Open Reduction and Internal Fixation of Thumb Metacarpal Base Fractures
Key Takeaway
Open reduction and internal fixation (ORIF) of thumb metacarpal base fractures, including Rolando and Bennett patterns, requires meticulous articular restoration to preserve trapeziometacarpal joint function. This advanced surgical guide details the Foster and Hastings technique, utilizing a palmar radial approach, provisional Kirschner wire stabilization, and rigid 2.7-mm T-plate or L-plate fixation. Strict adherence to biomechanical principles and early postoperative mobilization are essential for optimal outcomes.
Introduction to Thumb Metacarpal Base Fractures
Fractures of the base of the thumb metacarpal represent a unique and challenging subset of hand trauma. The trapeziometacarpal (TMC) joint is a highly mobile, biconcave saddle joint that is fundamental to the biomechanics of pinch and grasp. Disruption of this articular surface, as seen in Bennett (two-part) and Rolando (three-part or comminuted) fractures, rapidly leads to post-traumatic osteoarthritis and profound functional impairment if not anatomically restored.
Open Reduction and Internal Fixation (ORIF) is the gold standard for displaced, unstable, or incongruous intra-articular fractures of the thumb metacarpal base. The primary surgical objective is the exact restoration of the articular congruity, followed by stable internal fixation that permits early active range of motion. This comprehensive guide details the operative management of these complex injuries, with a specific focus on the Foster and Hastings plating technique and alternative salvage methods for severe comminution.
Surgical Anatomy and Pathomechanics
Understanding the deforming forces acting upon the thumb metacarpal is critical for achieving and maintaining reduction. The fracture patterns are dictated by the intrinsic and extrinsic musculotendinous units crossing the first carpometacarpal (CMC) joint.
- The Volar Ulnar Beak Fragment: In both Bennett and Rolando fractures, the volar ulnar articular fragment remains anatomically reduced within the TMC joint. It is held securely in place by the robust anterior oblique ligament (AOL), which originates from the trapezium.
- The Metacarpal Shaft: The distal metacarpal shaft is subjected to powerful deforming forces. The abductor pollicis longus (APL) inserts at the dorsal-radial base of the metacarpal, pulling the shaft proximally, dorsally, and radially. Simultaneously, the adductor pollicis pulls the distal aspect of the metacarpal ulnarly into the palm, creating a supination and adduction deformity.
💡 Clinical Pearl: Deforming Forces
The hallmark of a thumb metacarpal base fracture is the proximal, dorsal, and radial subluxation of the metacarpal shaft driven by the APL. Successful ORIF requires counteracting these exact vectors during the reduction maneuver: longitudinal traction, palmar abduction, and pronation.
Preoperative Evaluation and Imaging
Accurate preoperative planning relies on high-quality orthogonal imaging. Standard posteroanterior (PA) and lateral views of the hand are insufficient due to the 30-degree pronated position of the thumb relative to the rest of the hand.
Radiographic Protocol
- True AP (Robert's View): The forearm is maximally pronated with the dorsum of the thumb resting flat against the cassette. This provides a true anteroposterior view of the TMC joint.
- True Lateral View: The hand is pronated 15 to 30 degrees, and the X-ray beam is directed parallel to the palmar surface of the fingers.
- Computed Tomography (CT): For complex Rolando fractures or severe comminution, a fine-cut CT scan with 3D reconstructions is invaluable for mapping articular fragments and planning screw trajectories.
Indications for Open Reduction and Internal Fixation
While some minimally displaced fractures may be managed with closed reduction and percutaneous pinning (CRPP), ORIF is strictly indicated in the following scenarios:
* Intra-articular step-off or gap greater than 1.0 to 2.0 mm.
* Failure to achieve or maintain closed reduction.
* Large articular fragments that can accommodate lag screw fixation.
* Open fractures requiring formal debridement.
* Polytrauma patients requiring immediate upper extremity weight-bearing for transfers.
