Lower Limb Trauma: Master Urgent Management & Ace Your Exams
Key Takeaway
We review everything you need to understand about Lower Limb Trauma: Master Urgent Management & Ace Your Exams. Lower limb trauma, specifically hip dislocation, constitutes a surgical emergency due to significant risks like femoral head avascularity, chondrolysis, and neurovascular compromise. Initial management involves ATLS principles, thorough assessment for associated injuries, and evaluating neurovascular status, particularly the sciatic nerve. Urgent closed or open reduction under general anesthesia is critical to restore joint integrity and prevent severe long-term complications.
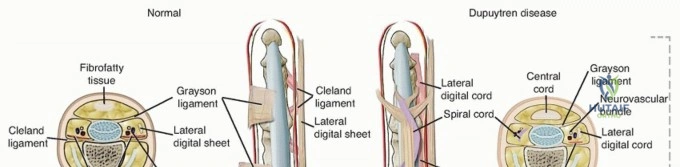
A 65-year-old patient presents with a chronic, flexion deformity of the ulnar digit. You are asked to discuss the management options for Dupuytren’s contracture. How would you counsel this patient regarding the differences between Needle Aponeurotomy and Collagenase injection?
Candidate: I would discuss both as minimally invasive options. Needle aponeurotomy involves using a needle to mechanically divide the cord, while collagenase injection enzymatically lyses the cord. Needle aponeurotomy is cheap but has a high recurrence rate, whereas collagenase is more expensive and has side effects like skin tearing or local inflammation.
The candidate fails to address the specific patient anatomy. A high-scoring answer must mention that collagenase is no longer widely available/withdrawn in many markets and that both methods are restricted to specific contracture severities (Tubiana grades). Failing to mention the risk of tendon rupture or neurovascular injury shows a lack of clinical nuance.
A structured answer: 1. Classification: Confirm the Tubiana stage; these are best for cord-based disease, not bulky palmar nodules. 2. Needle Aponeurotomy: Explain the mechanical division of cords; emphasize it is an office-based procedure, cost-effective, but technically demanding with a risk of neurovascular injury (digital nerves at risk). 3. Collagenase (Clostridium histolyticum): Acknowledge its enzymatic mechanism; discuss historical advantages (no surgery) and disadvantages (significant local inflammatory reaction, skin tears, and current global supply limitations/market withdrawal). 4. Comparison: Compare recurrence rates to formal fasciectomy (higher) and contrast the recovery profile—emphasizing that for a 65-year-old, minimal downtime is the primary goal.
