Operative Management of Phalangeal Fractures and PIP Joint Fracture-Dislocations
Key Takeaway
Proximal and middle phalangeal fractures often present with volar angulation due to intrinsic muscle forces. Operative management ranges from percutaneous Belsky-Eaton pinning to rigid internal fixation using lag screws or minicondylar plates. For PIP joint fracture-dislocations, treatment is dictated by the articular involvement size, utilizing extension block splinting for smaller fragments and volar plate arthroplasty or hemihamate grafts for larger, unstable defects.
Introduction to Phalangeal Fractures
Fractures of the phalanges are among the most common skeletal injuries encountered in orthopedic and hand surgery. While many can be managed nonoperatively, unstable, displaced, or intraarticular fractures demand precise surgical intervention to restore the intricate biomechanical balance of the hand. The middle and proximal phalanges are particularly susceptible to direct blows on the dorsum of the fingers or axial loading combined with torsional forces.
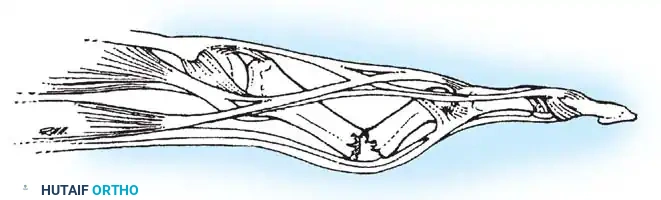
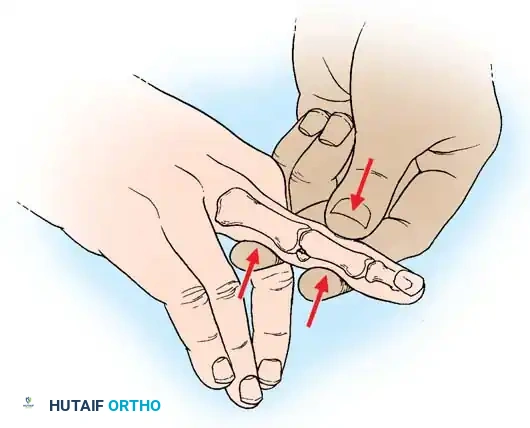
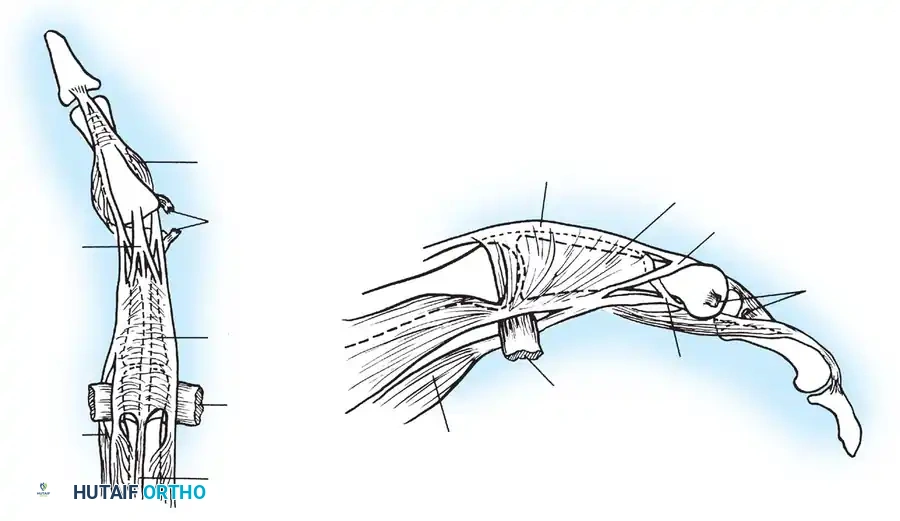
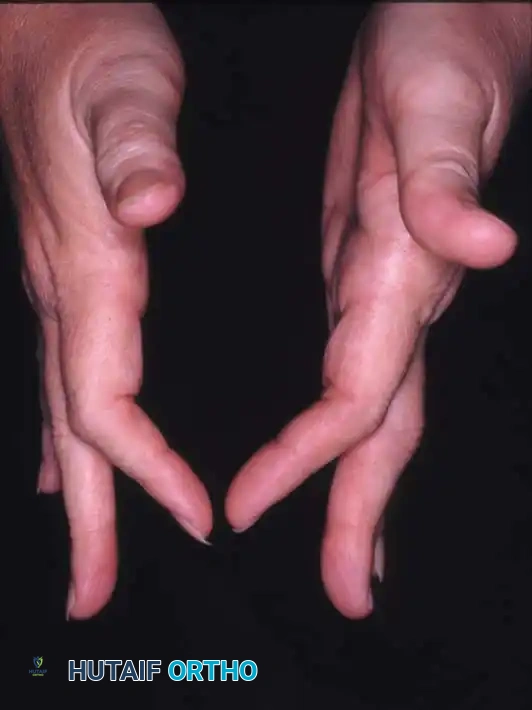
Understanding the deforming forces is paramount. In proximal phalanx fractures, the intrinsic muscles (interossei and lumbricals) flex the proximal fragment, while the central slip of the extensor mechanism extends the distal fragment. This predictably results in volar angulation (apex volar), causing the fingers to assume a claw position.
Clinical Pearl: Full flexion of the metacarpophalangeal (MCP) joint to 70–90 degrees is required to relax the deforming intrinsic forces, tighten the collateral ligaments, and maintain anatomical reduction during both closed and open management.
