Intraarticular Hand Fractures: Surgical Management & Malunion
Key Takeaway
Intraarticular fractures of the hand involving more than one-third of the articular surface with associated subluxation require precise anatomical reduction and stable fixation. This guide details the biomechanical principles, surgical approaches, and Kirschner wire fixation techniques for condylar fractures. It also provides evidence-based protocols for managing metacarpal malunions, emphasizing functional outcomes over radiographic appearance to optimize patient recovery and preserve grip strength.
PRINCIPLES OF INTRAARTICULAR FRACTURE MANAGEMENT
Intraarticular fractures of the phalanges and metacarpals present a complex biomechanical challenge. The preservation of articular congruity, joint stability, and a frictionless gliding surface is paramount to maintaining the intricate kinematics of the hand. Fractures that disrupt the articular surface inevitably alter the distribution of forces across the joint, predisposing the patient to post-traumatic osteoarthritis, stiffness, and profound functional impairment if managed inadequately.
When an intraarticular fracture yields a single fragment that involves one-third or more of the joint surface, the structural integrity of the joint is compromised. Such fractures are frequently accompanied by subluxation or frank dislocation due to the unopposed pull of intrinsic and extrinsic musculature, combined with the destabilization of the collateral ligament complex.
Surgical Warning: Non-operative management of displaced intraarticular fractures involving >30% of the articular surface with associated subluxation universally leads to poor functional outcomes. Anatomical reduction and stable fixation—typically utilizing Kirschner wires (K-wires) or interfragmentary sutures—are absolute indications.
Biomechanics and Pathoanatomy
The stability of the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints relies on a delicate balance between the bony architecture, the volar plate, and the collateral ligaments. In condylar fractures, the fracture line typically propagates sagittally or coronally through the articular surface.
Because the collateral ligament originates on the condyle, the displaced fragment is subjected to rotational and translational forces. However, this anatomical relationship can be leveraged surgically: the intact collateral ligament attached to the fractured condyle can be utilized as a tension band to assist in closed or percutaneous reduction via ligamentotaxis.
SURGICAL TECHNIQUE: CONDYLAR FRACTURES
Condylar fractures are notoriously unstable. While closed reduction can occasionally be achieved by flexing the finger and apposing the larger, stable fragment to the smaller, displaced fragment, maintaining this reduction without internal fixation is nearly impossible.
Preoperative Planning and Positioning
- Anesthesia: Regional block (axillary or supraclavicular) or a local wrist block is preferred to allow intraoperative assessment of the tenodesis effect if necessary.
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is inflated to 250 mm Hg following exsanguination.
- Fluoroscopy: A mini-C-arm must be positioned to allow seamless anteroposterior (AP), lateral, and oblique intraoperative imaging.
Step-by-Step Fixation Strategy
1. Assessment of Displacement
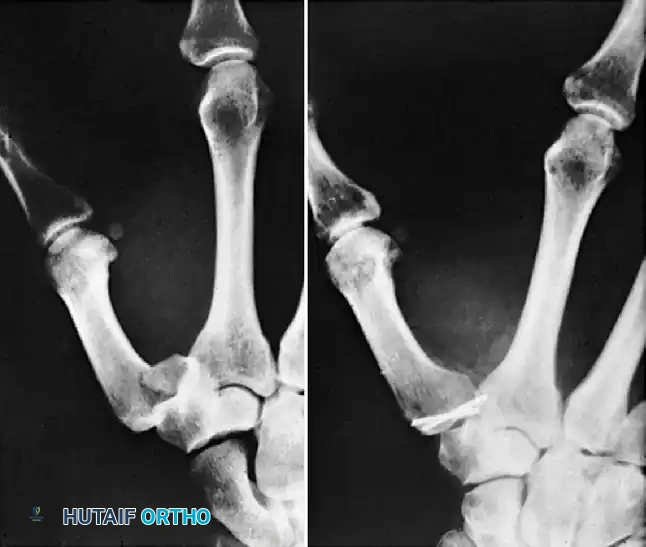
Initial fluoroscopic evaluation determines the degree of displacement and the size of the articular fragment. Displaced, unstable condylar fractures almost universally require open reduction and internal fixation (ORIF) or precise percutaneous pinning if closed reduction is successful.
Figure 1: Displaced, unstable condylar fracture. The articular step-off and rotational deformity necessitate intervention to restore joint congruity.
