Management of Hip Deformities in Cerebral Palsy: A Surgical Masterclass
Key Takeaway
Hip deformities in cerebral palsy range from mild subluxation to complete dislocation, driven by muscle imbalance, retained primitive reflexes, and altered biomechanics. Early detection using Reimers' migration percentage is critical. Surgical management, including adductor tenotomy and iliopsoas recession, aims to restore joint congruity, alleviate pain, and optimize ambulatory function. This guide details the pathophysiology, clinical evaluation, and step-by-step surgical techniques for managing spastic hip dysplasia.
Pathoanatomy and Biomechanics of the Spastic Hip
Deformities of the hip in patients with cerebral palsy (CP) represent a complex continuum ranging from mild, painless subluxation to complete dislocation accompanied by severe joint destruction, intractable pain, and profound impairment of mobility. Unlike developmental dysplasia of the hip (DDH), the hip in a child with cerebral palsy is typically anatomically normal at birth. The progressive deformity is acquired and multifactorial, driven primarily by spastic muscle imbalance, retained primitive reflexes, abnormal posturing, and secondary pelvic obliquity.
When a spastic hip begins to subluxate, the natural history is one of relentless progression; it rarely improves without decisive orthopedic intervention. The altered biomechanical forces across the joint, combined with delayed or absent weight-bearing, lead to profound structural bony deformities. These include progressive acetabular dysplasia, excessive femoral anteversion, an increased neck-shaft angle (coxa valga), and regional osteopenia.
Clinical Pearl: Increased femoral anteversion is significantly more common in ambulatory patients than in nonambulators and typically does not remodel or change significantly after 6 years of age.
Bobroff et al. demonstrated that with increasing age, the neck-shaft angle in children with CP paradoxically increases, contrasting sharply with the physiological varus remodeling seen in unaffected children. Furthermore, Baker et al. reviewed the radiographic appearance of 258 hips in 129 patients with CP, finding that only 21% were radiographically normal. Their analysis revealed valgus deformity of the femoral neck in 76%, increased acetabular roof obliquity in 62%, subluxation in 16%, dislocation in 12%, and varus deformity in a mere 2%. Baker postulated that prolonged spasticity of the adductor and flexor musculature leads to a relative overpowering of the abductors and extensors. This chronic imbalance causes growth inhibition of the greater trochanter, producing a relative valgus overgrowth of the proximal femur.
Epidemiology and Clinical Evaluation
Hip pain is a paramount complaint among young adults with cerebral palsy, severely impacting their quality of life. In a cross-sectional multicenter study by Hodgkinson et al., the prevalence of hip pain in 234 adult patients (mean age 28 years) was a staggering 47%. Progressive hip instability occurs in approximately 15% of all patients with CP, with the highest incidence seen in severely affected individuals, particularly those with spastic quadriplegia.
Sharrard noted that when nonspastic types of CP and hemiplegia were excluded, 92% of patients exhibited some degree of hip deformity. Lonstein and Beck further stratified this risk, finding that hip subluxation and dislocation occurred in 7% of ambulators but up to 60% of dependent sitters.
Radiographic Surveillance and the Migration Percentage
Because early hip subluxation in CP is typically painless and masked by severe contractures, clinical detection is notoriously difficult. Therefore, all hips in patients with cerebral palsy must be considered abnormal until proven otherwise. Routine clinical and radiographic screening should be performed every 6 months, particularly during periods of rapid growth and in patients with spastic quadriplegia. Radiographic changes typically become apparent between 2 and 4 years of age.
In 1969, Beals introduced a practical radiographic method for quantifying hip subluxation, which Reimers later popularized as the Migration Percentage (MP).
Radiographic Technique: Careful patient positioning is critical. The patient must be supine, hips neutral and together, with the patellae facing strictly forward to neutralize the effect of anteversion. The measurement error for an experienced observer is approximately 5 degrees.
