Operative Management of Proximal & Middle Phalanx Fractures
Key Takeaway
Proximal and middle phalangeal fractures frequently result from direct dorsal trauma, leading to characteristic volar angulation and claw deformity due to intrinsic and extrinsic muscle forces. Operative intervention is indicated for open, multiple, or irreducible fractures. Surgical management utilizes precise dorsal or dorsolateral approaches, employing minifragment screws, Kirschner wires, or Pratt’s technique to achieve anatomic reduction, restore articular congruity, and permit early mobilization for optimal functional recovery.
INTRODUCTION TO PHALANGEAL FRACTURES
Fractures of the proximal and middle phalanges are among the most frequently encountered skeletal injuries in orthopedic hand trauma. While many of these fractures can be managed non-operatively with precise closed reduction and protective splinting, a significant subset demands meticulous surgical intervention. A direct blow on the dorsum of the fingers is the most common etiology, often resulting in transverse, oblique, or comminuted fracture patterns.
The primary goal of operative management is to achieve stable anatomic reduction that permits early active mobilization. The hand is an unforgiving anatomic region; prolonged immobilization inevitably leads to tendon adhesions, joint contractures, and profound functional impairment. Therefore, the modern orthopedic surgeon must possess a deep understanding of phalangeal biomechanics, surgical anatomy, and advanced internal fixation techniques to optimize patient outcomes.
BIOMECHANICS AND PATHOANATOMY
Understanding the deforming forces acting upon the phalanges is critical for both closed reduction and surgical fixation. The proximal phalanx is uniquely vulnerable because it lacks direct tendinous insertions along its shaft, acting instead as an intercalated bone segment suspended between the complex intrinsic and extrinsic muscle systems.
When a fracture occurs in the proximal or middle phalanx, the predictable displacement pattern is volar apex angulation. This occurs due to a combination of forces:
* Proximal Fragment: The interosseous muscles, which insert onto the base of the proximal phalanx, exert a strong flexion force.
* Distal Fragment: The central slip of the extensor mechanism, inserting on the base of the middle phalanx, exerts an extension force.
This biomechanical tug-of-war results in the characteristic volar angulation, and the fingers may assume a pathognomonic "claw" position.
FIGURE 67-43: Biomechanical representation of deforming forces. Full flexion of the metacarpophalangeal (MCP) joint is required to relax these deforming intrinsic forces and maintain reduction.
Clinical Pearl: To neutralize the deforming forces during closed reduction or provisional surgical pinning, the metacarpophalangeal (MCP) joint must be placed in 70 to 90 degrees of flexion. This "intrinsic plus" position maximizes the tension on the collateral ligaments and relaxes the interossei, facilitating alignment of the fracture fragments.
INDICATIONS FOR SURGICAL INTERVENTION
While undisplaced or stable fractures are amenable to conservative care, surgical stabilization is strictly indicated under the following conditions:
* Multiple Fractures: To restore the structural cascade of the hand and permit early rehabilitation.
* Open Fractures: Requiring meticulous debridement and rigid stabilization to prevent infection and promote soft tissue healing.
* Intra-articular Fractures: Displaced fractures involving the MCP or proximal interphalangeal (PIP) joints require anatomic reduction to prevent post-traumatic osteoarthritis.
* Rotational Malalignment: Even minor rotational deformities (e.g., scissoring of the digits during flexion) are poorly tolerated and mandate operative correction.
* Unstable Fracture Patterns: Short oblique, spiral, or comminuted fractures that lose reduction in a cast or splint.
SURGICAL APPROACHES TO THE PHALANGES
The choice of surgical approach is dictated by the fracture pattern, the planned fixation construct, and the necessity to minimize trauma to the delicate extensor apparatus.
The Dorsolateral Approach
The dorsolateral approach provides excellent exposure for diaphyseal fractures while minimizing direct injury to the central slip. The incision is placed along the mid-axial line, dorsal to the neurovascular bundle. The transverse retinacular ligaments are incised, allowing the extensor mechanism to be elevated dorsally. This approach is highly favored for placing lateral plates or interfragmentary screws.
The Dorsal Approach
For complex proximal phalangeal fractures, particularly those with intra-articular extension, a direct dorsal approach is often required.
Surgical Warning: A straight longitudinal incision over the dorsum of the digit must be strictly avoided, as it predictably leads to severe scar contracture and limits finger flexion.
Instead, the incision should extend from the metacarpophalangeal joint to the proximal interphalangeal joint in a gentle "S" curve. Once the skin flaps are elevated, the extensor mechanism is exposed. The surgeon may choose to split the extensor tendon longitudinally (splitting the central slip) or utilize a tendon-sparing approach by elevating the lateral bands, depending on the exact location of the fracture.
OPERATIVE TECHNIQUES AND FIXATION STRATEGIES
Technique 1: Minifragment Screw Fixation for Intra-articular Fractures
Displaced intra-articular fractures of the proximal phalanx base are challenging injuries that compromise the congruity of the MCP joint. Rigid internal fixation using minifragment screws (typically 1.0 mm to 1.5 mm) is the gold standard for achieving anatomic articular reduction.
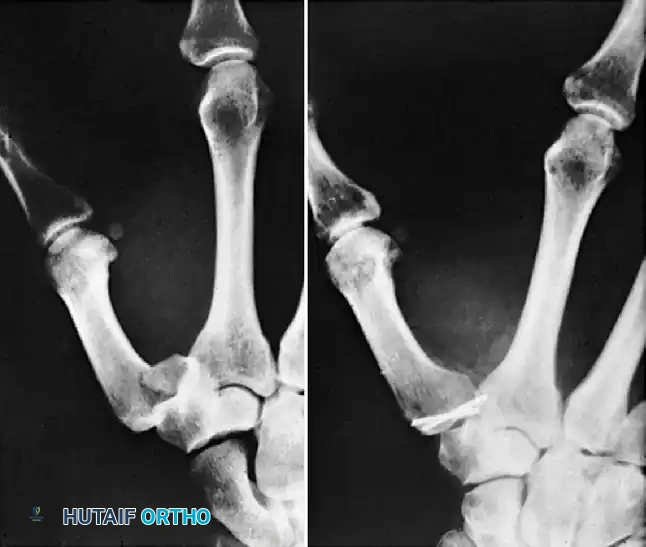
Case Example: Three-Part Displaced Intra-articular Fracture
Preoperative Evaluation:
The following radiographs demonstrate a complex, three-part displaced intra-articular fracture of the proximal phalanx in a 27-year-old man. The articular surface is significantly disrupted, necessitating open reduction.