Fractures of the Middle and Proximal Phalanx
When multiple digits are involved, or when fractures are open, highly comminuted, or associated with soft-tissue loss, operative stabilization is mandatory. The goal is to achieve skeletal stability that permits early active range of motion (ROM), thereby preventing the dreaded complication of tendon adhesion and joint stiffness.
Surgical Approaches
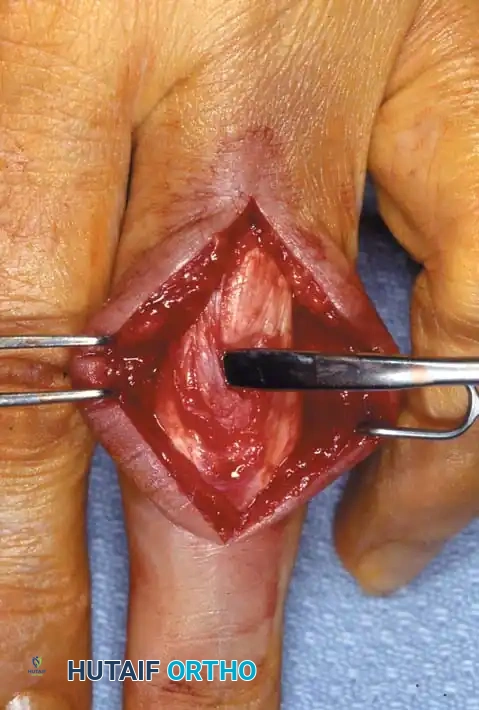
The approach to the proximal and middle phalanges must respect the delicate extensor hood mechanism.
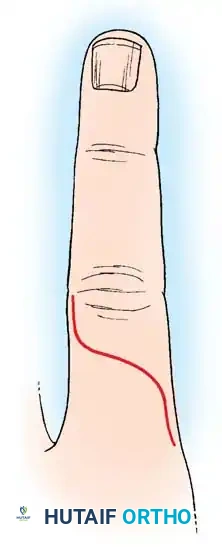
- Longitudinal Dorsolateral Incision: Placed between the lateral band and the central slip, offering excellent exposure of the diaphysis while minimizing scarring directly over the tendon.
- Dorsal S-Curve Incision: For proximal phalangeal fractures, an incision extending from the MCP joint to the proximal interphalangeal (PIP) joint in an S-curve provides extensile exposure.
Surgical Technique: Lag Screw Fixation
For oblique or spiral fractures where the fracture length is at least twice the diameter of the bone, lag screw fixation provides superior biomechanical stability, converting torsional loads into axial compression.
Surgical Warning: Limit periosteal stripping to 1 or 2 mm—only enough to ensure anatomical reduction. Excessive stripping devascularizes the fracture fragments and promotes dense adhesions between the bone and the overlying extensor mechanism.
Step-by-Step Technique:
* Preparation: Following local débridement of the fracture hematoma and interposed soft tissue, anatomically reduce the fracture.
* Provisional Fixation: Utilize pointed reduction forceps or 0.035-inch Kirschner wires (K-wires) for temporary fixation. Ensure K-wires are placed out of the planned trajectory of the screws.
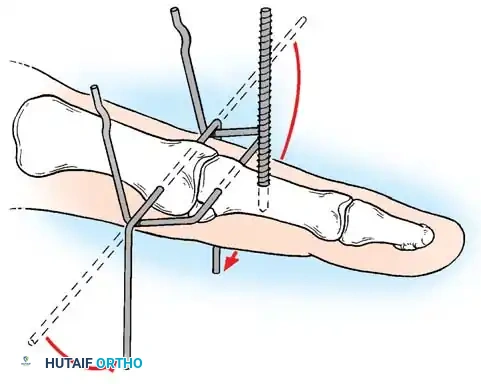
* Screw Trajectory Planning:
* For compressive forces (which act to deform and shorten the bone), place the screw at 90 degrees to the bone’s long axis.
* For torsional stress, place screws at 90 degrees to the fracture plane.
* The Optimal Compromise: To resist both axial and torsional loading, place a screw that bisects the angle between a line 90 degrees to the fracture and a line 90 degrees to the bone’s long axis.
* Drilling and Placement: Use the lag technique. Overdrill the near cortex (gliding hole) and drill the far cortex with the core diameter drill (thread hole). Check that screw placement near the fracture spikes is accurate to ensure bicortical purchase.
* Implant Selection: Use 2.0-mm screws for diaphyseal shaft fractures and 2.7-mm screws for metaphyseal fractures. Metacarpal head fractures usually can be fixed with a single screw; fractures of the metaphysis and diaphysis require a minimum of two screws.
* Countersinking: Always countersink the screw head. This allows for better load distribution under the screw head and removes prominence that could abrade the extensor tendon.

Minicondylar Plate Fixation
Büchler and Fischer popularized the use of minicondylar plates for complex metacarpal and phalangeal periarticular injuries.
Indications:
1. Acute fractures associated with partial or complete flexor tendon disruption treated with primary tenorrhaphy and early motion.
2. Replantation of digits.
3. Metaphyseal osteotomies of phalanges or metacarpals, especially in conjunction with capsulotomy or tenolysis.
4. Digit reconstruction (osteoplastic, pedicle graft, free composite tissue transfer) requiring stable skeletal fixation.