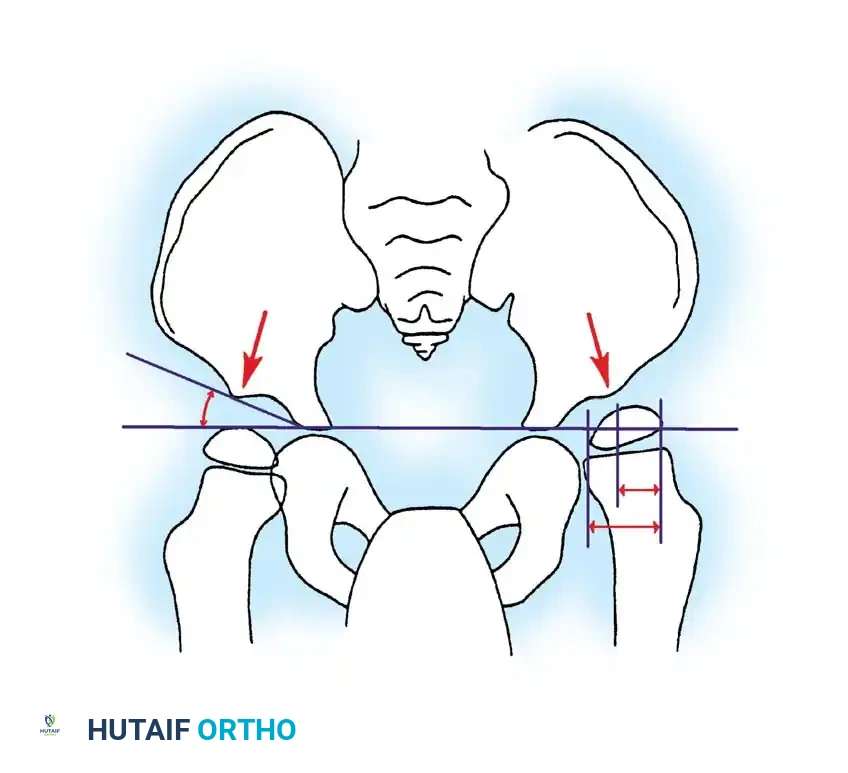
The migration percentage is calculated by drawing Hilgenreiner's line (connecting the bilateral triradiate cartilages) and dropping perpendicular lines (Perkins' lines) at the lateral margins of the ossified acetabular sourcil. The width of the femoral head uncovered (lateral to Perkins' line) is divided by the total width of the femoral head and multiplied by 100.
* Normal: MP < 33%
* Subluxation: MP 33% – 99%
* Dislocation: MP 100%
More critical than a single absolute value is the velocity of change observed within a given patient over time.
Flexion Deformities and Gait Kinematics
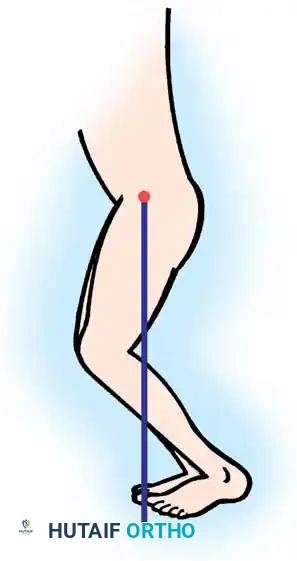
Crouched gait—characterized by excessive flexion of the hip, knee, and ankle—is a hallmark of spastic diplegia and quadriplegia. Excessive hip flexion shifts the center of gravity anteriorly, which the patient compensates for by increasing lumbar lordosis, flexing the knees, and dorsiflexing the ankles.
It is imperative to differentiate whether increased hip flexion is a primary deformity or a secondary kinematic compensation for distal contractures (e.g., fixed knee flexion).
Surgical Warning: If an unrecognized fixed knee flexion contracture is present, an isolated hip flexor release will paradoxically weaken the hip, exacerbate the anterior center of gravity shift, and ultimately worsen the crouch gait.
Pseudoadduction vs. True Adduction
A common source of clinical confusion is differentiating a flexion-internal rotation deformity ("pseudoadduction") from an isolated true adduction contracture. Children with pseudoadduction typically sit in the classic "W" position: hips flexed to 90 degrees and maximally internally rotated, knees maximally flexed, and feet externally rotated.