Patient Positioning and Preparation
- Anesthesia: Regional anesthesia (supraclavicular or axillary brachial plexus block) is preferred, supplemented with intravenous sedation or general anesthesia based on patient factors.
- Positioning: The patient is placed supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Equipment: A mini-C-arm fluoroscopy unit must be positioned perpendicular to the hand table to allow for dynamic intraoperative imaging without compromising the sterile field.
Surgical Approach: The Palmar Radial Incision
The Foster and Hastings technique utilizes a palmar radial approach, which provides excellent visualization of the TMC joint and the volar articular fragments.
Step-by-Step Exposure
- Incision: Make a palmar radial incision, similar to the classic Wagner approach used for a Bennett fracture. Begin at the dorsal-radial aspect of the TMC joint and curve the incision volarly and distally along the glabrous border of the thenar eminence.
- Distal Extension: Extend the radial end of the incision distally along the diaphyseal portion of the thumb metacarpal to allow for adequate plate placement.
- Nerve Protection: Carefully dissect through the subcutaneous tissues. Identify and protect the sensory branches of the superficial radial nerve (SBRN) and the lateral antebrachial cutaneous nerve (LABCN).
🚨 Surgical Warning: Neuroma Prevention
Aggressive retraction or inadvertent transection of the superficial radial nerve branches will lead to the development of a highly debilitating, painful neuroma. Use blunt retraction and maintain meticulous hemostasis to keep the nerve branches in view throughout the procedure.
- Muscular Interval: Elevate the thenar musculature (abductor pollicis brevis and opponens pollicis) extraperiosteally from the palmar aspect of the metacarpal shaft.
- Arthrotomy: Perform a longitudinal arthrotomy of the TMC joint to expose the articular surface and the fracture hematoma. Irrigate the joint to remove debris and visualize the volar ulnar fragment.
Surgical Technique: The Foster and Hastings Plating Method
Once exposure is achieved, the focus shifts to anatomic articular reduction and rigid internal fixation using a 2.7-mm system.
1. Fracture Reduction and Provisional Fixation
- Clear the fracture site of organized hematoma and interposed periosteum.
- Reduce the two large basilar fragments (the palmar and dorsal articular fragments). This is often achieved using a combination of longitudinal traction, pronation, and direct manipulation with a dental pick or small pointed reduction forceps.
- Provisionally fix the reduced articular fragments with a 0.035-inch or 0.045-inch Kirschner wire (K-wire). Verify the articular congruity under direct vision and fluoroscopy.
2. Plate Selection and Positioning
- Select a small T-plate or L-plate designed to accept 2.7-mm screws. The plate must be contoured to match the normal slight volar concavity of the thumb metacarpal.
- Place the transverse portion of the T-plate over the basilar fragments of the metacarpal.
- The K-Wire Slide Technique: The previously placed provisional K-wire should ideally slide through one of the two proximal holes in the transverse portion of the plate. If the alignment is incorrect, place a second K-wire in line with one of the plate holes, secure the fragments, and remove the first wire.
3. Articular Reconstruction with Interfragmentary Compression
To achieve absolute stability at the articular surface, the screws placed through the transverse portion of the plate must function as lag screws.
- Drilling the Thread Hole: With a 2.0-mm drill bit, drill through the free hole in the transverse portion of the plate, passing through both the near (dorsal) and far (palmar) articular fragments.
- Tapping: Tap the drilled hole with a 2.7-mm tap to prepare the thread profile.
- Overdrilling for Lag Effect: To achieve interfragmentary compression, the near cortex (the dorsal fragment) must be overdrilled to create a gliding hole. Use a 2.7-mm drill bit to overdrill only the dorsal fragment.
- Screw Insertion: Insert a 2.7-mm cortical screw of appropriate length. As the screw head engages the plate, it will compress the palmar articular fragment against the dorsal articular fragment.