5. Arthrodesis of the PIP or MCP joints.
Contraindications:
1. Use in the vicinity of open physes in pediatric patients.
2. Joint fragments narrower than 6 mm (for the 2.0-mm plate) or 5 mm (for the 1.5-mm plate).
3. Condylar blade and screw intraarticular insertion (with the exception of the dorsal recess of the metacarpal head).
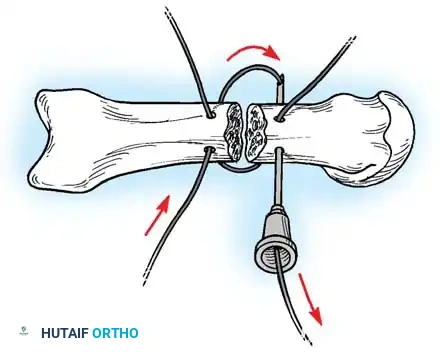
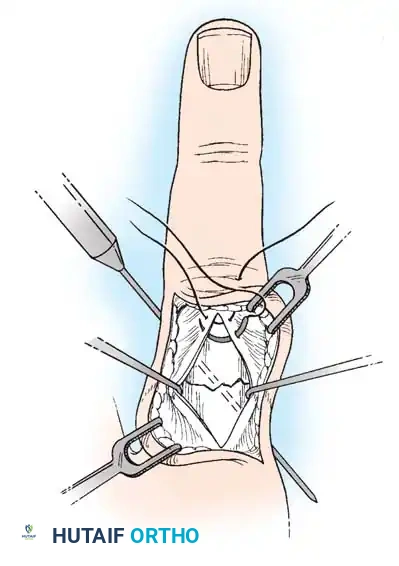
Open Reduction and K-Wire Fixation: The Pratt Technique
For transverse or short oblique fractures where screw fixation is impossible, the Pratt technique offers a reliable method of crossed K-wire fixation.
Step-by-Step Technique:
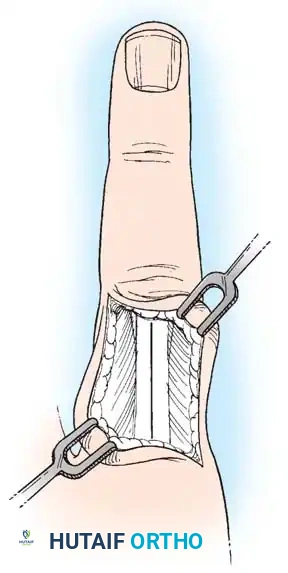
* Expose the extensor tendon and incise it longitudinally precisely in its center. Retract it to each side to expose the fracture site.
* Drill a K-wire into the distal fragment under direct vision.
* After anatomically reducing the fracture, drill the wire retrograde into the proximal fragment.
* Repeat with a second wire to create a crossed configuration, ensuring rotational stability.
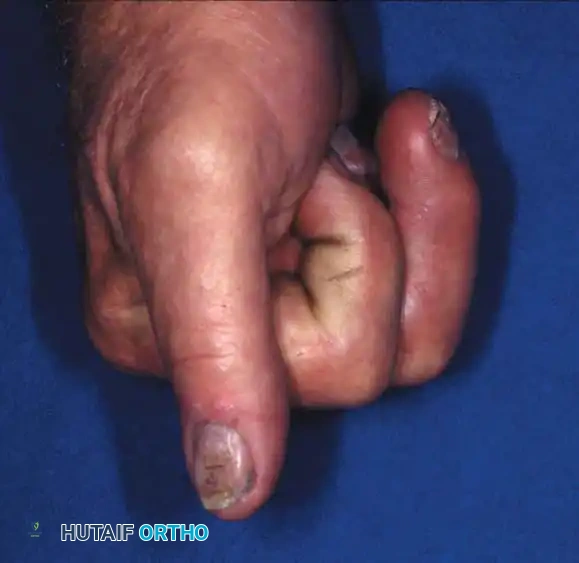
* Correct any rotational deformity (scissoring of the digits). Note that while some minor shortening may be acceptable, malrotation is poorly tolerated and leads to digital overlap during flexion.
* Meticulously repair the extensor tendon with a fine non-absorbable or slowly absorbing suture.
* Support the finger in the position of function (MCP flexed 70 degrees, PIP extended) and the wrist in 30 degrees of extension.

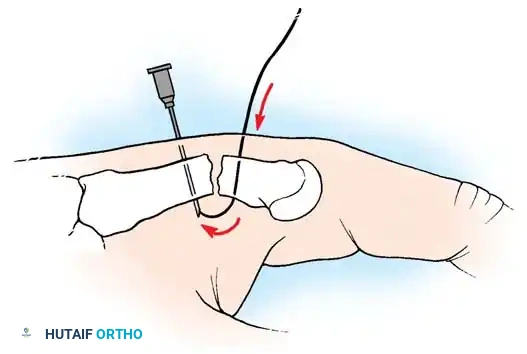
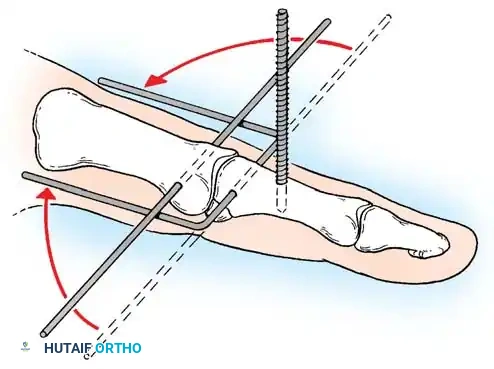
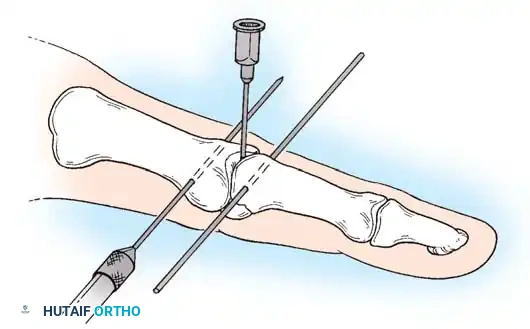
Percutaneous Techniques: Belsky-Eaton Pinning
Sometimes an unstable oblique fracture of a middle or proximal phalanx can be treated by closed reduction and percutaneous pinning. Belsky and Eaton described a highly effective technique for pinning multiple proximal phalangeal fractures without opening the fracture site.
