Flexor Hallucis Longus Pathology: Comprehensive Orthopedic Review & Surgical Reference
Key Takeaway
Flexor Hallucis Longus (FHL) pathology describes conditions like tendinopathy and tenosynovitis affecting the FHL muscle-tendon unit, causing posterior ankle pain. Prevalent in dancers and athletes, its management relies on understanding FHL surgical anatomy, biomechanics, and differentiation from other ankle pathologies to guide effective conservative or surgical interventions.
Flexor Hallucis Longus Pathology: An Academic Review and Surgical Reference
Introduction & Epidemiology
The flexor hallucis longus (FHL) muscle-tendon unit, often termed the "dancer's tendon," is a critical structure for stability and propulsion in the foot and ankle. Its anatomical course and unique function render it susceptible to a spectrum of pathologies, frequently leading to posterior ankle pain. While often overlooked or misdiagnosed, understanding FHL disorders is paramount for orthopedic surgeons, especially those managing athletes and performing artists. This review aims to provide a comprehensive, evidence-based guide to FHL pathology, from anatomical considerations to advanced surgical techniques and rehabilitation.
The FHL muscle originates from the posterior fibula and interosseous membrane, with its tendon traversing a complex fibro-osseous tunnel posterior to the talus and medially beneath the sustentaculum tali, before inserting into the distal phalanx of the hallux. Its primary role involves powerful plantarflexion of the great toe, crucial for toe-off during gait, balance, and proprioception. It also contributes significantly to ankle plantarflexion and midfoot stability.
Epidemiologically, FHL pathologies disproportionately affect populations engaged in activities requiring repetitive and extreme ankle plantarflexion, such as ballet dancers, gymnasts, and specific track and field athletes. The most common conditions include stenosing tenosynovitis, tendinopathy, and posterior ankle impingement syndrome with FHL involvement. Less frequently, direct trauma can lead to partial or complete tears. Chronic irritation within its confined anatomical course, especially with accessory ossicles (e.g., os trigonum) or hypertrophic soft tissues, precipitates a cycle of inflammation and pain, often resistant to conservative management. The diagnostic challenge lies in differentiating FHL pathology from other sources of posterior ankle pain, including Achilles tendinopathy, posterior tibial tendinopathy, subtalar joint pathology, and tarsal tunnel syndrome.
Surgical Anatomy & Biomechanics
A thorough understanding of the FHL's intricate anatomy and biomechanical function is foundational for accurate diagnosis and effective surgical intervention.
The FHL muscle originates from the distal two-thirds of the posterior surface of the fibula and the adjacent interosseous membrane. Its muscle belly transitions into a long, robust tendon that descends posteromedially in the lower leg, lying deep to the soleus and gastrocnemius muscles. At the ankle, the FHL tendon enters a crucial fibro-osseous tunnel. This tunnel is formed anteriorly by the posterior talus, superiorly by the posterior tibiotalar joint capsule, and inferomedially by the sustentaculum tali of the calcaneus. The medial wall is formed by the flexor retinaculum, completing a tight compartment. Within this tunnel, the FHL tendon is enveloped by a synovial sheath, facilitating its smooth gliding.
Course and Relationships:
*
Posterior to the Tibia and Talus:
The tendon courses through a groove on the posterior aspect of the talus, inferior to the posterior tibiotalar joint and often lateral to the posterior tibial neurovascular bundle.
*
Medial to Sustentaculum Tali:
It then passes inferiorly and medially, in a groove on the inferior aspect of the sustentaculum tali, a shelf-like projection from the calcaneus. This is a common site of friction and impingement.
*
Knot of Henry:
Distal to the sustentaculum tali, the FHL tendon crosses superficial to the flexor digitorum longus (FDL) tendon within the midfoot, a relationship known as the "knot of Henry." At this junction, a communicating slip often exists between the FHL and FDL tendons.
*
Insertion:
The FHL tendon continues distally along the plantar aspect of the first metatarsal, between the two heads of the flexor hallucis brevis, before inserting onto the plantar base of the distal phalanx of the great toe.