FIGURE 67-41 A: Preoperative anteroposterior radiograph demonstrating the intra-articular split.

FIGURE 67-41 B: Preoperative oblique radiograph highlighting the displacement and articular step-off.
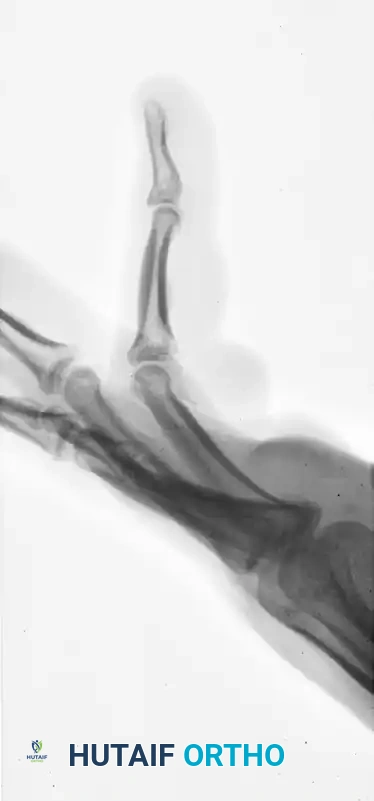
FIGURE 67-41 C: Preoperative lateral radiograph showing the volar subluxation tendency.
Surgical Execution:
1. Exposure: A dorsal S-shaped incision is utilized. The joint capsule is opened to directly visualize the articular surface.
2. Reduction: The articular fragments are meticulously reduced using dental picks and provisional 0.028-inch Kirschner wires.
3. Fixation: Minifragment lag screws are placed to compress the articular fragments. It is imperative that the screws are placed perpendicular to the fracture plane to achieve maximum interfragmentary compression.
Pitfall: The collateral ligaments of the MCP joint glide over the base of the proximal phalanx during flexion and extension. If screw heads are left prominent, they will impinge on the collateral ligaments, leading to severe postoperative stiffness and pain.
Postoperative Result:
The screw heads must be countersunk or carefully selected to ensure a low profile. The following radiographs demonstrate successful anatomic reduction and fixation.