2. Closed Reduction via Ligamentotaxis
Before committing to a formal open approach, closed manipulation should be attempted. By applying traction and utilizing the intact collateral ligament, the surgeon can often guide the displaced condylar fragment back into its anatomical bed. The finger is typically flexed to tighten the collateral ligaments, which pulls the fragment into alignment with the intact condyle.

Figure 2: Manipulation of the fracture using the intact collateral ligament. This tension permits the precise insertion of a Kirschner wire to provisionally hold the reduction.
3. Kirschner Wire Fixation
Once anatomical reduction is confirmed fluoroscopically, percutaneous pinning is performed. A 0.035-inch or 0.045-inch K-wire is driven transversely across the condyles.
Clinical Pearl: A single K-wire acts as an axis of rotation. Even if the fracture appears perfectly reduced on AP and lateral views, a single wire cannot control the rotational forces exerted by the collateral ligament during postoperative mobilization.
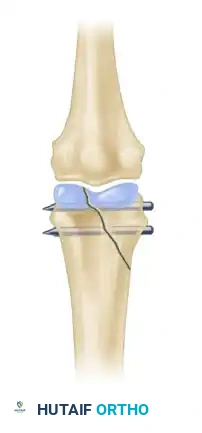
To prevent the reduced fragment from spinning around the primary wire, a second K-wire must be inserted. This second wire can be placed parallel to the first or in a divergent configuration, depending on the size of the fragment.

Figure 3: Two wires are strictly necessary to avoid rotation of the reduced fragment and ensure absolute stability of the articular surface.
4. Open Reduction (If Closed Manipulation Fails)
If closed reduction is inadequate (articular step-off >1 mm), an open approach is mandated.
* A mid-axial or dorsal approach is utilized.
* The extensor apparatus is carefully retracted or split longitudinally.
* The joint capsule is incised to visualize the articular surface directly.
* Hematoma and soft tissue interposition are cleared from the fracture site.
* The fragment is reduced under direct vision using a pointed reduction forceps, taking care not to crush the fragile articular cartilage.
* Fixation is achieved with two transverse K-wires or, if the fragment is large enough, miniature interfragmentary screws (1.0 mm or 1.2 mm).
Radiographic Confirmation
Intraoperative imaging must confirm absolute articular congruity. The K-wires are typically cut outside the skin and bent to facilitate removal in the clinic, though they may be buried if prolonged fixation is anticipated or patient compliance is a concern.

Figure 4: Anteroposterior radiograph demonstrating a condylar fracture anatomically reduced and fixed with two crossed Kirschner wires.

Figure 5: Lateral radiograph of the same condylar fracture, confirming restoration of the articular contour and appropriate wire placement.
MANAGEMENT OF MALUNITED FRACTURES
Despite optimal initial management, or in cases of neglected trauma, malunion of metacarpal and phalangeal fractures remains a significant clinical challenge. The functional consequences of malunion include weakness of grasp and pinch, particularly if the metacarpals and proximal phalanges are involved. Furthermore, patients frequently report a disturbance in their kinesthetic sense—a loss of fine proprioceptive control during complex hand tasks.
Rotational malalignment and angular deformities can cause notable aesthetic and functional hand deformity. This is most dramatically accentuated when the patient attempts to make a composite fist, leading to digital overlapping or "scissoring."
The Philosophy of Intervention
Surgical Warning: Not every malunited fracture requires surgical intervention. The function of the fingers and the hand—not the radiographic appearance—must dictate whether treatment is necessary. Ill-advised surgical treatment usually fails to improve function and, due to the risks of scarring and stiffness, frequently makes it worse.
Minor malunion deformities should generally be accepted, provided that the motion of the surrounding joints is satisfactory. This conservative approach is especially true in patients beyond middle age, where the risk of postoperative stiffness following an osteotomy far outweighs the biomechanical benefits of anatomical realignment.
Metacarpal Neck Malunions: Biomechanical Considerations
The tolerance for angular deformity in metacarpal neck fractures varies drastically depending on the specific ray involved. This is dictated by the compensatory mobility of the carpometacarpal (CMC) joints.
The Fifth and Fourth Metacarpals:
Most malunited fractures of the metacarpal neck should not be treated surgically, particularly those involving the fifth metacarpal. The fifth CMC joint possesses approximately 20 to 30 degrees of anteroposterior mobility.
* Flexion deformities of 40 degrees (and sometimes up to 50 degrees) in the fifth metacarpal neck can easily be accepted with excellent functional outcomes.