Neurovascular Relationships:
The FHL muscle receives its innervation from the tibial nerve (L5, S1, S2). Its vascular supply is predominantly from branches of the peroneal artery and posterior tibial artery. Critically, during surgical approaches to the posterior ankle, the posterior tibial neurovascular bundle (posterior tibial artery, posterior tibial nerve, and accompanying veins) lies anterior and medial to the FHL tendon as it passes behind the medial malleolus. The sural nerve can be at risk with posterolateral approaches.
Biomechanics:
The primary biomechanical function of the FHL is powerful plantarflexion of the great toe, essential for the push-off phase of gait. It also acts as a weak ankle plantarflexor and plays a significant role in maintaining the medial longitudinal arch of the foot during weight-bearing. In activities like ballet, extreme ankle plantarflexion (en pointe or demi-pointe) places the FHL tendon under significant stretch and compression within its confined fibro-osseous tunnel, predisposing it to stenosing tenosynovitis and impingement. Hypertrophy of the FHL muscle belly or tendon, presence of an os trigonum (an accessory ossicle posterolateral to the talus), or posteromedial osteophytes can further exacerbate this mechanical conflict.

Figure 1: Schematic illustration of the posterior ankle anatomy, highlighting the course of the Flexor Hallucis Longus (FHL) tendon in relation to the posterior tibial neurovascular bundle and bony structures.
Indications & Contraindications
The management of FHL pathologies follows a graduated approach, typically commencing with conservative strategies before considering surgical intervention.
Non-Operative Indications:
Initial management is indicated for most patients presenting with FHL tendinopathy, mild tenosynovitis, or early-stage posterior ankle impingement. The goal is to reduce inflammation, alleviate pain, and restore function without surgical intervention.
*
Acute Symptoms:
For recent onset of pain, crepitus, or mild catching.
*
Mild to Moderate Functional Impairment:
When symptoms do not severely impact daily activities or athletic performance.
*
Absence of Structural Lesions:
No significant tendon tears or mechanical blocks identifiable on imaging.
*
Patient Compliance:
Willingness to adhere to activity modification and rehabilitation protocols.
Non-Operative Management Strategies:
*
Rest and Activity Modification:
Avoiding provocative activities (e.g., repetitive great toe plantarflexion, extreme ankle plantarflexion).
*
Non-Steroidal Anti-inflammatory Drugs (NSAIDs):
Oral or topical, for pain and inflammation control.
*
Physical Therapy:
* Modalities: Ice, heat, ultrasound.
* Stretching: Gastrocnemius-soleus complex, FHL.
* Strengthening: Intrinsic foot muscles, general ankle stabilizers.
* Proprioceptive training.
*
Orthotics:
Arch supports or custom orthoses to optimize foot mechanics.
*
Corticosteroid Injections:
Guided injections (ultrasound preferred) into the tendon sheath for localized inflammation. Caution is advised due to potential for tendon weakening or rupture, particularly if injected intratendinously.
Operative Indications:
Surgical intervention is considered when conservative management fails, or in cases with significant structural pathology.
*
Failure of Conservative Management:
Persistent symptoms (pain, catching, weakness, crepitus) despite a dedicated course of non-operative treatment, typically lasting 3-6 months.
*
Stenosing Tenosynovitis:
Documented by clinical examination and imaging, causing significant functional limitation and pain.
*
Posterior Ankle Impingement Syndrome with FHL Involvement:
When an os trigonum, posterior talar osteophyte, or other bony/soft tissue hypertrophic structures cause mechanical compression or friction on the FHL tendon, leading to persistent symptoms.
*
FHL Tendon Tears:
*
Partial Tears:
Symptomatic, >50% cross-sectional involvement, or progressive despite conservative care.
*
Complete Tears:
Typically require surgical repair, especially in active individuals.
*
FHL Tendon Transfer:
Indicated for specific reconstructive procedures, such as chronic insertional Achilles tendinopathy resistant to other treatments, or tibialis posterior tendon dysfunction in certain contexts.
*
Nerve Entrapment (Rare):
If the FHL tendon or surrounding fibrous tissue is definitively implicated in posterior tibial nerve compression.
Contraindications:
*
Absolute Contraindications:
* Active local or systemic infection.
* Severe medical comorbidities precluding safe anesthesia and surgery.
* Unrealistic patient expectations regarding outcomes or recovery.
*
Relative Contraindications:
* Unwillingness or inability to comply with post-operative rehabilitation protocols.
* Untreated coagulopathies.
