Surgical Management of the Upper Extremity in Cerebral Palsy
Key Takeaway
The surgical management of the upper extremity in cerebral palsy aims to improve function, hygiene, and cosmesis. This comprehensive guide details evidence-based approaches to spasticity, including dynamic electromyography, botulinum toxin application, and targeted surgical interventions. Key procedures discussed encompass pronator teres rerouting, flexor carpi ulnaris tendon transfers, and thumb-in-palm deformity correction, providing orthopedic surgeons with a rigorous framework for optimizing patient outcomes.
Introduction to the Spastic Upper Extremity
The surgical management of the upper extremity in cerebral palsy (CP) represents one of the most complex challenges in pediatric and reconstructive orthopedics. The primary objective of surgical intervention is to enhance the patient's quality of life by improving upper limb function, facilitating hygiene, and addressing severe cosmetic deformities that cause psychological distress.
Cerebral palsy is a non-progressive encephalopathy, but the musculoskeletal manifestations are highly progressive. The typical spastic upper extremity presents with a predictable pattern of deformity: shoulder internal rotation, elbow flexion, forearm pronation, wrist flexion, ulnar deviation, finger flexion, and a thumb-in-palm deformity. This textbook-level guide synthesizes decades of evidence-based literature to provide a comprehensive framework for the evaluation, biomechanical understanding, and step-by-step surgical execution of upper extremity reconstruction in the CP patient.
Preoperative Evaluation and Decision-Making
Patient selection and meticulous preoperative planning are the cornerstones of successful outcomes. Surgery is generally deferred until the child is at least 6 to 8 years old, allowing for neurologic maturation, the establishment of a definitive motor pattern, and the ability to cooperate with postoperative rehabilitation.
Clinical Assessment and Goal Setting
The surgeon must distinguish between dynamic spasticity (muscle overactivity that resolves under anesthesia) and static myostatic contracture (fixed shortening of the musculotendinous unit).
Clinical Pearl: Always evaluate the hand in multiple positions. The "tenodesis effect" is critical; a patient may only be able to extend their fingers when the wrist is maximally flexed. Correcting the wrist flexion deformity without addressing the finger flexors may inadvertently strip the patient of their only mechanism for grasp and release.
The Role of Dynamic Electromyography (EMG)
Pioneered by Hoffer and colleagues, dynamic EMG is an invaluable tool for surgical decision-making. Surface or fine-wire EMG is utilized during functional tasks (e.g., reaching, grasping, and releasing) to identify which muscles are firing out of phase.
* In-phase muscles: Fire during their intended physiologic action.
* Out-of-phase muscles: Fire continuously or during antagonistic movements, making them prime candidates for release, lengthening, or transfer.
Botulinum Toxin A as a Diagnostic and Therapeutic Adjunct
Botulinum toxin A (BoNT-A) acts by inhibiting acetylcholine release at the neuromuscular junction, providing temporary relief of focal spasticity.
Surgical Warning: BoNT-A is not merely a temporizing measure; it is a profound diagnostic tool. Injecting the flexor carpi ulnaris (FCU) or pronator teres (PT) can simulate the functional outcome of a surgical release or transfer. If a BoNT-A injection unmasks underlying weakness in the antagonist muscles (e.g., wrist extensors), a simple release will fail, and a tendon transfer is mandated.
Management of Forearm Pronation Deformity
Forearm pronation contracture severely limits the patient's ability to position the hand in space, particularly for feeding and self-care, which require supination. The primary deforming forces are the pronator teres (PT) and the pronator quadratus (PQ).
Indications for Surgery
- Pronator Tenotomy/Release: Indicated for severe, rigid contractures where active supination is entirely absent, and the goal is purely passive correction for hygiene or cosmesis.
- Pronator Teres Rerouting: Indicated for patients with dynamic pronation spasticity who possess some underlying, albeit weak, active supination.