- Second Proximal Screw: Repeat the exact same lag screw technique with the second proximal plate hole to secure the articular block.
💡 Clinical Pearl: Complex Fracture Patterns
The exact fracture pattern may vary significantly. In some Rolando variants, you may require the use of a lag screw placed entirely separate from the plate, or two screws placed slightly off-center through the proximal plate holes to adequately compress the articular fragments together. Adapt your fixation strategy to the specific morphology of the fracture.
4. Metacarpal Shaft Fixation
- Once the articular block is anatomically reconstructed and compressed, reduce the metacarpal shaft to the stabilized intra-articular fragments.
- Ensure rotational alignment is correct by assessing the thumb nail cascade relative to the index finger.
- Attach the diaphyseal portion of the metacarpal to the long longitudinal portion of the T-plate or L-plate using standard 2.7-mm cortical screws.
Alternative Techniques: External Fixation and Tension Band Wiring
In cases of severe comminution (complex Rolando fractures) where the articular fragments are too small or numerous to accept 2.7-mm screws, rigid internal plating may be impossible. In these scenarios, the principles of ligamentotaxis must be employed.
The Distractor Technique
For highly unstable, comminuted fractures, an external fixation distractor combined with limited internal fixation (such as tension band wiring or fine K-wires) is a highly effective salvage technique.
- Pin Placement: Place two threaded half-pins into the trapezium (or radius, depending on the frame design) and two into the distal thumb metacarpal shaft.
- Distraction: Apply the external fixator and distract the joint. Ligamentotaxis will pull the comminuted fragments toward their anatomic positions via their capsular and ligamentous attachments.
- Limited Internal Fixation: If large enough fragments exist, use a tension band wiring construct or percutaneous K-wires to secure the major articular pieces while the ex-fix unloads the joint.
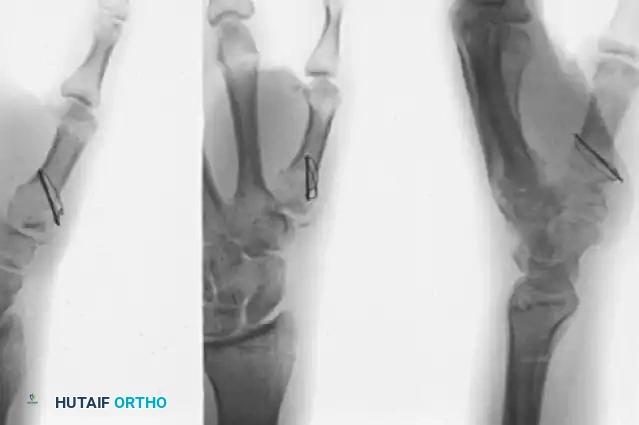
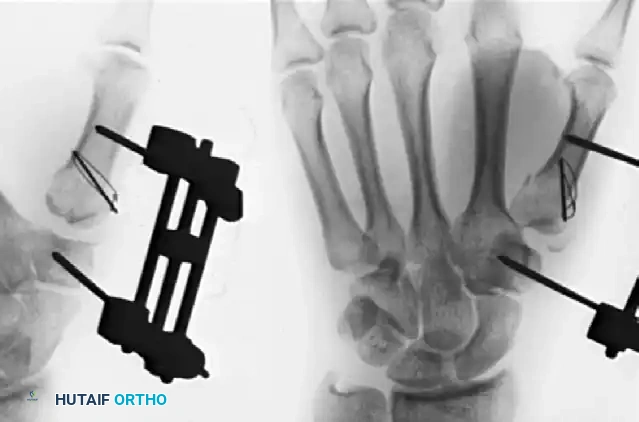
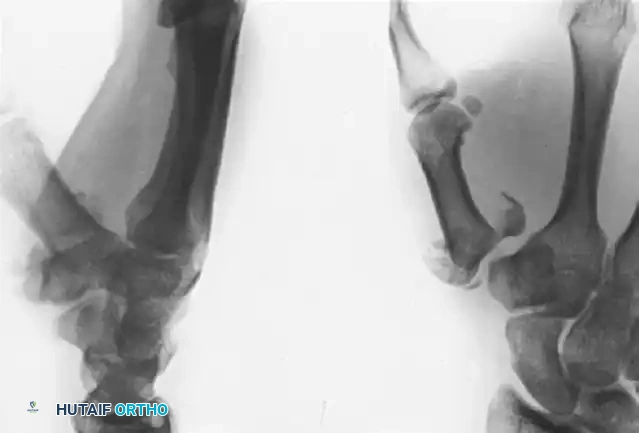
🔪 Surgical Technique 67-4: Severe Rolando Fracture Management
As demonstrated in Figure 67-15, a severely comminuted Rolando fracture can be successfully treated by an external fixation distractor combined with tension band wiring. Because the fracture is inherently unstable, the distractor is left in place for a full 8 weeks. This prolonged neutralization protects the articular cartilage during healing, frequently resulting in excellent carpometacarpal and metacarpophalangeal function.