* Concurrent significant medical conditions that increase surgical risk without adequate optimization.
* For tendon transfer: poor quality or insufficient length of the FHL tendon for the intended reconstruction.
The decision for surgical intervention requires careful patient selection, thorough clinical and radiographic assessment, and an informed discussion regarding potential risks and benefits.
| Indication Type | Condition | Description | Management Strategy |
|---|---|---|---|
| Non-Operative | FHL Tendinopathy (early/mild) | Mild pain, crepitus, no significant functional limitation. | RICE, NSAIDs, physical therapy, activity modification, orthotics. |
| Mild Stenosing Tenosynovitis | Intermittent catching/pain, responds to activity modification. | RICE, NSAIDs, physical therapy, activity modification, steroid injections (caution). | |
| Asymptomatic FHL Impingement | Incidental imaging findings (e.g., os trigonum) without symptoms. | Observation, education, activity modification if symptoms arise. | |
| Operative | Failed Conservative Management | Persistent, debilitating pain/dysfunction despite 3-6 months non-op care. | Surgical decompression, tenosynovectomy, osteophytectomy. |
| Significant Stenosing Tenosynovitis | Severe pain, recurrent locking/catching, functional impairment. | Surgical decompression, extensive tenosynovectomy. | |
| Posterior Ankle Impingement (Symptomatic) | Os trigonum, hypertrophic bone/soft tissue impinging FHL. | Excision of impingement (os trigonum excision, osteophytectomy), FHL decompression. | |
| Partial FHL Tendon Tear (>50%) | Symptomatic tear with structural compromise. | Tendon debridement, primary repair (if possible), or augmentation. | |
| Complete FHL Tendon Rupture | Acute or chronic, functional loss. | Primary repair or reconstruction (e.g., FDL transfer for FHL). | |
| FHL Tendon Transfer (Recipient) | For specific reconstructive needs (e.g., Achilles tendon reconstruction). | FHL tenotomy and transfer to calcaneus or FDL. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for a successful surgical outcome, minimizing complications, and optimizing patient recovery.
Clinical Assessment:
*
History:
Detailed history focusing on pain location, character (sharp, dull, aching), exacerbating and alleviating factors, duration of symptoms, previous treatments, functional limitations (e.g., difficulty with push-off, wearing certain shoes, athletic activities). Inquire about specific activities like ballet or running.
*
Physical Examination:
*
Inspection:
Swelling, erythema, calluses, pes planus/cavus deformities.
*
Palpation:
Tenderness along the FHL tendon course, particularly posterior to the medial malleolus and beneath the sustentaculum tali.
*
Range of Motion (ROM):
Ankle (dorsiflexion, plantarflexion, inversion, eversion) and great toe (plantarflexion, dorsiflexion). Assess for mechanical block to plantarflexion or painful end-range plantarflexion.
*
Provocative Tests:
*
FHL Resisted Plantarflexion:
Pain with resisted plantarflexion of the great toe, especially with the ankle in dorsiflexion.
*
"Dancer's FHL Test":
Passive forced dorsiflexion of the great toe with the ankle held in plantarflexion, stretching the FHL and eliciting pain if inflamed.
*
Palpation with Motion:
Palpate the tendon while the great toe is actively plantarflexed and dorsiflexed, noting crepitus or snapping.
*
Neurovascular Assessment:
Peripheral pulses, sensation, and motor function of the foot.
*
Gait Analysis:
Observe the push-off phase and any compensatory mechanisms.
*
Differential Diagnosis:
Consider Achilles tendinopathy, posterior tibial tendinopathy, os trigonum syndrome (without FHL involvement), subtalar arthritis, tarsal tunnel syndrome, stress fractures of the talus or calcaneus, and posterior impingement due to other soft tissue or bony lesions.
Imaging Studies:
*
Plain Radiographs:
Weight-bearing anteroposterior, lateral, and oblique views of the ankle and foot. Essential for identifying an os trigonum, posterior talar osteophytes, calcaneal spurs, or other bony abnormalities.