Step-by-Step Technique:
* The fractured phalanx is held reduced with the MCP joint flexed to 90 degrees. This tightens the collateral ligaments, using them as a tension band to align the proximal fragment.
* A single K-wire is drilled from the dorsal aspect of the metacarpal head, passing across the MCP joint and straight down the medullary canal of the proximal phalanx to cross the fracture.
* Crucial Step: The wire must not cross the PIP joint.
* Leave the wire exposed proximally (bent outside the skin) to allow for easy removal in the clinic at 3 to 4 weeks.
Management of Severe Comminution
Open or severely comminuted fractures of the phalanges may be unsuitable for internal fixation using traditional plates or screws, as the hardware may further fragment the bone or require excessive soft-tissue stripping.
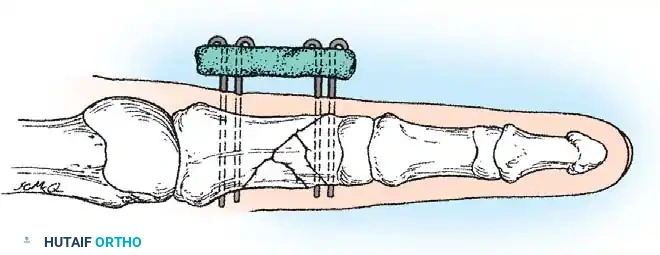
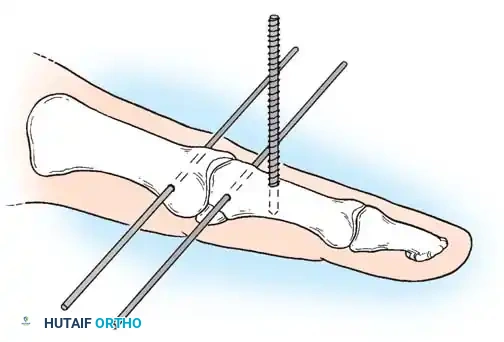
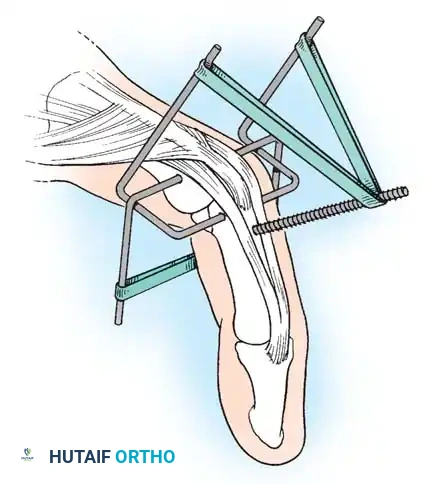
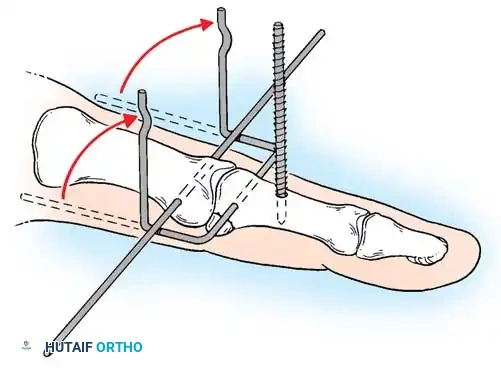
In such cases, external fixation using a mini external fixator is ideal. Alternatively, the technique suggested by Milford utilizes percutaneous transverse K-wires joined externally by a segment of polymethyl methacrylate (PMMA) bone cement. This acts as a custom, low-profile external fixator. Final alignment of the bone is manually maintained while the acrylic cement sets.