In pseudoadduction, secondary bony deformities such as increased femoral anteversion, external tibial torsion, and planovalgus feet are almost universally present. In a true isolated adduction contracture, these secondary torsional deformities are absent.
Adduction Deformities: Soft Tissue Management
Adduction is the most common primary deformity of the hip in children with CP. Severe adductor spasticity causes scissoring of the legs during the swing phase of gait, drives progressive lateral hip subluxation, and creates profound difficulties with perineal hygiene in dependent sitters.
For mild contractures, an isolated adductor longus tenotomy is sufficient. More severe contractures require the release of the gracilis and the anterior half of the adductor brevis. These procedures are almost always performed bilaterally to prevent the development of a "windswept" pelvis.
Indications for Soft-Tissue Release
The ideal candidate for isolated soft-tissue lengthening is a child younger than 8 years of age who exhibits:
* Hip abduction of less than 30 degrees in extension.
* A Migration Percentage (MP) between 25% and 60%.
While early soft-tissue release is highly beneficial, Turker and Lee demonstrated that at an 8-year follow-up, 58% of patients required a secondary bony procedure. Soft-tissue release often serves to delay major bony reconstruction until the child is older, the risk of recurrence is lower, and the pelvic bone stock is more robust.
### 🔪 Surgical Technique: Adductor Tenotomy and Release
Step 1: Positioning and Preparation
Place the patient supine on the operating table. Prepare and drape the lower extremities from the toes to the inferior costal margin, carefully isolating the perineum to allow full intraoperative range of motion.

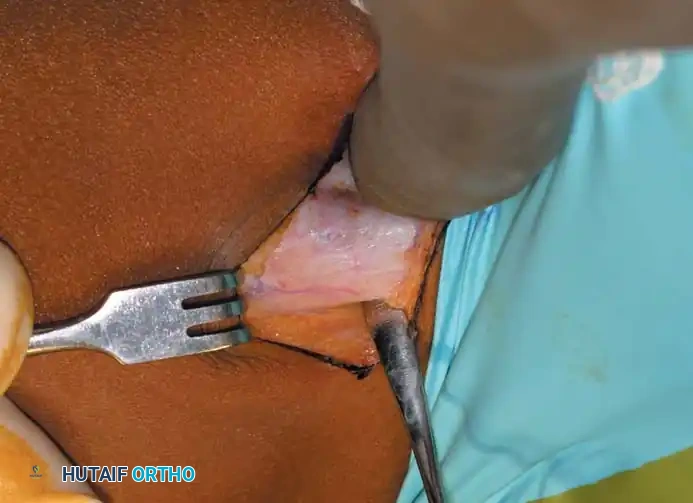
Step 2: Incision
Palpate the taut adductor longus tendon at its origin on the pubis. Make a 3-cm transverse incision centered over the tendon, approximately 1 cm distal to its origin.
Step 3: Fascial Dissection
Dissect bluntly through the subcutaneous adipose tissue to identify the underlying adductor fascia. Make a longitudinal incision in the fascia to expose the tendinous portion of the adductor longus.