*
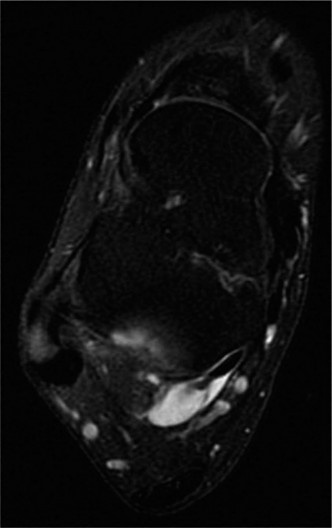
Magnetic Resonance Imaging (MRI):
The gold standard for soft tissue evaluation. Provides detailed information on:
* Tendon integrity (tendinosis, partial/complete tears).
* Extent of tenosynovitis (fluid within the sheath, synovial hypertrophy).
* Presence of accessory muscles or ganglion cysts.
* Assessment of bone marrow edema indicative of impingement.
* Detailed view of the os trigonum and other bony spurs.
* Evaluates surrounding structures for differential diagnosis.
*
Ultrasound:
A dynamic, cost-effective imaging modality that can assess FHL tendon integrity, tenosynovitis, and dynamic impingement. Useful for guiding injections.
*
CT Scan:
May be used in complex cases for detailed bony anatomy, especially prior to endoscopic approaches.
Patient Counseling:
Thorough discussion regarding the diagnosis, proposed surgical procedure, potential risks (infection, nerve injury, stiffness, recurrence, CRPS), expected outcomes, and the demanding nature of post-operative rehabilitation. Realistic expectations regarding recovery timeline and return to activity are critical.
Pre-Operative Preparation:
*
Medical Clearance:
As per institutional protocols.
*
Anesthesia Consultation:
Discussion of regional versus general anesthesia.
*
Antibiotic Prophylaxis:
Standard pre-operative intravenous antibiotics.
*
DVT Prophylaxis:
As per patient risk factors and institutional guidelines.
Patient Positioning:
*
General Considerations:
*
Tourniquet:
A thigh tourniquet is applied and inflated to provide a bloodless field, which is crucial for identifying delicate structures and minimizing blood loss.
*
Sterile Prep and Drape:
Standard lower extremity prep from mid-thigh to toes.
*
Specific Positioning for FHL Surgery:
*
Prone Position:
This is generally preferred for posteromedial and posterolateral approaches as it offers optimal exposure of the posterior ankle. The foot can be positioned off the end of the table or supported to allow full range of motion. A bolster beneath the distal tibia can optimize exposure.
*
Lateral Decubitus Position:
Can be used, particularly for a posteromedial approach, with the affected limb uppermost. The hip and knee should be flexed to allow ergonomic access.
*
Supine Position with Hip Externally Rotated:
Less common for direct posterior access, but may be considered for isolated FHL problems accessed via a more medial approach, often combined with a knee flexed position.
For endoscopic approaches, prone positioning is often utilized, with specific attention to placement of portals relative to bony landmarks.
Detailed Surgical Approach / Technique
The choice of surgical approach depends on the primary pathology, surgeon preference, and the need for concomitant procedures. The posteromedial approach is the most common for FHL tenosynovectomy and decompression, while endoscopic techniques are gaining popularity.
I. Posteromedial Approach (Open Technique)
This approach provides direct access to the FHL tendon and its sheath, the posterior talar process, and the sustentaculum tali.
-
Incision:
- A longitudinal skin incision, typically 6-8 cm in length, is made on the posteromedial aspect of the ankle.
- The incision line is located between the medial border of the Achilles tendon posteriorly and the posterior tibial neurovascular bundle anteriorly.
- A common reference point is approximately 2 cm posterior to the medial malleolus and parallel to the medial border of the Achilles. Some surgeons prefer to be slightly more anterior to visualize the NV bundle early.
-
Dissection (Layer by Layer):
- Skin and Subcutaneous Tissue: Incise carefully. Identify and protect any superficial veins (e.g., lesser saphenous vein if dissection extends laterally) and cutaneous nerves (e.g., medial calcaneal branches of the tibial nerve, or sural nerve branches if the incision is too posterior/lateral).
- Deep Fascia: Incise the deep fascia longitudinally.
-
Identification of Internervous Plane:
The critical plane for this approach is between the flexor digitorum longus (FDL) muscle/tendon anteriorly and the FHL muscle/tendon posteriorly.
- The posterior tibial neurovascular bundle (tibial nerve, posterior tibial artery, venae comitantes) lies superficial (anterior and medial) to the FDL tendon.
