate endosteal scalloping, with the deepest area measuring up to 4 mm on the medial cortex. There was no overt cortical breach or aggressive periosteal reaction.
*
Matrix Detail:
The chondroid matrix calcifications were more clearly delineated, showing a classic ring-and-arc pattern throughout the lesion.
*
No Soft Tissue Extension:
No extraosseous soft tissue mass was identified.
The CT findings, while still leaning towards a cartilaginous lesion, highlighted the extent of endosteal erosion, which is a critical differentiating feature. Lesions with endosteal scalloping greater than 2/3 of the cortical thickness or >1 cm are more suspicious for chondrosarcoma. In our patient, the scalloping was significant enough to warrant further investigation.
Magnetic Resonance Imaging (MRI)
An MRI of the left humerus with and without intravenous contrast was subsequently obtained to further characterize the lesion's biological activity and relationship to surrounding neurovascular structures.
*
T1-weighted sequences:
Showed a heterogeneous signal intensity, predominantly intermediate to low signal, consistent with a cartilaginous matrix.
*
T2-weighted/STIR sequences:
Demonstrated high signal intensity within the lesion, indicating high water content typical of hyaline cartilage. Importantly, areas of focal increased signal intensity, suggestive of myxoid degeneration or edema, were noted.
*
Post-contrast T1-weighted sequences with fat saturation:
Revealed heterogeneous, peripheral, nodular, or ring-and-arc enhancement patterns within the lesion. Notably, there were areas of more diffuse, intense enhancement, raising further suspicion for a low-grade chondrosarcoma rather than a simple enchondroma, which typically shows minimal or punctate peripheral enhancement.
*
Marrow Edema:
Minimal surrounding marrow edema was present.
*
Neurovascular Bundles:
The brachial plexus and axillary neurovascular structures were uninvolved.
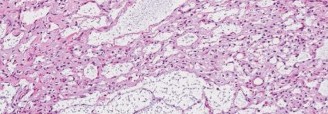
Figure 3: Coronal T1-weighted MRI demonstrating the intramedullary lesion with intermediate signal intensity.

Figure 4: Axial T2-weighted MRI showcasing the high signal intensity characteristic of cartilage, along with subtle surrounding marrow changes.
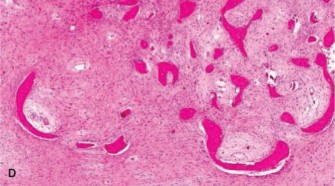
Figure 5: Post-contrast T1-weighted MRI with fat saturation, revealing heterogeneous, nodular enhancement, a concerning feature for potential malignancy.
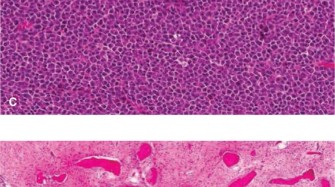
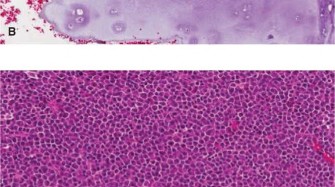
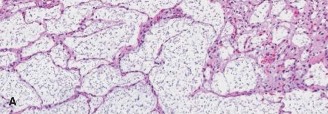
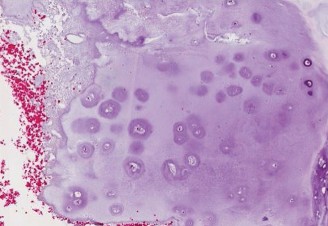
Biopsy
Given the persistent pain and the concerning imaging features (significant endosteal scalloping, heterogeneous enhancement on MRI), an image-guided core needle biopsy was performed. The biopsy was planned carefully to avoid contaminating surrounding tissues, using a longitudinal approach that could be easily excised if a wider resection were required. The pathologist reported findings consistent with a cartilaginous tumor with mild nuclear atypia, binucleated chondrocytes, and increased cellularity in focal areas. These features were considered borderline and non-definitive for an overt malignancy, leading to a diagnosis of "atypical cartilaginous tumor (ACT)" or "enchondroma with features suggestive of low-grade chondrosarcoma." This histological ambiguity, coupled with the clinical symptoms and radiographic concerns, solidified the diagnostic dilemma.
Differential Diagnosis
The key to managing cartilaginous lesions, particularly in the long bones, lies in accurately differentiating between an enchondroma and a low-grade chondrosarcoma (Grade I). This distinction can be challenging due to overlapping radiological and histological features. Other considerations include fibrous dysplasia (monostotic or polyostotic), bone infarct, and more aggressive chondrosarcoma grades.
| Feature | Enchondroma | Low-Grade Chondrosarcoma (Grade I) | Fibrous Dysplasia (FD) | Bone Infarct |
|
Clinical Presentation
| Often asymptomatic. May present with pain (especially with low-grade malignancy), swelling, or pathologic fracture (rare). | |
|
Patient Demographics
| 48-year-old male. | 48-year-old male. | | | | |
|
Clinical Presentation | Pain (insidious, dull, aching, worse at night/activity), swelling, possible pathological fracture (rare if solitary and small). | Persistent pain (progressively worsening, especially at night, unrelieved by rest/analgesics), palpable mass, pathological fracture (more common than enchondroma). Symptoms may be vague, hence the 'dilemma'. | Usually asymptomatic. Can cause pain if very large or pathological fracture (rare). | Sudden onset of severe pain, particularly in joints (femoral head, humeral head). Can be asymptomatic in early stages. Distinct risk factors. | | | | | | |
|
Radiographic Findings | Well-defined, intramedullary lytic lesion. Punctate or "popcorn" calcifications. Mild endosteal scalloping (< 2/3 cortical thickness, < 1 cm depth). No cortical breach or aggressive periosteal reaction. |
|
MRI Features | Homogeneous high T2 signal. Minimal or punctate peripheral enhancement on post-contrast images. No soft tissue component. Absence of significant marrow edema. | Heterogeneous T2 signal, often with intermediate/low signal areas (fibrosis, calcification). Peripheral nodular or diffuse enhancement. Marrow edema (more frequent than enchondroma), possible cortical breakthrough, soft tissue component. May have periosteal reaction. | Normal bone architecture. | Normal, but can be seen in rare cases of atypical presentation or subtle low-grade disease progression. | Bone Infarct (FD is typically a bone lesion, not affecting architecture, but some studies may show some commonality). Fibrous dysplasia can mimic some features of chronic bone infarct on MRI (e.g., serpentine low signal rim of bone infarct). | |
|
Treatment Considerations
| Most enchondromas are asymptomatic and require no treatment. If symptomatic or concerning, may consider curettage with bone grafting. If suspicious, proceed with careful observation and serial imaging. If symptoms persist or progress, consider biopsy or removal. | En bloc resection with wide margins is the gold standard, when anatomically possible, to reduce local recurrence. Curettage is generally not appropriate for definitive treatment. Adjuvant radiation therapy in specific cases (e.g., incomplete resection, high-grade tumors). Chemotherapy is largely ineffective for conventional chondrosarcoma. | Fib | | |
| |
| | |
|
Fibrous Dysplasia (FD)** | Normal bone architecture. Typically asymptomatic, discovered incidentally. Usually a "bone lesion" of fibrous bone, with different features from a cartilaginous tumor. | Monostotic or Polyostotic forms. Expansile lytic lesion, "ground-glass" matrix. No calcifications. No cortical destruction. May have shepherd's crook deformity in the femur. Can also occur in long bones. | |
| |
| | | | | |
Clinical & Radiographic Imaging
You Might Also Like