Surgical Technique: Pronator Teres Rerouting
The PT rerouting procedure converts the spastic pronator into an active supinator.
- Positioning and Incision: The patient is positioned supine with the arm on a hand table. A longitudinal incision is made over the middle third of the radial aspect of the volar forearm.
- Exposure: The interval between the brachioradialis (BR) and the flexor carpi radialis (FCR) is developed. The superficial radial nerve and the radial artery are identified and meticulously protected.
- Tendon Harvest: The insertion of the PT on the lateral aspect of the radius is identified. The tendon is detached with a generous strip of periosteum to maximize length.
- Mobilization: The PT is mobilized proximally. Care must be taken not to injure the median nerve branches supplying the muscle belly.
- Rerouting: The tendon is passed through the interosseous membrane (from volar to dorsal) or routed circumferentially around the radius (from volar to dorsal, then radial).
- Fixation: With the forearm held in maximum supination, the tendon is anchored back to its original insertion site or to the anterolateral radius using a suture anchor or transosseous sutures.
Management of Wrist Flexion Deformities
Wrist flexion with ulnar deviation is the hallmark of the spastic CP hand. The FCU is almost universally the primary deforming force.
Flexor Carpi Ulnaris (FCU) to Extensor Carpi Radialis Brevis (ECRB) Transfer
First popularized by Green and Banks, this transfer removes the deforming volar-ulnar force and augments dorsal-radial extension.
Indications
- Dynamic wrist flexion deformity.
- Adequate passive wrist extension (at least neutral with fingers extended).
- Voluntary control of the fingers.
Surgical Technique
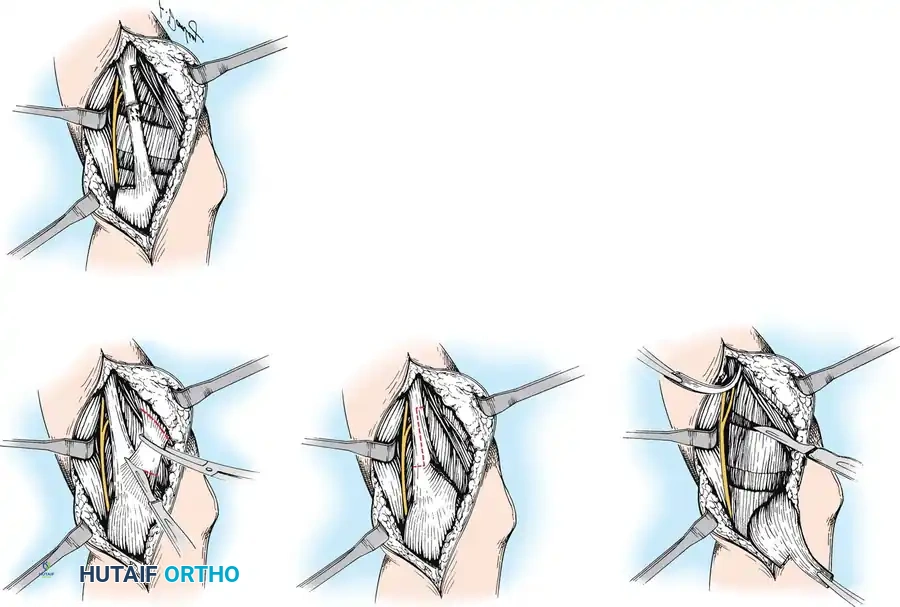
- Harvesting the FCU: A longitudinal incision is made over the distal volar-ulnar forearm. The FCU tendon is identified and detached directly from the pisiform.
- Mobilization: The FCU is mobilized proximally to the mid-forearm. The ulnar nerve and artery, which lie immediately deep and radial to the FCU, must be protected. The muscle belly is freed from its fascial attachments to allow adequate excursion.
- Preparation of the ECRB: A second longitudinal incision is made over the dorsal-radial wrist (base of the third metacarpal). The ECRB is identified. (The ECRB is chosen over the ECRL to prevent radial deviation and because it is a more central wrist elevator).