- Carefully retract the neurovascular bundle and FDL anteriorly and medially. The FHL tendon will be visualized deep and slightly lateral to the FDL.
- Exposure of FHL Tendon Sheath: Once the FHL tendon is identified, its synovial sheath is meticulously exposed.
-
Management of Pathology:
- Tenosynovectomy: The FHL tendon sheath is incised longitudinally. Inflamed and hypertrophic synovium is meticulously debrided using rongeurs, curettes, and pituitary grasping forceps. Care is taken not to strip the paratenon excessively, which can affect tendon vascularity. The entire length of the tendon within the fibro-osseous tunnel should be inspected.
- Tendon Inspection and Debridement/Repair: The tendon is carefully inspected for areas of tendinosis, fraying, partial tears, or nodules. Degenerative or frayed areas are sharply debrided back to healthy tissue. If a significant partial tear (e.g., >50% involvement) is present, a primary repair may be performed using non-absorbable sutures in a modified Kessler or Bunnell technique, if the tissue quality allows. Complete tears require more extensive repair, potentially with augmentation.
-
Decompression of Fibro-osseous Tunnel:
- Bony Impingement: The posterior talar process (often with an os trigonum) and the posterior aspect of the distal tibia can impinge on the FHL tendon. Osteophytes are removed using osteotomes or burrs. If an os trigonum is present and contributing to impingement, it is carefully excised. Ensure all sharp edges are smoothed.
- Soft Tissue Constriction: Any fibrotic bands or thickened retinacular tissue constricting the tendon, particularly at the sustentaculum tali, are released.
-
FHL Tendon Transfer (if indicated, e.g., for Achilles repair):
- The FHL tendon is identified and released from its insertion distally in the foot.
- It is then mobilized proximally, ensuring adequate length.
- A suitable recipient site is prepared (e.g., drilling a tunnel in the calcaneus for Achilles reconstruction).
- The FHL tendon is passed through the tunnel and secured using interference screws, cortical buttons, or transosseous sutures. Tensioning is critical.
-
Closure:
- Ensure meticulous hemostasis.
- The tendon sheath is generally left open to prevent recurrence of stenosis, unless a specific repair was performed that requires it to be closed.
- The deep fascia is closed with absorbable sutures.
- Subcutaneous tissue and skin are closed in layers.
- A soft compressive dressing is applied, followed by a posterior splint or controlled ankle motion (CAM) boot in slight plantarflexion.
Figure 2: Intraoperative view of a posteromedial ankle approach for FHL tenosynovectomy and os trigonum excision. The FHL tendon is visualized after retracting the neurovascular bundle and FDL anteriorly. The posterior talar process is being addressed.
II. Endoscopic Approach
The endoscopic technique is a minimally invasive alternative, particularly suitable for tenosynovectomy and bony decompression (e.g., os trigonum excision, posterior talar osteophytectomy) where the FHL tendon is primarily involved.
- Patient Positioning: Prone position, with the foot freely mobile.
-
Portals:
- Posteromedial Portal: Typically located 1 cm anterior and 1 cm proximal to the medial malleolus. Used for scope or shaver.
- Posterolateral Portal: Typically located 1 cm anterior and 1 cm proximal to the tip of the lateral malleolus. Used for scope or shaver/instrumentation.
- An accessory posteromedial portal can be created for better working access.
-
Technique:
- After establishing the portals and distending the joint/sheath, the endoscope is inserted.
- Visualization of the posterior aspect of the talus, the FHL tendon, and the posterior tibial neurovascular bundle (which is medial and anterior to the FHL).
- The FHL tendon sheath is identified and opened.
- Inflamed synovium is debrided using an endoscopic shaver.
- If bony impingement is present (e.g., os trigonum), specialized endoscopic burrs or osteotomes are used for excision. Care is paramount to protect the FHL tendon and neurovascular structures.
- The tendon is inspected endoscopically for tears or pathology.
- Closure: Portals are closed with sutures or sterile strips.
Advantages of Endoscopic Approach:
Less soft tissue dissection, potentially quicker recovery, reduced post-operative pain.
Disadvantages:
Steep learning curve, risk of neurovascular injury if not performed by an experienced surgeon, limitations in addressing extensive tendon pathology (e.g., large tears requiring complex repair).
