Advanced Orthopaedic Management of Adults with Cerebral Palsy and Post-Stroke Hemiparesis
Key Takeaway
The orthopaedic management of adults with cerebral palsy and post-stroke hemiparesis requires a nuanced understanding of spasticity, altered biomechanics, and progressive musculoskeletal deterioration. Treatment shifts from the pediatric focus of growth modulation to adult priorities: pain reduction, functional preservation, and hygiene optimization. Surgical interventions, including tendon lengthenings and joint reconstructions, must be meticulously timed and preceded by rigorous gait analysis and electromyography to ensure realistic, patient-centered outcomes.
Adults with Cerebral Palsy: Evolving Orthopaedic Challenges
The landscape of cerebral palsy (CP) management has undergone a profound transformation over recent decades. Tremendous advances in pediatric care, including early intervention, sophisticated rehabilitation, and judicious surgical strategies, have enabled a generation of children who historically would have faced institutionalization to be successfully integrated into families and society. This paradigm shift has led to an increasing population of adults living with CP, presenting a unique and evolving set of orthopaedic challenges that demand specialized understanding and management.
Unlike the pediatric population, where the focus is on growth modulation and the prevention of deformity, the adult CP patient presents with the sequelae of long-standing neuromuscular imbalance, failing compensatory mechanisms, and early-onset degenerative joint disease.
Epidemiology and Long-Term Outcomes in Adult CP
Despite the growing number of adults with CP, the long-term outcomes of treatment and the natural history of musculoskeletal issues in this population remain less comprehensively understood compared to pediatric CP. Population-based studies are gradually shedding light on the trajectory of function and independence.
- Functional Trajectory: Strauss et al. (2007) conducted a significant review of 904 adults with CP, revealing a marked decline in ambulation by age 60 among individuals who were mobile as young adults. This highlights the progressive nature of musculoskeletal deterioration and the eventual failure of compensatory mechanisms. Interestingly, other essential skills such as feeding, speech, and the ability to order meals in public were often well-preserved, suggesting a differential impact on various functional domains.
- Independence and Care Needs: The same study found that 18% of 60-year-olds with CP lived independently, while a substantial 41% resided in facilities providing higher levels of medical care. This underscores the diverse spectrum of independence and the varying support needs within the adult CP population.
- Survival Rates: Long-term survival rates in adults with CP are moderately worse than the general population, with non-ambulators experiencing a particularly reduced life expectancy. This emphasizes the systemic health challenges often associated with severe CP, including recurrent respiratory infections and compromised nutritional status.
- Socioeconomic Integration: Michelsen et al. (2005), in their review of 819 adults with CP, provided insights into educational and employment outcomes. They reported that 33% of patients had education beyond secondary school (compared to 77% of controls), and 29% were competitively employed (compared to 82% of controls). An additional 5% held specially created jobs. The study noted a higher rate of unemployment in patients with comorbidities such as seizures, but surprisingly, no substantial impact of the severity of motor involvement on employment rates. This suggests that cognitive abilities, communication skills, and societal support play crucial roles in vocational integration.
Common Orthopaedic Problems in Adults with CP
Many adults with CP present for orthopaedic care in their 30s and 40s as the compensatory mechanisms developed during childhood and adolescence begin to fail. The chronic biomechanical stresses, altered muscle tone, and increased body mass lead to a predictable pattern of degenerative changes and deformities.
- Degenerative Hip Disease: Hip subluxation or dislocation, a common issue in pediatric CP, can progress to severe osteoarthritis in adulthood, even in hips that were previously deemed stable. Abnormal muscle forces (e.g., adductor and flexor spasticity) contribute to joint incongruity, edge-loading, and accelerated cartilage wear. Total Hip Arthroplasty (THA) in this population is technically demanding due to altered proximal femoral anatomy (excessive anteversion, coxa valga), poor bone stock, and a high risk of postoperative dislocation requiring dual-mobility or constrained components.
- Knee Instability and Genu Recurvatum: Often arises secondary to long-standing ankle equinus. The persistent plantarflexion at the ankle creates a plantarflexion-knee extension couple. To maintain the center of gravity over the base of support during the stance phase, the patient compensates with knee hyperextension (genu recurvatum). Over time, this places abnormal stress on the posterior knee capsule and cruciate ligaments, eventually leading to painful instability and early patellofemoral osteoarthritis.
- Flatfoot Deformity (Pes Planovalgus): Chronic muscle imbalance, particularly weakness of the invertors (tibialis posterior) and dorsiflexors combined with spasticity of the evertors (peroneals) and plantarflexors (gastrocnemius-soleus complex), leads to progressive collapse of the medial longitudinal arch. This results in painful, rigid flatfoot deformities, often accompanied by midfoot abduction and forefoot supination.