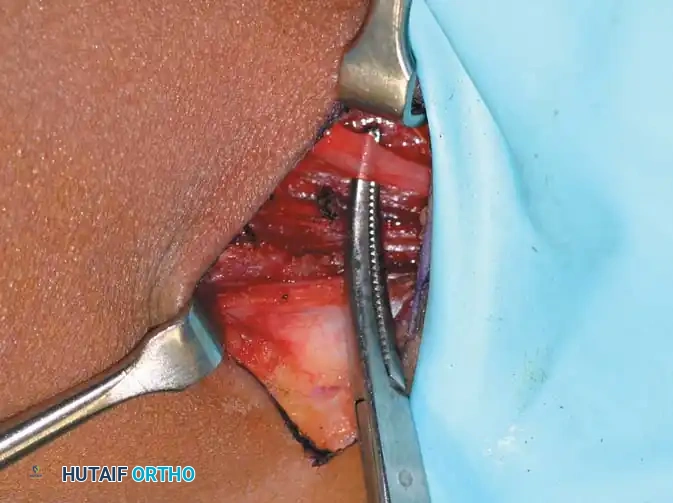
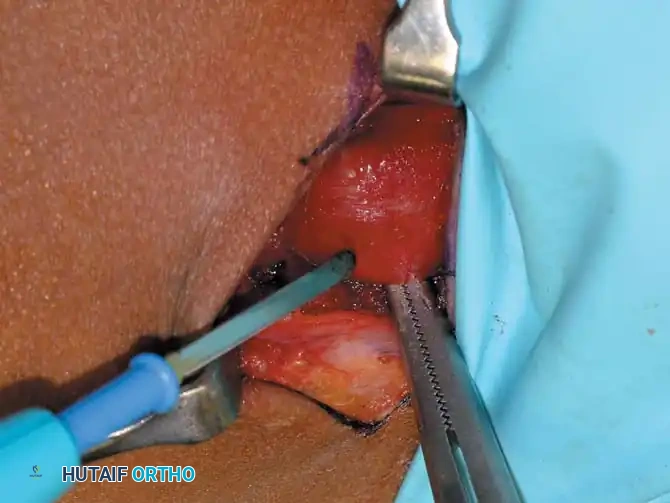
Step 4: Muscle Release
Isolate the adductor longus tendon and resect a small portion using electrocautery to prevent bridging. If the hip does not abduct to at least 45 degrees, sequentially release the gracilis and the anterior half of the adductor brevis.
Surgical Pitfall: Meticulously avoid injury to the anterior branch of the obturator nerve, which lies in the fascial interval between the adductor longus and adductor brevis. Do not perform an obturator neurectomy, as this frequently leads to an iatrogenic, irreversible abduction contracture.
Step 5: Closure
Once adequate abduction is achieved, irrigate the wound. Close the adductor fascia meticulously to prevent unsightly postoperative skin dimpling. Close the subcutaneous tissue and skin in a standard layered fashion.
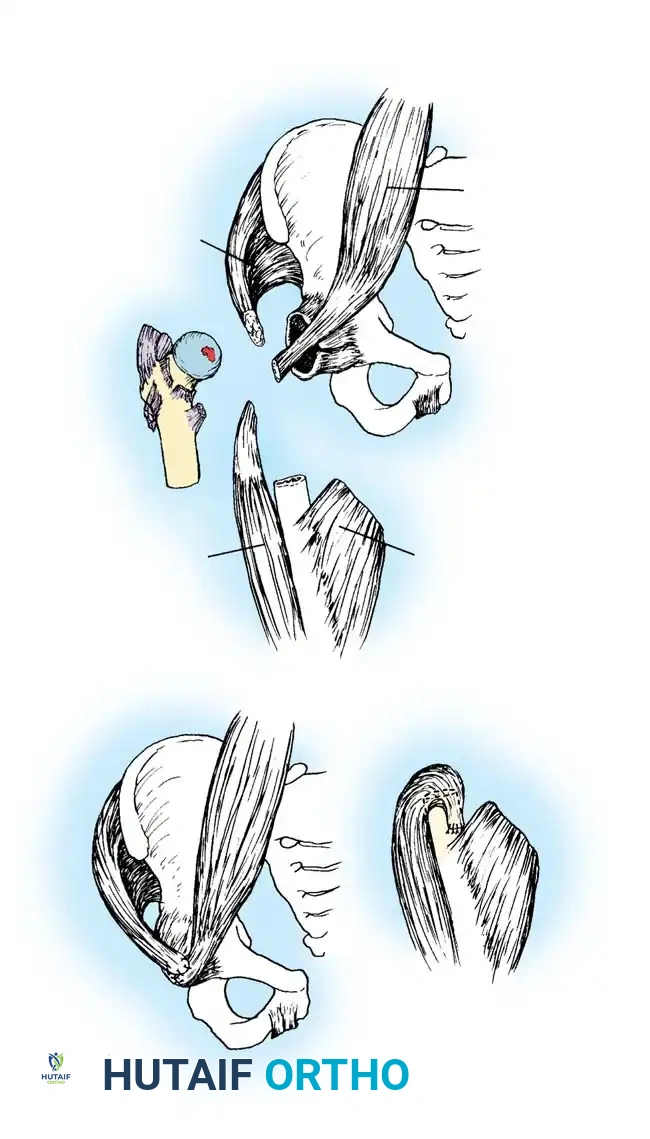
Management of Hip Flexion Contractures: Iliopsoas Recession
Hip flexion contractures between 15 and 30 degrees are typically managed with an iliopsoas lengthening via an intramuscular recession over the pelvic brim.