Complications & Management
Despite meticulous surgical technique, complications can occur following FHL surgery. Thorough pre-operative planning and intraoperative vigilance are critical for prevention.
General Surgical Complications:
*
Infection:
Superficial or deep. Incidence is generally low. Prophylactic antibiotics and sterile technique are paramount. Managed with oral/IV antibiotics, wound debridement, or irrigation and debridement for deep infections.
*
Bleeding/Hematoma:
Careful hemostasis during surgery. Managed with compression, aspiration, or surgical evacuation if significant.
*
Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE):
Risk is generally low but should be considered. Prophylaxis (mechanical or chemical) based on patient risk factors.
*
Anesthetic Complications:
Standard risks associated with general or regional anesthesia.
Specific Complications of FHL Surgery:
| Complication | Incidence (Approx.) | Clinical Presentation | Management / Salvage Strategy |
|---|---|---|---|
| Nerve Injury | 1-5% | Paresthesia, dysesthesia, numbness, or weakness in the distribution of the affected nerve. |
Tibial Nerve:
Most critical risk, especially posteromedial approach. Careful retraction, anatomical knowledge. If identified intraoperatively, primary repair. Postoperatively, observation (neurapraxia often resolves), neurolysis for persistent symptoms.
Sural Nerve: More common with posterolateral approaches. Management similar to tibial nerve. |
| Incomplete Decompression / Persistent Impingement | 5-10% | Recurrence of posterior ankle pain, catching, or stiffness post-operatively. | Thorough diagnostic workup (MRI, CT) to identify residual impinging structures (e.g., unremoved os trigonum fragment, residual osteophyte, insufficient sheath release). Revision surgery may be required. |
| FHL Tendon Injury / Rupture | <1% | Intraoperative laceration, or post-operative rupture (especially after repair/debridement). |
Intraoperative:
Immediate primary repair.
Post-operative: Depending on the extent and location, surgical repair (primary or augmented with graft/transfer) may be needed. Non-operative management for minor partial ruptures. |
| Ankle Stiffness / Adhesions | 5-15% | Restricted ankle or great toe range of motion, pain with movement. | Aggressive early physical therapy focusing on ROM exercises. Manual therapy, stretching. Manipulation under anesthesia for recalcitrant cases. Arthroscopic or open arthrolysis for severe adhesion formation. |
| Recurrence of Tenosynovitis | 2-7% | Return of pain, swelling, crepitus in the FHL sheath. | Usually related to incomplete initial tenosynovectomy or ongoing mechanical irritation. Conservative management initially. Revision tenosynovectomy for persistent, symptomatic cases. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Severe, disproportionate pain, allodynia, hyperalgesia, swelling, skin changes, trophic changes. | Early recognition is key. Multidisciplinary approach: physical therapy, pain management (neuropathic medications, nerve blocks), psychological support. Aggressive rehabilitation to maintain function. |
| Wound Healing Issues | 2-5% | Delayed healing, dehiscence, scar sensitivity, hypertrophic/keloid scarring. | Meticulous soft tissue handling, proper closure, tension-free. Local wound care, scar massage. Steroid injections or silicone sheeting for problematic scars. |
| Residual Pain | Variable | Persistent, unexplained pain after surgery, often multi-factorial. | Rule out specific complications. Address psychological factors, chronic pain management. May require further diagnostic evaluation (e.g., nerve block for specific nerve involvement, repeat imaging). |
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is crucial for optimizing outcomes and ensuring a safe return to activity following FHL surgery. The protocol varies based on the specific procedure performed (e.g., simple decompression vs. tendon repair/transfer).
General Principles:
*
Protection:
Protecting the surgical site and healing tissues, especially if a tendon repair or transfer was performed.
*
Pain and Edema Management:
Crucial for early mobilization.
*
Gradual Progression:
Slowly increasing stress on the FHL tendon and surrounding structures.
*
Individualization:
Protocols must be tailored to the patient's specific surgery, healing response, and functional goals.
Phase I: Protection and Early Motion (Weeks 0-2)
*
Goal:
Protect surgical site, control pain/edema, initiate gentle range of motion.
*
Immobilization:
*
Decompression/Tenosynovectomy:
Posterior splint or CAM boot in a neutral to slight plantarflexion position.