- Spinal Deformity: Neuromuscular scoliosis is prevalent in CP and often progresses into adulthood, especially in non-ambulatory individuals (GMFCS levels IV and V). Progressive curves can lead to significant pelvic obliquity, seating difficulties, intractable back pain, and compromise of cardiopulmonary function.
- Osteopenia and Fragility Fractures: Disuse osteopenia is frequently observed in adults with CP, particularly in those with limited mobility and minimal weight-bearing status. Nutritional deficits and long-term use of antiepileptic medications further exacerbate poor bone mineral density, predisposing these patients to low-energy fragility fractures, most commonly of the distal femur or proximal tibia.
Principles of Management for Adults with CP
A patient-centered approach, mirroring the philosophy in pediatric CP, is paramount. The goals of intervention must be realistic and aligned with the patient's functional aspirations and overall quality of life.
- Functional Focus: Not all deformities require treatment. Attention should be primarily focused on deformities that cause pain, interfere with independent function (e.g., transfers, ambulation), or significantly compromise hygiene or ease of nursing care.
- Multidisciplinary Team: Management requires a cohesive multidisciplinary team including orthopaedic surgeons, neurologists, physiatrists, physical and occupational therapists, orthotists, and social workers.
- Realistic Expectations: It is crucial to manage patient and caregiver expectations regarding the potential outcomes of surgical or non-surgical interventions. Complete restoration of normal kinematics is rarely achievable.
- Non-Surgical Interventions: Custom orthotics (AFOs, KAFOs), specialized seating systems, physical therapy, botulinum toxin injections, and oral medications for spasticity management (e.g., baclofen, tizanidine) are the first line of treatment.
- Surgical Considerations: Surgical intervention is typically reserved for cases where non-surgical measures have failed to alleviate pain, improve function, or prevent further rapid deterioration.
Clinical Pearl: In adult CP, the surgical paradigm shifts from prophylactic growth modulation to salvage procedures. Degenerative changes are often irreversible, making pain control, joint stabilization (often via arthrodesis), and functional preservation the primary goals.
Adult Stroke Patients: Orthopaedic Evaluation and Treatment
Cerebrovascular accidents (CVAs), or strokes, represent a leading cause of long-term disability worldwide. With advancements in acute stroke care, the incidence of survival is rising, leading to a growing population of individuals living with residual neurological deficits, primarily hemiparesis. Orthopaedic surgeons play a critical role in addressing the musculoskeletal sequelae that significantly impact mobility, independence, and quality of life. Pioneers such as Perry, Nickel, and Waters have made foundational contributions to our understanding of the orthopaedic evaluation and treatment of the spastic hemiparetic patient.
Lower Extremity Management in Stroke Patients
Approximately 65% to 75% of stroke patients recover sufficient lower extremity function to permit ambulation. This higher recovery rate compared to the upper extremity is attributed to several factors:
* Reduced Sensory Dependence: The lower extremity relies less on fine tactile sensation and proprioception for its primary function (ambulation) than the upper extremity does for prehension.
* Gross Motor Functions: Activities necessary for walking are largely gross motor functions, which are more easily driven by primitive reflex arcs.
* Primitive Postural Reflexes: These reflexes, often enhanced in the presence of spasticity, can be harnessed to contribute to basic, albeit pathological, ambulation patterns.
Most patients with residual hemiparesis will initially require external support (e.g., hemi-walker, quad cane) and orthotic bracing to achieve independent ambulation.
Early Phase Management (Acute to Subacute)
The primary goal in the early phases of recovery is the prevention of fixed myostatic contractures and the establishment of proper limb positioning.
* Orthotic Positioning: Early application of rigid ankle-foot orthoses (AFOs) or resting splints helps maintain the ankle in a neutral position, preventing the ubiquitous equinus deformity caused by gastrocnemius-soleus overactivity.
* Range-of-Motion (ROM) Exercises: Aggressive passive and active-assisted ROM exercises are crucial to prevent capsular contractures and maintain joint mobility.
* Early Mobilization: Encouraging the patient to stand and walk as soon as medically stable is vital for preventing deep vein thrombosis, improving pulmonary toilet, and facilitating neuroplastic motor recovery.
* Electrical Stimulation: Functional electrical stimulation (FES) can be utilized to maintain muscle bulk, mobilize joints, and serve as a sensorimotor educational tool to increase cortical awareness of muscle contractions.
Motor Recovery and Gait Training
Motor recovery typically occurs most rapidly during the first 3 to 4 months post-stroke. To become a functional ambulator, patients require adequate spontaneous neurological recovery to allow voluntary, selective control of the hip and knee.