- Tendon Routing: A generous subcutaneous tunnel is created around the ulnar border of the forearm, directing the FCU from volar to dorsal.
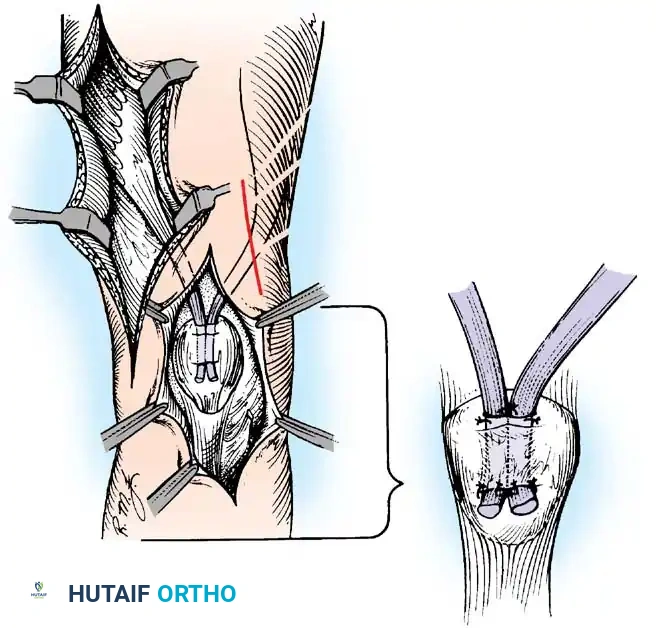
- Tendon Weave: Using a Pulvertaft weave, the FCU is interlaced through the ECRB.
- Tensioning: The transfer is tensioned with the wrist in 30 degrees of extension and the forearm in neutral rotation.
Pitfall: Over-tensioning the transfer or failing to address concomitant finger flexor spasticity can lead to a severe loss of grip strength. Always assess the finger flexors; if they are tight, fractional lengthening of the flexor digitorum superficialis (FDS) and profundus (FDP) must be performed simultaneously.
Flexor-Pronator Origin Release (Page Procedure)
For severe, rigid flexion contractures of the wrist and fingers where no functional recovery is expected, a muscle origin release (flexor-pronator slide) is indicated.
Surgical Technique
- Incision: A medial longitudinal incision is made over the distal humerus, extending across the elbow joint to the proximal ulnar forearm.
- Nerve Decompression: The ulnar nerve is identified, decompressed in the cubital tunnel, and protected. The median nerve is identified as it passes between the heads of the pronator teres.
- Muscle Release: The common flexor origin is sharply detached from the medial epicondyle. The origins of the FCU, FCR, PT, and FDS are elevated extra-periosteally and allowed to slide distally.
- Closure: The arm is immobilized in extension to allow the muscle mass to heal in its new, lengthened position.
Wrist Arthrodesis
In the mature patient with a severely contracted, non-functional hand, wrist arthrodesis provides a stable, cosmetically acceptable limb and facilitates perineal care and dressing.
- Approach: A dorsal longitudinal approach is utilized. Extensor tendons are mobilized and retracted.
- Joint Preparation: The radiocarpal and midcarpal joints are decorticated. Proximal row carpectomy (PRC) may be performed simultaneously to decompress the joint and allow correction of severe flexion without excessive tension on the neurovascular bundle.
- Fixation: A dorsal spanning reconstruction plate is applied from the distal radius to the third metacarpal.
Management of the Thumb-in-Palm Deformity
The thumb-in-palm deformity severely impairs prehension, preventing the patient from opening the first web space to grasp objects. House classified this deformity into four types based on the primary spastic muscles (adductor pollicis, flexor pollicis brevis, flexor pollicis longus, and first dorsal interosseous).
Surgical Correction Strategies
Correction typically requires a multi-level approach addressing both the intrinsic and extrinsic musculature.