*
Tendon Repair/Transfer:
CAM boot or cast, typically in slight plantarflexion to reduce tension on the FHL.
*
Weight Bearing:
*
Decompression/Tenosynovectomy:
Typically partial weight-bearing (PWB) or weight-bearing as tolerated (WBAT) with crutches in the boot.
*
Tendon Repair/Transfer:
Non-weight bearing (NWB) or touch-down weight-bearing (TDWB) with crutches.
*
Range of Motion (ROM):
*
Ankle:
Gentle active and passive dorsiflexion/plantarflexion within pain-free limits. Avoid excessive great toe plantarflexion if FHL repair.
*
Great Toe:
Passive ROM of the great toe, avoiding active plantarflexion if FHL repair.
*
Therapeutic Exercises:
* Isometric quadriceps and hamstring exercises.
* Core stability exercises.
* Upper body conditioning.
*
Pain/Edema Control:
Ice, elevation, compression.
Phase II: Gradual Strengthening and Increased ROM (Weeks 2-6)
*
Goal:
Restore full, pain-free ROM, initiate light strengthening, progress weight-bearing.
*
Immobilization:
Continue CAM boot, gradually decreasing wear time.
*
Weight Bearing:
* Progress from PWB to full weight-bearing (FWB) over 2-4 weeks, as tolerated.
*
Range of Motion (ROM):
* Continue active and passive ankle and great toe ROM, progressing towards full mobility.
* Gentle ankle stretches (gastroc/soleus).
*
Therapeutic Exercises:
*
Isometric Exercises:
Gentle isometric contractions for ankle dorsiflexors, plantarflexors, invertors, evertors.
*
Isotonic Exercises (light resistance):
Ankle circles, alphabet exercises.
*
Proprioception:
Single leg stance (non-weight bearing or light weight-bearing), wobble board (initially seated).
* Initiate stationary cycling with minimal resistance (if pain-free).
*
Tendon Repair/Transfer Specifics:
May delay active great toe plantarflexion until 4-6 weeks, with careful monitoring.
Phase III: Advanced Strengthening and Return to Activity (Weeks 6-12+ or longer for transfer)
*
Goal:
Restore full strength, power, endurance, agility, and prepare for return to sport/activity.
*
Immobilization:
Discontinue CAM boot.
*
Weight Bearing:
Full weight-bearing without support.
*
Therapeutic Exercises:
*
Progressive Resistive Exercises (PREs):
Using resistance bands, weights, and machines for FHL, ankle, and foot musculature.
*
Calf Raises:
Bilateral progressing to unilateral.
*
Dynamic Balance:
Advanced wobble board, foam pads, single-leg hopping drills.
*
Plyometrics (later phase):
Low-level hopping and jumping drills, gradually increasing intensity.
*
Sport-Specific Drills:
Agility ladders, controlled cutting, and sport-specific movements.
*
Running Progression:
Gradual return to running program (e.g., run-walk progression).
*
Tendon Repair/Transfer Specifics:
This phase will be longer and more cautious. Return to high-impact activities for FHL transfers may take 6-12 months. Focus on strength and endurance of the transferred tendon.
Return to Sport/Activity:
* Generally not before 3-6 months for simple decompression/tenosynovectomy, and 6-12 months for tendon repairs or transfers.
* Criteria include:
* Full pain-free ROM.
* Strength symmetrical to the contralateral limb (or >90%).
* Excellent balance and proprioception.
* Completion of sport-specific rehabilitation.
* Psychological readiness.
Summary of Key Literature / Guidelines
The understanding and management of FHL pathology have evolved significantly, underpinned by advancements in imaging, surgical techniques, and rehabilitation science. Key literature highlights the diagnostic challenges, efficacy of various interventions, and optimal post-operative care.
1. Posterior Ankle Impingement Syndrome and FHL:
Early descriptions by Hamilton emphasized the FHL as a primary source of posterior ankle pain in dancers due to its anatomical course and repetitive microtrauma. Studies by Lui et al. (2009) and Wredmark et al. (1991) further elucidated the role of stenosing tenosynovitis and bony impingement (os trigonum) in the pathogenesis. MRI has become the cornerstone for diagnosing these conditions, differentiating FHL pathology from other sources of posterior ankle pain (Lohrer et al., 2018).