* Definitive Bracing: Once maximal motor recovery has been achieved and the gait pattern has stabilized (typically 6 to 9 months post-stroke), a definitive custom brace should be prescribed. This brace must effectively control the specific gait defect (e.g., a solid AFO for severe drop foot and spasticity, or an articulated AFO if selective dorsiflexion is partially preserved).
Neurophysiology of Stroke Gait (Perry et al.)
Dr. Jacquelin Perry significantly advanced the understanding of neurophysiology in both normal individuals and stroke patients, identifying distinct neurological sources of motion that dictate the hemiparetic gait pattern:
- Sophisticated Components of Normal Function:
- Selective Control: The normal ability to move one joint independently of another, or to contract an isolated muscle. This is often severely impaired or absent in stroke.
- Habitual Control: The automatic performance of learned skills, such as walking, originating from the basal ganglia and cerebellum. This automaticity is disrupted, requiring the patient to exert immense conscious effort to walk.
- Primitive Controls (Overt in Spastic Patients): These are normally suppressed by higher cortical centers but become overtly expressed when upper motor neuron inhibition is lost.
- Locomotor Pattern (Mass Synergy): Mass movements of flexion and extension. Patients can initiate these movements but cannot modify them. For example, in the extensor synergy, knee extension is obligatorily coupled with ankle plantarflexion and hip extension.
- Control of Verticality: Extensor muscles exhibit increased tone when the body is erect compared to supine. Standing provides a massive proprioceptive stimulus that exacerbates extensor spasticity in the lower extremity.
- Primitive Limb Synergy: A multisegmental spinal cord reflex linking extensor muscle action to limb posture. When the knee is extended, the tone of the triceps surae significantly increases. This phenomenon confounds the Silfverskiöld test, which is used to differentiate isolated gastrocnemius contracture from combined gastrocnemius-soleus contracture.
- Fast Stretch Reflex: Characterized by clonus—an intermittent burst of muscle activity initiated by velocity sensors (muscle spindles) when a muscle is stretched rapidly.
- Slow Stretch Reflex: Characterized by lead-pipe or clasp-knife rigidity, a continuous muscle reaction to stretch often misinterpreted as a fixed structural contracture.
Pitfall: Misinterpreting the slow stretch reflex (dynamic spasticity) as a fixed myostatic contracture can lead to inappropriate and overly aggressive surgical lengthening. A thorough examination, potentially including diagnostic nerve blocks or examination under anesthesia, is crucial to differentiate the two.
Pre-Surgical Evaluation and Timing
Surgical decision-making in the stroke population must be meticulous. Visual observational gait analysis, combined with dynamic kinesiologic electromyography (EMG), is the gold standard for determining which muscles are firing inappropriately during the gait cycle.
- Timing of Surgery: Orthopaedic surgical intervention should strictly be deferred until at least 6 months, and ideally 9 to 12 months, after the stroke. By this time, spontaneous neurological recovery has plateaued, and the patient's neurological baseline is established. Operating during the phase of active neurological recovery can lead to unpredictable and often disastrous functional outcomes.
- Patient Expectations: The surgeon must have a frank discussion with the patient and family. Restoration of a "normal" gait is impossible. The goals are strictly functional: improving brace tolerance, enhancing stability, reducing energy expenditure, and alleviating pain.
Specific Lower Extremity Surgical Management
Surgical procedures in the adult CP and stroke populations predominantly involve soft-tissue rebalancing (tendon lengthenings, releases, and transfers) and, less frequently, corrective osteotomies or arthrodeses for rigid deformities.
Hip: Management of Scissoring Gait
Adductor Spasticity and Contracture
- Indication: A scissoring gait pattern caused by severe spasticity or contracture of the hip adductors. This leads to a narrow base of support, impaired balance, difficulty with perineal hygiene, and interference with catheterization or dressing.
- Diagnostic/Therapeutic Nerve Block: Before considering surgical release, a diagnostic block of the obturator nerve using a local anesthetic (e.g., bupivacaine) is mandatory. If the block resolves the scissoring and improves passive abduction, the deformity is primarily driven by dynamic spasticity, and the patient may benefit from a neurectomy or botulinum toxin. If abduction remains restricted, a fixed myostatic contracture is present, necessitating surgical release.
Surgical Technique: Open Adductor Tenotomy and Obturator Neurectomy
- Positioning: The patient is placed supine on the operating table. The affected hip is flexed, abducted, and externally rotated (frog-leg position) to place the adductor musculature under maximal tension.