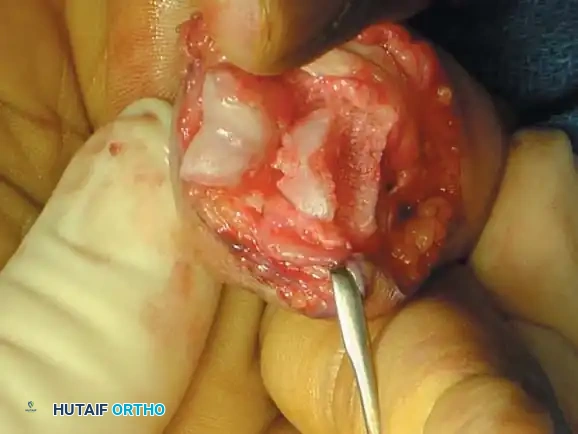
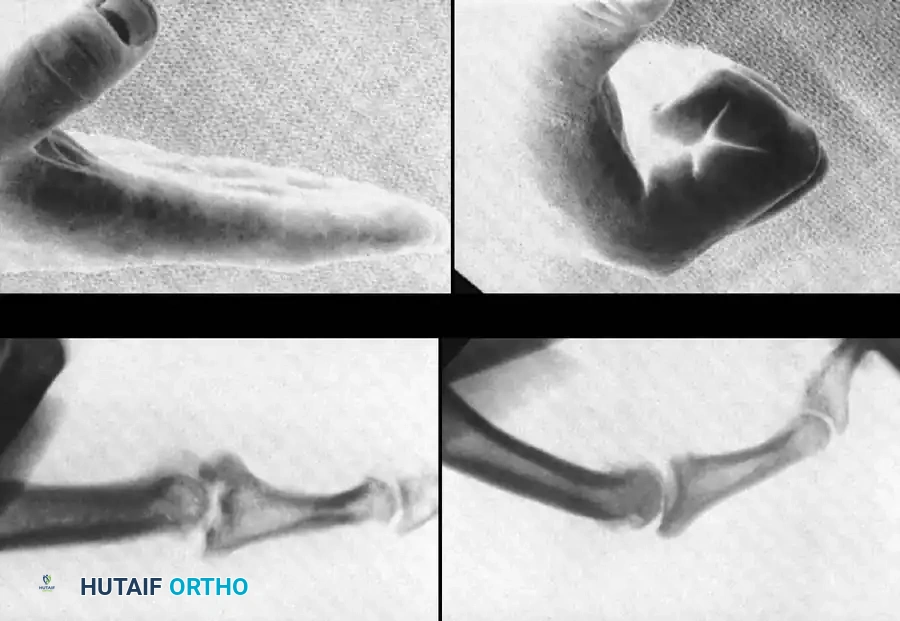
Fracture-Dislocations of the Proximal Interphalangeal (PIP) Joint
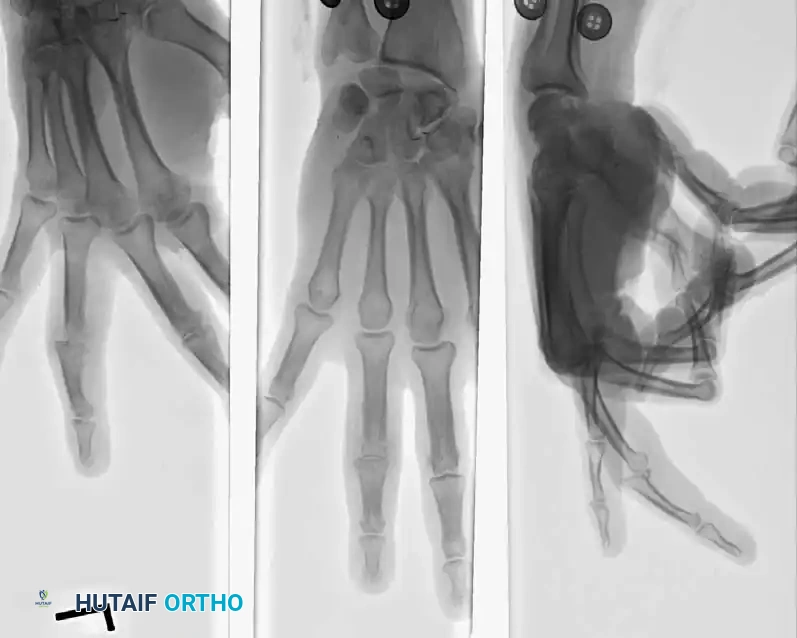
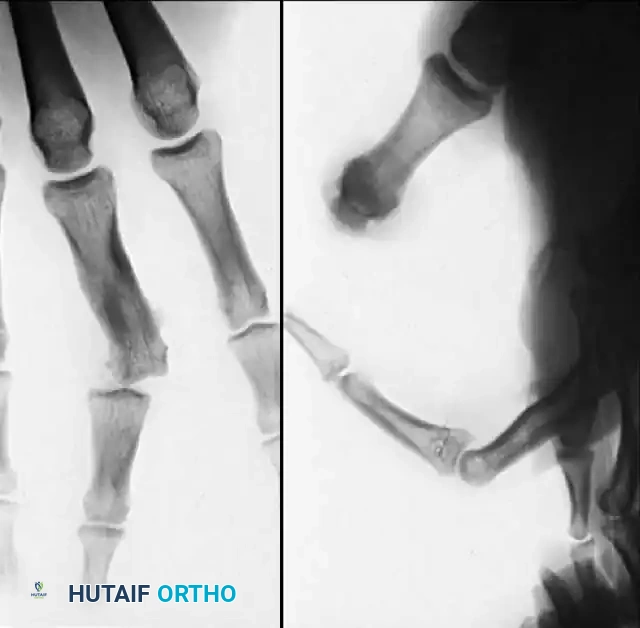
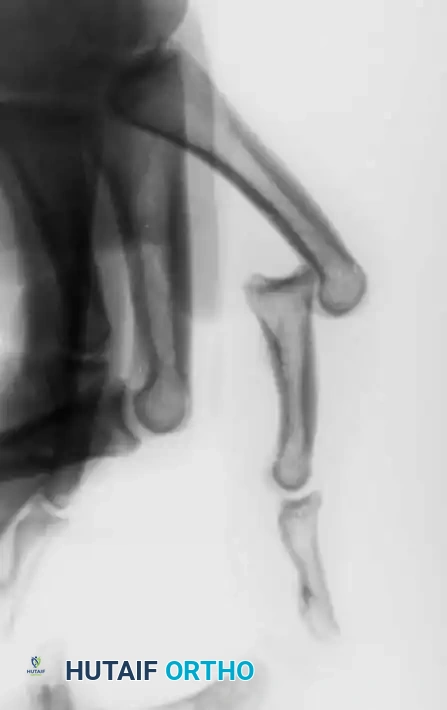
Fracture-dislocations at the PIP joint typically result in an unstable dorsal displacement of the middle phalanx. This is caused by the disruption of the volar plate's attachment to the volar lip of the middle phalanx, often accompanied by impaction of the articular surface.