* When the fifth metacarpal head is displaced volarward due to a malunited neck fracture, the mobile CMC joint allows dorsal displacement of the distal end of the bone. Consequently, when a hard object is grasped, the palm yields, preventing the metacarpal head from acting as a painful pressure point.
* This compensatory mechanism is also true, albeit to a slightly lesser extent (10 to 15 degrees of mobility), for the ring finger (fourth metacarpal).
The Second and Third Metacarpals:
Conversely, the biomechanics of the index and long fingers are entirely different. There is little to no motion in the second and third CMC joints; they form the rigid central pillar of the hand.
* Because these joints cannot yield dorsally, any significant volar displacement of the metacarpal head results in a prominent bony mass in the palm.
* Patients with malunions of the second or third metacarpal neck frequently experience severe pain with firm grasp.
* Therefore, the threshold for surgical correction (osteotomy) in the second and third metacarpals is much lower, with angular deformities greater than 15 degrees often requiring intervention.
Secondary Deformities and Contractures
When a metacarpal head is markedly displaced volarward, the biomechanics of the MCP joint are fundamentally altered. To achieve digital extension, the proximal phalanx must hyperextend relative to the malpositioned metacarpal head. Over time, this MCP joint hyperextension leads to secondary contracture of the collateral ligaments in a shortened position.
If surgical correction of the malunion is undertaken late, simply performing a corrective osteotomy of the metacarpal will not restore motion. The contracted collateral ligaments will tether the joint. In these complex cases, a dorsal capsulotomy and collateral ligament release must be performed concomitantly with the corrective osteotomy.
Surgical Correction of Malunions
Certain malunions causing unacceptable functional deficits can be treated with corrective osteotomy.
Corrective Osteotomy Principles:
* Preoperative Planning: Precise measurement of the angular and rotational deformity is required. Contralateral radiographs are useful for templating.
* Approach: A dorsal longitudinal incision is made over the affected metacarpal or phalanx.
* Osteotomy: A closing wedge or opening wedge osteotomy is performed at the apex of the deformity (usually the old fracture site).
* Fixation: Rigid internal fixation is mandatory to allow early mobilization. This is typically achieved with a low-profile titanium mini-plate and screws, or crossed K-wires if plating is not feasible.
Osteoarticular Grafts:
In cases where intraarticular malunion has led to severe articular cartilage loss, angular deformity, subluxation, dislocation, or impending joint destruction accompanied by intractable pain, simple osteotomy is insufficient. In these salvage scenarios, osteoarticular grafts (such as transferring a portion of the toe proximal phalanx or hemi-hamate arthroplasty) may be useful to reconstruct the joint surface and restore a functional, pain-free arc of motion. Alternatively, in high-demand patients or those with end-stage destruction, arthrodesis or silicone arthroplasty may be indicated depending on the specific joint involved.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of both acute intraarticular fracture fixation and malunion correction relies heavily on meticulous postoperative rehabilitation.
- Immobilization: Immediately postoperatively, the hand is placed in a bulky soft dressing and a volar orthosis. The hand is positioned in the "intrinsic plus" position: wrist extended 20-30 degrees, MCP joints flexed 70-90 degrees, and PIP/DIP joints fully extended. This position maintains the collateral ligaments of the MCP joints at their maximal length, preventing contracture.
- Early Motion: If rigid internal fixation was achieved, active range of motion (AROM) of the uninvolved digits is encouraged immediately. Gentle, supervised AROM of the affected digit may begin within 3 to 5 days, depending on fracture stability.
- Pin Management: If percutaneous K-wires were used, pin site care is instituted. K-wires are typically removed in the clinic at 4 to 6 weeks once radiographic evidence of bridging callus is observed.
- Strengthening: Progressive strengthening and passive range of motion (PROM) exercises are delayed until clinical and radiographic union is confirmed, usually around 6 to 8 weeks postoperatively.
CONCLUSION
The management of intraarticular hand fractures demands a profound understanding of digital biomechanics and a meticulous surgical technique. While closed reduction and percutaneous pinning with multiple K-wires remain the gold standard for acute condylar fractures, the surgeon must be prepared to open the joint to ensure absolute articular congruity. In the realm of malunions, clinical judgment is paramount; the surgeon must weigh the functional deficits against the inherent risks of corrective osteotomy, always prioritizing the patient's functional capacity over the pursuit of radiographic perfection.
You Might Also Like