Closure and Postoperative Protocol
Meticulous closure and a structured rehabilitation program are just as critical as the surgical execution.
Wound Closure
- Deflate the tourniquet and achieve meticulous hemostasis. Hematoma formation can lead to excessive scarring and stiffness.
- Repair the joint capsule if possible, though it is often incorporated into the fracture repair.
- Close the subcutaneous tissues with absorbable sutures and the skin with non-absorbable monofilament sutures.
- Apply a sterile, non-adherent dressing followed by a soft compressive dressing.
Immobilization and Rehabilitation
- Immediate Post-Op: The thumb is immobilized in a custom-molded thumb spica splint, leaving the interphalangeal (IP) joint free if it was not involved in the injury.
- Days 5 to 7: The bulky dressing is removed. Because rigid internal fixation (plating) provides absolute stability, active range-of-motion (AROM) exercises are begun within 5 to 7 days. Early mobilization is critical to prevent peritendinous adhesions and joint stiffness.
- Weeks 2 to 6: Sutures are removed at 10-14 days. The patient continues AROM out of the splint but wears a removable thermoplastic thumb spica orthosis between exercise sessions and at night.
- Weeks 6 to 8: Radiographic union is typically observed. The splint is discontinued, and progressive strengthening (pinch and grip exercises) is initiated.
- Weeks 10 to 12: Return to heavy manual labor and unrestricted activities is permitted once full radiographic consolidation and clinical strength are achieved.
Complications and Pitfalls
Despite meticulous technique, complications can arise following ORIF of thumb metacarpal base fractures.
- Post-Traumatic Osteoarthritis: The most common long-term complication. Even with anatomic reduction, the initial cartilage impact can lead to late-onset arthritis. Imperfect reduction (step-off >1mm) exponentially increases this risk, eventually requiring TMC arthrodesis or trapeziectomy.
- Sensory Neuroma: Injury to the superficial radial nerve branches during the palmar radial approach causes severe neuropathic pain. Prevention through careful dissection is paramount.
- Tendon Irritation or Rupture: Prominent hardware, particularly if placed too far dorsally or if screws protrude past the far cortex, can irritate or rupture the extensor pollicis longus (EPL) or flexor pollicis longus (FPL) tendons. Ensure screws are flush and plates are adequately covered by soft tissue.
- Loss of Reduction: Typically occurs if the patient is non-compliant with the postoperative splinting protocol or if the bone quality (osteoporosis) fails to hold the 2.7-mm screws. In osteoporotic bone, locking plates may be considered as an alternative to standard compression plates.
- Joint Stiffness: Prolonged immobilization is the enemy of the TMC joint. Strict adherence to the early active motion protocol (starting at 5-7 days) is essential for a functional outcome.
You Might Also Like