Treatment is strictly dictated by the percentage of articular surface involved and the degree of comminution.
1. Large Volar Fragment (>50% of Joint Surface)
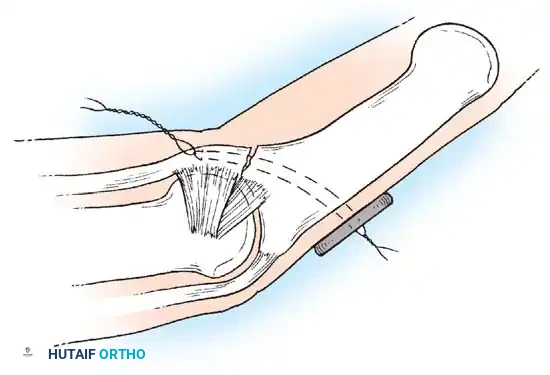
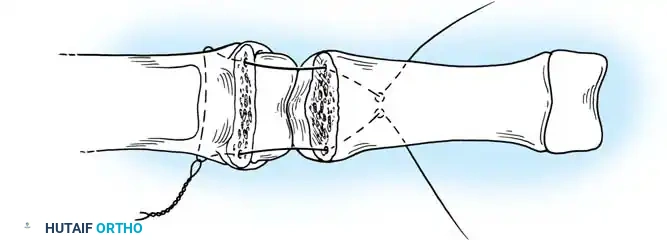
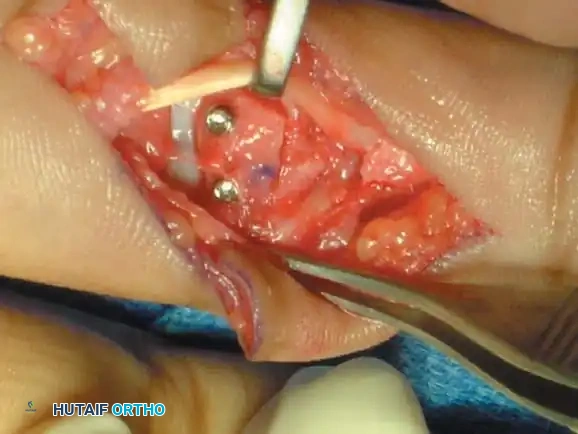
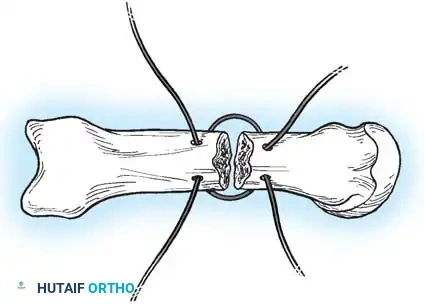
If a large, single volar fragment involving more than 50% of the joint surface is present, the joint is highly unstable. Open reduction and internal fixation (ORIF) is required. This can be achieved with miniature lag screws, K-wires, or a wire loop pull-out technique to secure the fragment and restore the volar buttress.
2. Small Volar Fragment (<50% of Joint Surface): Extension Block Splinting
If the fragment includes less than 50% of the articular surface and the joint can be concentrically reduced in flexion, the technique described by McElfresh, Dobyns, and O’Brien is the gold standard. This allows active motion of the PIP joint while maintaining the finger in an extension block splint.
Closed Reduction Technique (McElfresh, Dobyns, and O’Brien):
* Determine the exact angle of extension at which the PIP joint subluxates dorsally (the "instability angle") under fluoroscopy.
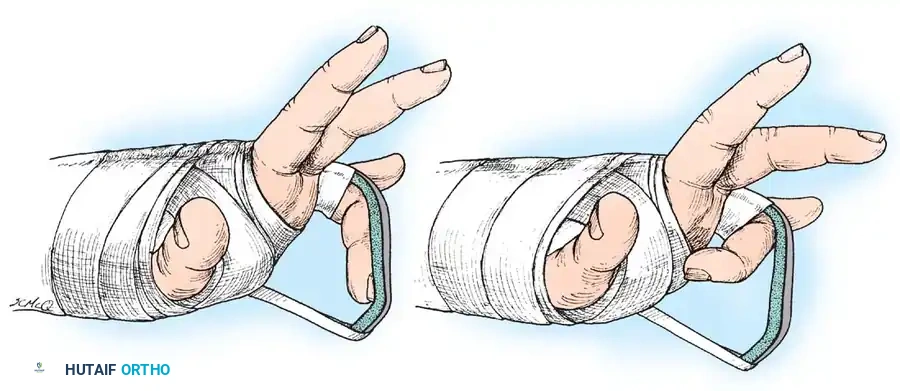
* Incorporate a malleable metal dorsal splint into a forearm gauntlet plaster cast.
* Position the splint so the involved finger is maintained in flexion at both the MCP and PIP joints.
* Block the PIP joint in flexion exactly 15 degrees short of the demonstrated position of instability.
* Ensure the proximal phalanx is held securely against the dorsal splint to prevent paradoxical extension at the PIP joint caused by further flexion of the MCP joint.