FIGURE 67-41 D: Postoperative AP radiograph showing anatomic restoration of the joint line.

FIGURE 67-41 E: Postoperative oblique radiograph confirming flush seating of the minifragment screws.

FIGURE 67-41 F: Postoperative lateral radiograph demonstrating restoration of the sagittal alignment. Note that the small screw heads do not interfere with collateral ligament function.
Technique 2: Pratt’s Technique for Phalangeal Shaft Fractures
While many diaphyseal fractures can be managed with closed reduction and percutaneous pinning, rare phalangeal shaft fractures require open reduction due to soft tissue interposition or severe comminution. In these instances, Pratt’s technique offers a reliable method for intramedullary stabilization using Kirschner wires and monofilament wire loops.
Step-by-Step Execution of Pratt's Technique:
-
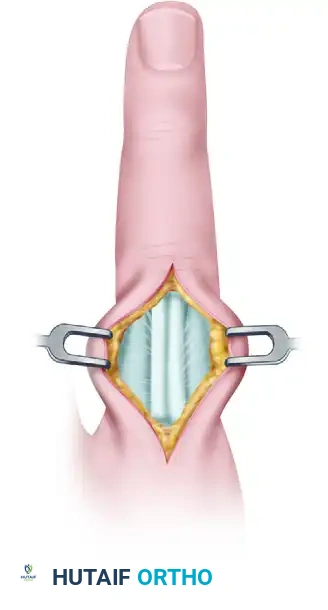
Incision and Exposure: A dorsal approach is utilized. The skin is incised, and the subcutaneous tissues are carefully dissected to expose the extensor mechanism.
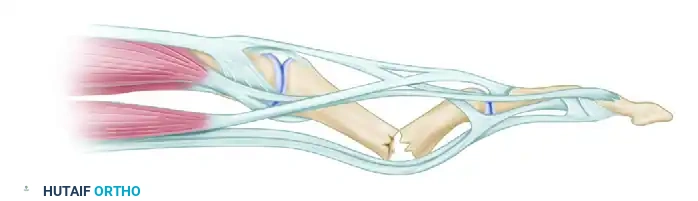
FIGURE 67-44 A: Initial dorsal exposure of the extensor mechanism over the fractured phalanx. -
Tendon Incision: The extensor mechanism is longitudinally incised precisely in the midline to expose the underlying fracture site. Care must be taken to avoid damaging the delicate periosteum more than necessary.
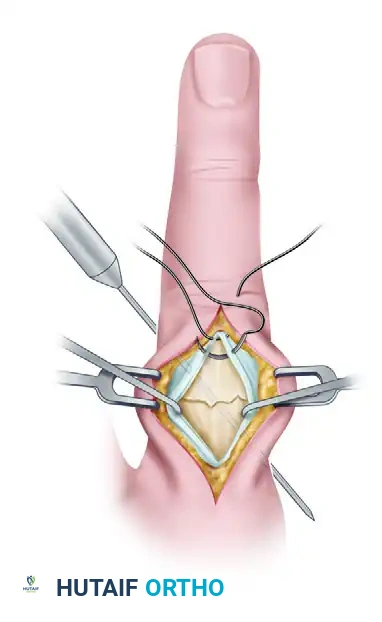
FIGURE 67-44 B: The extensor mechanism is incised, revealing the displaced phalangeal shaft fracture. -
Intramedullary Drilling and Pinning: The fracture is anatomically reduced. A Kirschner wire (typically 0.035 or 0.045 inch) is introduced into the medullary canal. Depending on the fracture pattern, crossed K-wires or a single stout intramedullary wire may be used. The wire is driven using a power drill to ensure precise placement without displacing the fracture fragments.