Clinical Pearl: In ambulatory children, a complete iliopsoas tenotomy at the lesser trochanter is contraindicated. It leads to profound hip flexion weakness, resulting in an inability to clear the foot during the swing phase of gait. Recession at the pelvic brim preserves sufficient strength for ambulation.
### 🔪 Surgical Technique: Iliopsoas Recession
Step 1: Approach
Place the patient supine with a bump under the ipsilateral buttock. Make a 5-cm "bikini" incision centered medial to and 2 cm distal to the anterior superior iliac spine (ASIS).
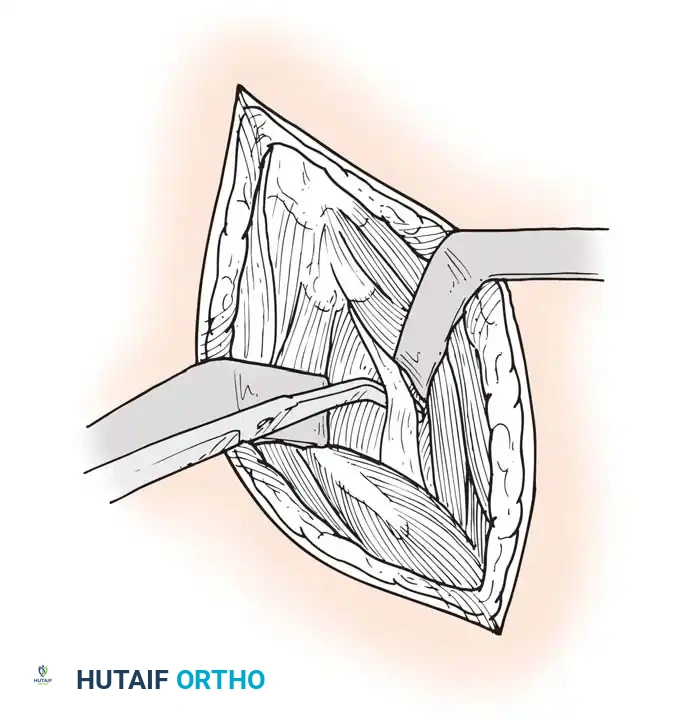
Step 2: Interval Development
Develop the internervous interval between the tensor fasciae latae (superior gluteal nerve) and the sartorius (femoral nerve). Expose the direct head of the rectus femoris at the anterior inferior iliac spine (AIIS).
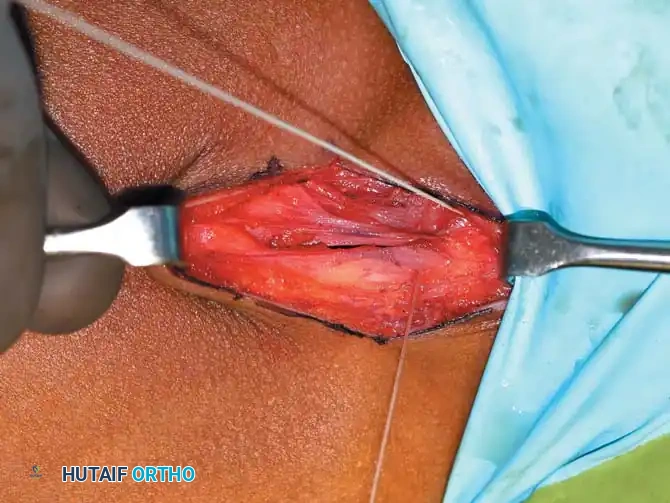
Step 3: Tendon Isolation
Palpate the pelvic brim medial and inferior to the rectus origin. The iliopsoas tendon lies in a shallow groove here. Flex the hip slightly to relax the anterior structures. Place a right-angle retractor on the lateral aspect of the iliopsoas muscle and retract medially to protect the femoral nerve.