* Aftertreatment: Immediate active flexion of the PIP joint is permitted and encouraged. Full extension is blocked for 6 to 12 weeks; however, the splint is adjusted weekly to permit an increased amount of extension as the fracture heals.
3. Comminuted Volar Fragment (≤40%): Volar Plate Arthroplasty
In PIP fracture-dislocations with a comminuted surface of the middle phalanx of 40% or less, or in persistent dorsal fracture-dislocations with preserved condyles of the proximal phalanx, the method of Eaton and Malerich (Volar Plate Arthroplasty) is indicated. This technique resurfaces the joint and restores the volar tether.
Open Reduction Technique (Eaton and Malerich):
* Make a volar incision using an elongated V with the flap based radially (or a standard Brunner zigzag incision).
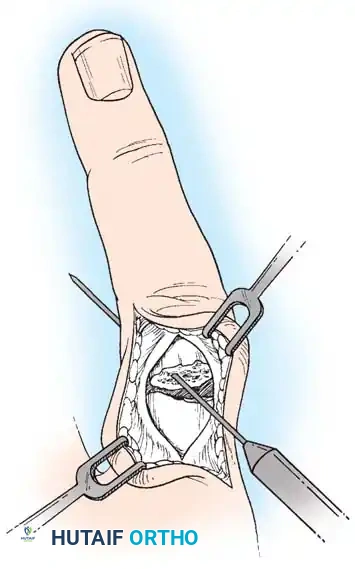
* Excise the flexor tendon sheath (C1 and A3 pulleys) from the proximal phalanx sufficiently to allow the flexor tendons to be retracted laterally, exposing the entire volar aspect of the joint.
* Hyperextend the joint to identify the fracture in fresh injuries.
* The volar plate is usually still attached to the comminuted bone fragments of the middle phalanx. Detach the volar plate from these fragments.
* Excise the comminuted volar lip fragments to create a smooth transverse trough at the base of the middle phalanx.
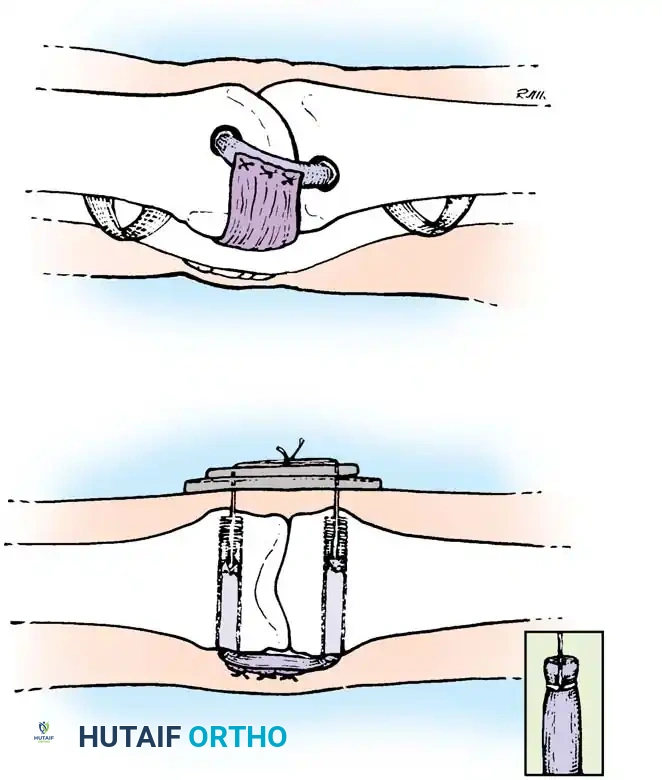
* Advance the volar plate into this bony defect and secure it using a pull-out wire or suture anchors, effectively resurfacing the volar aspect of the joint and restoring stability.
4. Chronic Instability: Autogenous Hemihamate Osteoarticular Grafting
When PIP joint dorsal subluxation persists even with 30 degrees of PIP joint flexion, or when >50% of the volar lip is destroyed and cannot be fixed, an autogenous hemihamate osteoarticular graft is recommended (Williams et al.).
A size-matched segment of the distal hamate articular surface (between the 4th and 5th metacarpal facets) is harvested. This graft perfectly matches the bicondylar contour of the middle phalanx base.
Surgical Pearl: Despite the dramatic stability achieved intraoperatively with a hemihamate graft, it is highly recommended to protect the repair with provisional transarticular K-wire pinning for 2 weeks to prevent graft displacement during early healing.
Postoperative Protocols and Rehabilitation
The ultimate success of phalangeal fracture management relies heavily on postoperative rehabilitation.
- Rigid Internal Fixation (Screws/Plates): If stable fixation is achieved, the finger is splinted for only 3 to 5 days to allow soft-tissue swelling to subside. Protected early active range of motion is then initiated under the guidance of a certified hand therapist.
- K-Wire Fixation: The finger is splinted in the intrinsic-plus position for 2 to 3 weeks. Wires are typically removed in the clinic at 3 to 4 weeks once clinical and radiographic callus is evident.
- Severe Comminution: Fractures treated with external fixation or traction require meticulous pin site care. Motion at the uninvolved joints (MCP, DIP) should be encouraged immediately to prevent complex regional pain syndrome (CRPS) and tendon adhesions.
Some fractures around the PIP joint result in poor outcomes despite the achievement of a concentric reduction. Persistent swelling, limited motion, and intrinsic imbalance commonly accompany comminuted fractures of the middle phalangeal base regardless of the method of open reduction. In these complex injuries, maintaining the undisturbed soft-tissue envelope around the fracture fragments via closed traction often yields faster healing and better final ROM than aggressive internal devices.