- Incision: A 4 to 5 cm longitudinal incision is made over the medial aspect of the proximal thigh, centered over the palpable cord of the adductor longus tendon, originating just inferior to the pubic tubercle.
- Superficial Dissection: The subcutaneous tissue is divided, taking care to identify and protect branches of the external pudendal vessels.
- Tendon Release: The adductor longus tendon is isolated and transected near its origin at the pubis. If severe contracture persists, the gracilis and the anterior fibers of the adductor brevis are sequentially identified and released.
- Obturator Neurectomy (Optional): If dynamic spasticity is a major component, the anterior branch of the obturator nerve, found resting on the anterior surface of the adductor brevis, can be identified, ligated, and resected (removing a 1-2 cm segment to prevent neuroma formation and reinnervation).
- Closure and Postoperative Care: The wound is closed in layers. Postoperatively, the patient is placed in an abduction pillow or a custom A-frame orthosis for 3 to 4 weeks to maintain the newly acquired abduction range while soft tissues heal.
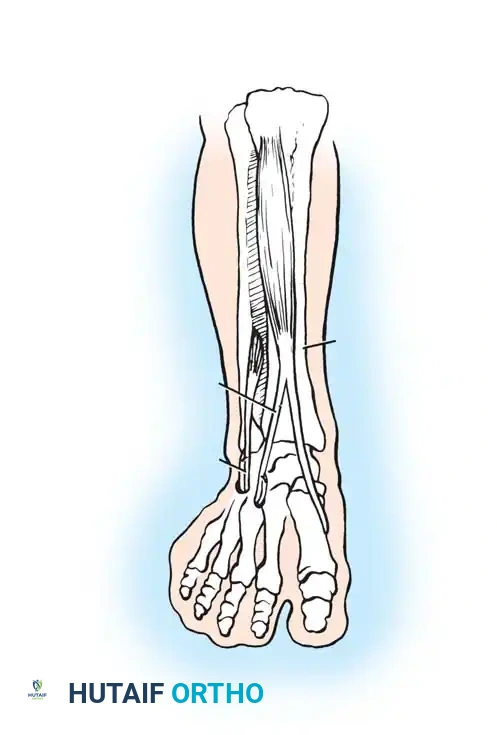
Foot and Ankle: Management of Equinovarus Deformity
Equinovarus is the most common foot deformity in both adult CP and post-stroke hemiparesis. It is characterized by plantarflexion (equinus) driven by the gastrocnemius-soleus complex, and inversion (varus) driven by an overactive tibialis anterior or tibialis posterior.
Surgical Technique: Achilles Lengthening and SPLATT Procedure
When dynamic EMG confirms that the tibialis anterior is firing continuously or inappropriately during the stance phase, causing the foot to supinate and invert, a Split Anterior Tibial Tendon Transfer (SPLATT) combined with Achilles lengthening is highly effective.
- Achilles Lengthening: Depending on the severity of the contracture, either a percutaneous Hoke triple hemisection or an open Z-lengthening of the Achilles tendon is performed to restore neutral ankle dorsiflexion. Care must be taken not to over-lengthen, which would result in a devastating calcaneal gait and profound weakness.
- SPLATT Incisions:
- Incision 1: Made over the insertion of the tibialis anterior at the medial cuneiform and base of the first metatarsal.
- Incision 2: Made over the anterior distal third of the leg, at the musculotendinous junction of the tibialis anterior.
- Incision 3: Made over the lateral midfoot, typically targeting the cuboid or the base of the third/fourth metatarsal.
- Tendon Splitting and Routing: The tibialis anterior tendon is split longitudinally from its insertion up to the musculotendinous junction. The lateral half of the split tendon is detached from its insertion, passed subcutaneously across the anterior ankle, and routed to the lateral midfoot incision.
- Fixation: The transferred lateral slip is anchored into the cuboid or lateral cuneiform using a biotenodesis screw or suture anchor, with the foot held in neutral dorsiflexion and slight eversion. This converts the deforming supinatory force of the tibialis anterior into a corrective, balanced dorsiflexion force.
- Postoperative Protocol: The patient is placed in a well-padded short leg cast in neutral alignment. Weight-bearing is strictly restricted for 6 weeks to allow for robust tendon-to-bone healing. Following cast removal, the patient transitions to a solid AFO and begins intensive physical therapy focusing on gait retraining and strengthening.
Surgical Warning: In the spastic patient, tendon transfers are rarely expected to function with normal voluntary, phasic control. Instead, they act as dynamic tenodeses. The primary goal of the SPLATT is to remove the deforming varus force and provide a balanced tether to maintain a plantigrade foot during the swing phase and initial contact.
You Might Also Like