Step 4: Recession
Isolate the tendinous portion of the psoas from the underlying muscle belly. Transect the tendon under direct vision, leaving the underlying muscle fibers intact to maintain continuity and preserve active hip flexion strength.
Bony Reconstruction: Pelvic Osteotomy
When soft-tissue releases fail, or when a child presents late with a Migration Percentage > 50% and severe acetabular dysplasia, bony reconstruction is mandatory. The goal is to restore the mechanical containment of the femoral head. In CP, the acetabular deficiency is typically global, but most pronounced posterosuperiorly.
The Dega or San Diego Pericapsular Osteotomy is the workhorse procedure for the spastic dysplastic hip. It is an incomplete transiliac osteotomy that hinges on the triradiate cartilage, allowing for multidirectional coverage of the femoral head.
### 🔪 Surgical Technique: Pericapsular Pelvic Osteotomy
Step 1: The Iliac Cut
Following a standard anterior approach to the hip and appropriate soft tissue releases, the inner and outer tables of the ilium are exposed. An incomplete osteotomy is initiated just above the AIIS and directed posteriorly toward the sciatic notch.
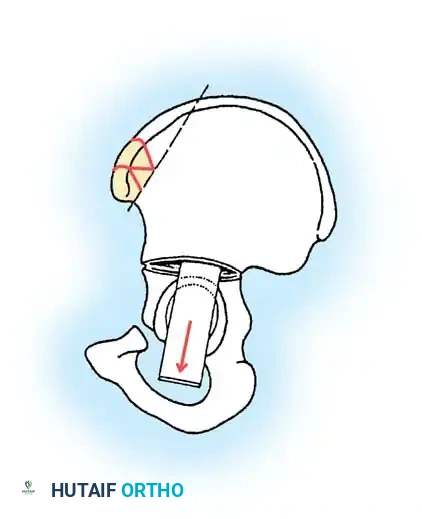
Step 2: Hinging the Osteotomy
The osteotomy is carefully advanced, leaving the medial cortex near the sciatic notch and the triradiate cartilage intact to act as a hinge.
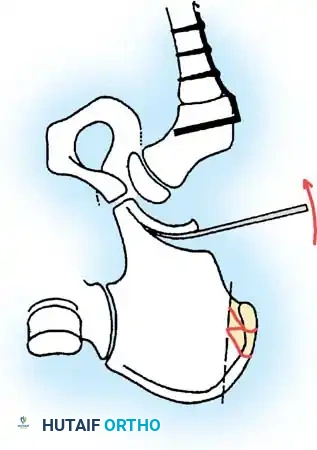
Step 3: Levering and Down-Grafting
Using a lamina spreader or a broad osteotome, the distal fragment (the acetabular roof) is levered laterally, anteriorly, and inferiorly to cover the femoral head.