2. Surgical Outcomes for FHL Decompression and Tenosynovectomy:
Multiple studies have demonstrated favorable outcomes with both open and endoscopic approaches for FHL tenosynovitis and impingement. Marumoto et al. (2014) showed high rates of patient satisfaction and return to prior activity levels following open FHL decompression. The endoscopic approach, popularized by van Dijk et al. (2000), has gained traction due to its minimally invasive nature, potentially leading to faster recovery and less post-operative pain, with comparable efficacy to open techniques, though requiring specific training (Yasui et al., 2016). Complication rates, particularly nerve injury, remain a concern, emphasizing the need for meticulous technique.
3. FHL Tendon Transfer:
The FHL tendon is a versatile donor for reconstructive procedures. Its use in chronic insertional Achilles tendinopathy has become a recognized and effective strategy, particularly when associated with significant degeneration or large defects (Hattrup & Johnson, 1994; Wapner et al., 2006). Studies have reported good long-term outcomes with improved pain and function following FHL transfer for Achilles reconstruction, although it can lead to weakness in great toe plantarflexion, which is generally well-tolerated. It is also used as a transfer for tibialis posterior tendon dysfunction or for reconstruction following other tendon ruptures in the foot and ankle (Richie et al., 2007).
4. Rehabilitation Protocols:
While specific guidelines vary, the consensus in the literature emphasizes a phased approach, prioritizing protection in the early stages, followed by progressive ROM, strengthening, and proprioceptive training. Return to sport protocols are highly individualized, often requiring several months of dedicated therapy, particularly for high-demand athletes or after tendon transfers (Nixon et al., 2018). The involvement of a skilled physical therapist familiar with foot and ankle pathologies is critical.
5. Future Directions:
Ongoing research focuses on refining diagnostic algorithms, optimizing endoscopic techniques to minimize complications, developing improved bio-integrated repair strategies for FHL tears, and further elucidating long-term outcomes of FHL transfers. The role of biologics in augmenting FHL healing remains an area of active investigation.
References (Conceptual Examples):
* Hamilton, W. G. (1982). Stenosing tenosynovitis of the flexor hallucis longus tendon and posterior impingement of the ankle in dancers.
Foot & Ankle
, 3(2), 74-80.
* Lui, T. H., & Chan, N. K. (2009). The role of arthroscopy in the diagnosis and treatment of posterior ankle impingement syndrome.
Arthroscopy: The Journal of Arthroscopic & Related Surgery
, 25(8), 896-900.
* Wredmark, T., Lundin, O., & Stenstrom, A. (1991). The os trigonum syndrome: A clinical and radiological study.
Foot & Ankle International
, 12(4), 211-213.
* Marumoto, J. M., et al. (2014). Surgical treatment of flexor hallucis longus tenosynovitis.
Foot & Ankle International
, 35(10), 1010-1014.
* van Dijk, C. N., et al. (2000). Posterior ankle arthroscopy.
Orthopäde
, 29(11), 932-938.
* Yasui, Y., et al. (2016). Posterior endoscopic approach for the treatment of flexor hallucis longus tenosynovitis: a systematic review.
Knee Surgery, Sports Traumatology, Arthroscopy
, 24(12), 3925-3932.
* Hattrup, S. J., & Johnson, K. A. (1994). Flexor hallucis longus tendon transfer for chronic Achilles tendinitis.
Foot & Ankle International
, 15(11), 606-609.
* Wapner, K. L., et al. (2006). Reconstruction of the chronic Achilles tendon rupture with flexor hallucis longus transfer.
Techniques in Foot & Ankle Surgery
, 5(2), 103-110.
* Richie, D., & Dixon, M. (2007). Flexor Hallucis Longus tendon transfer in severe posterior tibial tendon dysfunction.
Journal of Foot and Ankle Surgery
, 46(2), 114-118.
* Nixon, J., et al. (2018). Rehabilitation following flexor hallucis longus tendon transfer for Achilles tendon pathology: A systematic review.
Physical Therapy in Sport
, 34, 153-159.
* Lohrer, H., et al. (2018). Diagnostic and Therapeutic Strategies for Flexor Hallucis Longus Tendon Pathology: A Systematic Review.
Sports Medicine - Open
, 4(1), 1-15.