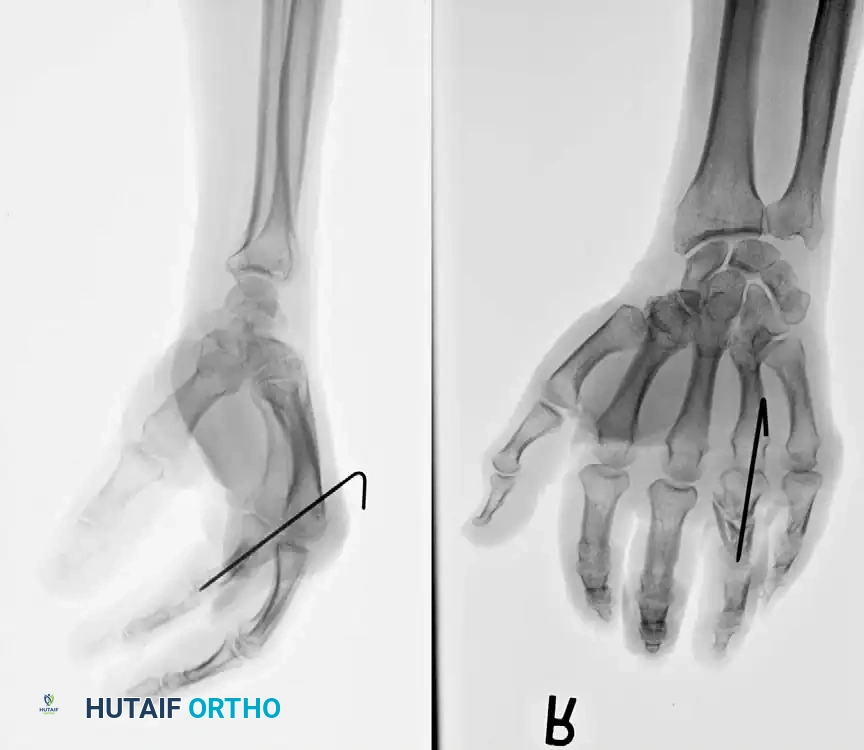
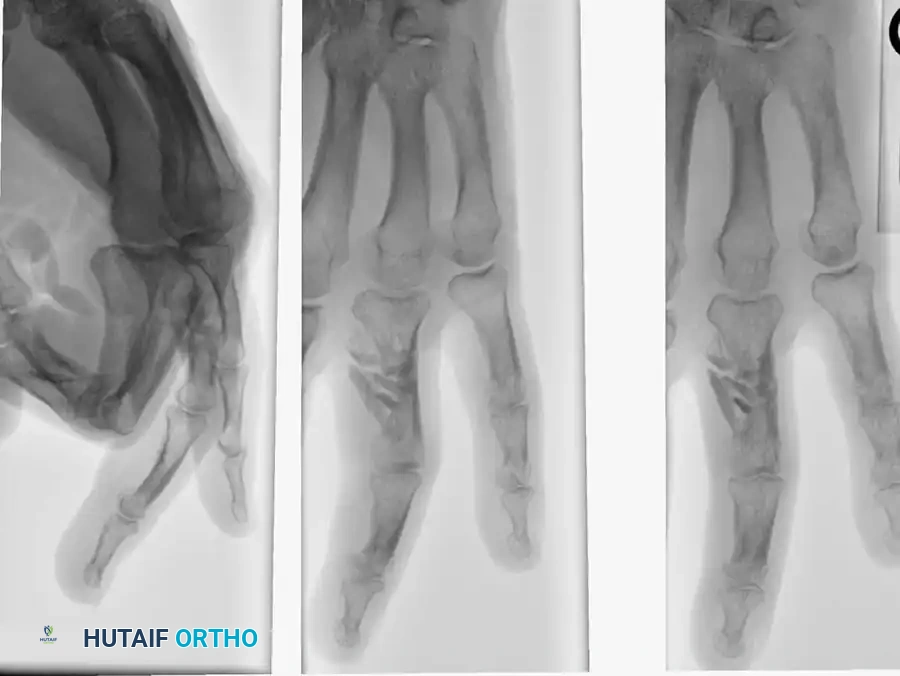
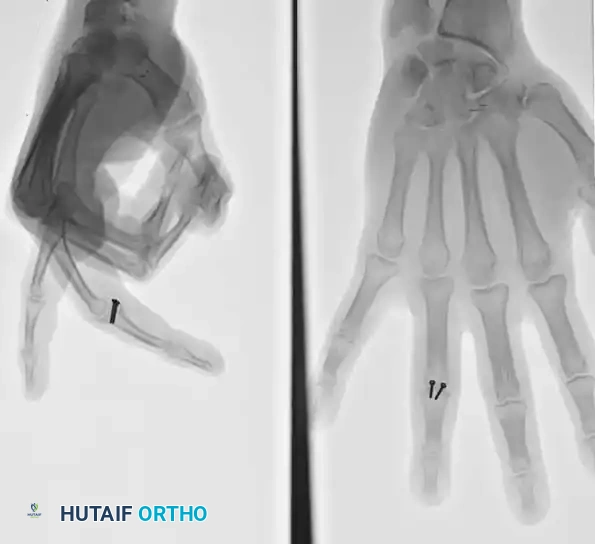
Associated Surgical & Radiographic Imaging



















You Might Also Like