FIGURE 67-44 C: A Kirschner wire is drilled across the fracture site to provide longitudinal and rotational stability. -
Closure and Supplemental Fixation: Once skeletal stability is achieved, the extensor mechanism must be meticulously repaired. A monofilament wire or strong non-absorbable suture is used to close the extensor split. This repair must be robust enough to withstand early active motion protocols.
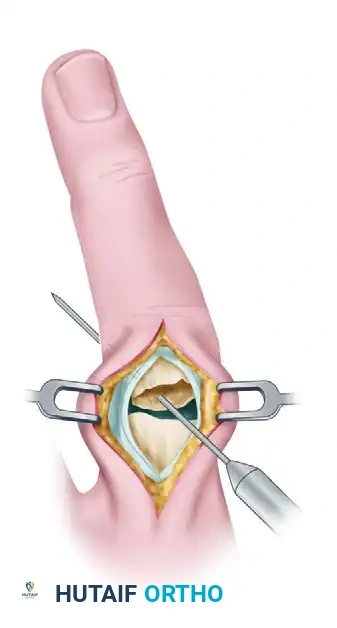
FIGURE 67-44 D: Final closure of the extensor mechanism over the stabilized fracture using monofilament wire.
Adjunctive Principles: Metacarpal Shaft Fixation
The biomechanical principles applied to phalangeal fractures are frequently extrapolated to metacarpal shaft fractures. When dealing with long oblique or spiral fractures of the metacarpals, interfragmentary lag screw fixation is highly effective. However, the metacarpals are subjected to significant sagittal bending moments during grip.
To counteract these forces, supplemental fixation is often required. The following case illustrates the use of lag screws augmented by cerclage wiring in a 75-year-old woman with middle and ring metacarpal shaft fractures.
Preoperative Imaging:

FIGURE 67-42 A: Preoperative AP radiograph showing shortened and oblique middle and ring metacarpal fractures.

FIGURE 67-42 B: Preoperative oblique radiograph demonstrating the fracture geometry, which is highly suitable for interfragmentary fixation.
Postoperative Imaging:
The fractures were reduced anatomically. Lag screws were placed to provide interfragmentary compression. To neutralize the sagittal bending moment—particularly in the ring metacarpal—a supplemental 24-gauge cerclage wire was applied.

FIGURE 67-42 C: Postoperative AP radiograph showing anatomic reduction and rigid fixation.

FIGURE 67-42 D: Postoperative oblique radiograph. Note that the sagittal bending moment of the ring metacarpal shaft fracture was successfully offset by the supplemental 24-gauge cerclage wire fixation.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The ultimate success of phalangeal fracture fixation is dictated not only by the surgery but by the postoperative rehabilitation. The primary enemy of hand surgery is stiffness caused by tendon adhesions.
Phase 1: Immediate Postoperative Period (Days 1-5)
* The hand is placed in a bulky, compressive dressing with a volar plaster splint.
* The wrist is extended to 30 degrees, the MCP joints are flexed to 70-90 degrees (intrinsic plus position), and the PIP/DIP joints are left fully extended.
* Strict elevation is mandated to minimize edema, which is a primary catalyst for fibrosis.
Phase 2: Early Active Motion (Days 5-21)
* If rigid internal fixation (e.g., lag screws or plates) was achieved, the bulky dressing is removed, and a custom thermoplastic splint is fabricated.
* Active range of motion
You Might Also Like