1. Release of Spastic Intrinsics
- Adductor Pollicis Release: An incision is made along the palmar crease of the thenar eminence. The transverse and oblique heads of the adductor pollicis are identified and released from the third metacarpal.
- First Dorsal Interosseous Release: If the first web space remains tight, the origin of the first dorsal interosseous is stripped from the first metacarpal.
2. Lengthening of the Flexor Pollicis Longus (FPL)
If the interphalangeal (IP) joint of the thumb is held in rigid flexion, the FPL must be addressed. Fractional lengthening at the musculotendinous junction in the distal forearm is preferred over Z-lengthening to preserve some active flexion for pinch.
3. Augmentation of Thumb Extension/Abduction (EPL Rerouting)
To provide a dynamic force to keep the thumb out of the palm, the Extensor Pollicis Longus (EPL) can be rerouted.
* The EPL is released from the third dorsal compartment (Lister's tubercle).
* It is transposed radially and volarly, aligning it with the abductor pollicis longus (APL) and extensor pollicis brevis (EPB).
* This alters its biomechanical vector, converting it from a pure IP joint extensor into a robust thumb abductor and radial extensor.
4. Metacarpophalangeal (MCP) Joint Stabilization
If the MCP joint is highly unstable or hyperextends (a common compensatory mechanism), arthrodesis of the MCP joint is highly recommended. Fusion is typically performed in 15 degrees of flexion, 15 degrees of abduction, and slight pronation using crossed Kirschner wires or a compression screw.
Management of Finger Deformities: The Swan-Neck Deformity
Swan-neck deformities in CP are driven by intrinsic muscle spasticity, leading to MCP joint flexion, proximal interphalangeal (PIP) joint hyperextension, and distal interphalangeal (DIP) joint flexion.
Sublimis (FDS) Tenodesis
To prevent PIP hyperextension, a tenodesis of the flexor digitorum superficialis is performed.
1. A mid-lateral or volar Bruner incision is made over the PIP joint.
2. One slip of the FDS is divided proximally.
3. The divided slip is left attached to its distal insertion on the middle phalanx.
4. With the PIP joint held in 20 to 30 degrees of flexion, the proximal end of the divided slip is sutured to the A2 pulley or anchored into the proximal phalanx, creating a checkrein against hyperextension.
Postoperative Protocols and Rehabilitation
The success of upper extremity surgery in CP is inextricably linked to rigorous postoperative rehabilitation.
Immobilization
Postoperatively, the limb is typically immobilized in a long-arm cast for 4 to 6 weeks.
* For tendon transfers (e.g., FCU to ECRB), the wrist is casted in 20-30 degrees of extension.
* For PT rerouting, the forearm is casted in maximum supination.
* For thumb-in-palm corrections, a thumb spica cast is utilized with the first web space widely abducted.
Therapy and Neuromuscular Electrical Stimulation (NMES)
Upon cast removal, a custom thermoplastic splint is fabricated for nighttime use to prevent contracture recurrence. Daytime therapy focuses on motor re-education.
Clinical Pearl: The brain must be "taught" to use the newly transferred muscle. Neuromuscular electrical stimulation (NMES) is highly effective in the early postoperative phase. Applying NMES to the transferred muscle (e.g., the FCU now acting as a wrist extensor) provides proprioceptive feedback to the cortex, facilitating neuroplasticity and integration of the new motor pattern.
Conclusion
Surgical reconstruction of the spastic upper extremity in cerebral palsy requires a profound understanding of altered biomechanics, meticulous preoperative evaluation utilizing dynamic EMG and BoNT-A, and precise surgical execution. By systematically addressing pronation contractures, wrist flexion deformities, and thumb-in-palm pathology, the orthopedic surgeon can significantly enhance the functional capacity and quality of life for these complex patients. Mastery of these techniques, coupled with dedicated postoperative rehabilitation, remains the gold standard in neuro-orthopedic care.
You Might Also Like