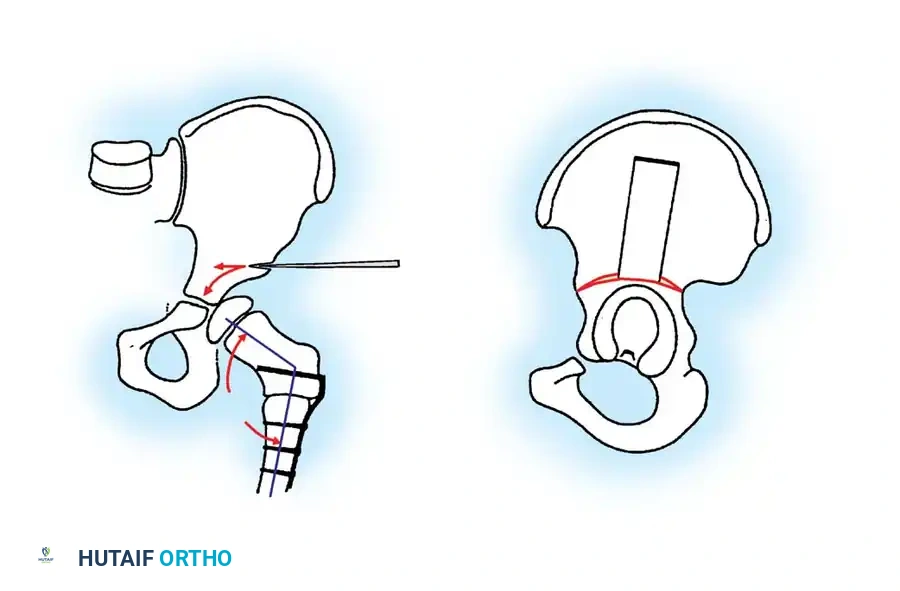
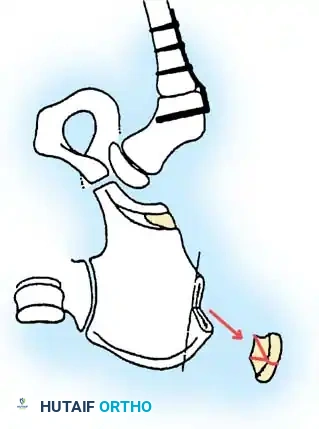
Step 4: Graft Preparation
Triangular or trapezoidal structural bone grafts are harvested from the proximal iliac crest.
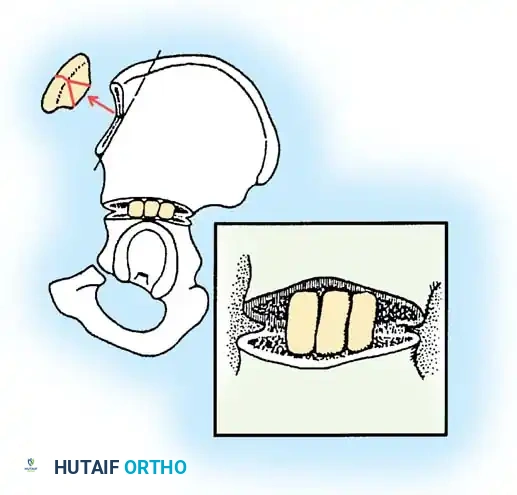
Step 5: Graft Placement
The structural grafts are impacted into the osteotomy gap. Because the osteotomy hinges on the flexible triradiate cartilage, the grafts are held firmly in place under compression without the need for internal hardware fixation.
Step 6: Final Assessment
The final construct provides robust, stable anterolateral and posterior coverage of the femoral head, dramatically improving the sourcil angle and normalizing the Migration Percentage.
Postoperative Protocols and Rehabilitation
Postoperative management is dictated by the extent of the surgical intervention and the patient's baseline functional status.
For isolated soft-tissue releases (adductor tenotomy and iliopsoas recession), patients are typically placed in a removable abduction pillow or A-frame orthosis. This allows for immediate, gentle physical therapy to maintain range of motion and prevent adhesive capsulitis.
For patients undergoing extensive bony reconstruction (pelvic osteotomies combined with femoral varus derotational osteotomies), a 1.5-spica cast is usually applied for 4 to 6 weeks to ensure rigid immobilization and graft incorporation. Following cast removal, aggressive physical therapy focuses on restoring baseline mobility, maximizing the newly acquired joint mechanics, and integrating the patient back into their functional ambulatory or sitting orthoses. Routine radiographic surveillance must continue until skeletal maturity to monitor for late recurrence.
You Might Also Like

