Mastering the Operative Management of the Four Medial Metacarpals

Key Takeaway
The management of medial metacarpal injuries requires a profound understanding of hand biomechanics and precise surgical execution. This comprehensive guide details the pathoanatomy, radiographic evaluation, and operative techniques for carpometacarpal fracture-dislocations, intraarticular fifth metacarpal base fractures, and complex metacarpophalangeal joint dislocations. Emphasizing evidence-based approaches, it provides orthopedic surgeons with step-by-step protocols for closed reduction, percutaneous pinning, and open reduction internal fixation to optimize functional outcomes.
INTRODUCTION TO THE MEDIAL METACARPALS
The four medial metacarpals (index, long, ring, and small) form the foundational longitudinal and transverse arches of the hand. Their precise anatomical alignment is paramount for grip strength, fine motor dexterity, and overall hand biomechanics. Injuries to these structures—ranging from carpometacarpal (CMC) fracture-dislocations to complex metacarpophalangeal (MCP) joint dislocations and diaphyseal fractures—demand meticulous clinical evaluation and often sophisticated surgical intervention. Failure to restore the intricate articular congruity and rotational alignment can lead to profound functional deficits, including weakened grip, chronic pain, and post-traumatic arthrosis.
CARPOMETACARPAL FRACTURE-DISLOCATION OF THE FINGER RAYS
Pathoanatomy and Clinical Presentation
Fracture-dislocations of the proximal articular ends of the medial metacarpals are high-energy injuries that are notoriously underdiagnosed in the acute setting. Massive dorsal and ulnar soft-tissue swelling frequently obscures the gross clinical deformity. While all four medial metacarpals can dislocate either dorsally or volarly, the fourth and fifth metacarpals are the most frequently involved, with dorsal displacement being the predominant vector due to the pull of the extrinsic extensor tendons.
🚨 CLINICAL PITFALL:
The massive edema associated with CMC fracture-dislocations can mask the step-off deformity. A high index of suspicion must be maintained in any patient presenting with a crush injury or axial load to the clenched fist.

Radiographic Evaluation
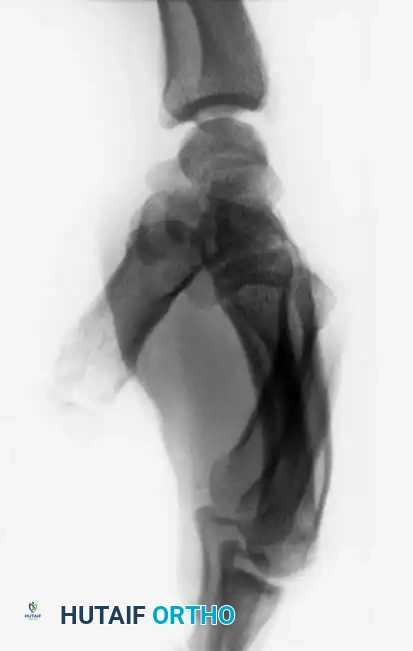
Standard posteroanterior (PA) radiographs may appear deceptively benign. The hallmark of a CMC dislocation on a PA view is the loss of the parallel joint surfaces (the "M" line) at the carpometacarpal articulations.

A true lateral radiograph is an absolute necessity for accurate diagnosis, as it will clearly demonstrate the dorsal or volar displacement of the metacarpal bases relative to the carpal row.

Oblique views further delineate the extent of articular comminution and subluxation.
Surgical Management
When identified acutely, manual reduction via longitudinal traction and direct pressure over the metacarpal bases is often easily achieved. However, the injury is inherently unstable.

Kirschner wire (K-wire) fixation is almost universally required to prevent redislocation.
For cases where closed reduction is unsuccessful or the injury is recognized late, Open Reduction and Internal Fixation (ORIF) is mandated. Lawlis and Gunther strongly advocate for open reduction and pinning, reporting excellent long-term results (average follow-up of 6.5 years). They recommend the open technique over closed percutaneous pinning to ensure anatomical reduction of the articular surface and to avoid inadvertent transfixation of the extensor tendons, which can lead to severe stiffness.
In chronic, neglected cases, open reduction may be impossible due to soft-tissue contracture and articular cartilage degradation. In such instances, resection of the proximal metacarpal base and formal carpometacarpal arthrodesis is the salvage procedure of choice.
INTRAARTICULAR FRACTURE OF THE BASE OF THE FIFTH METACARPAL
Biomechanics of the "Reverse Bennett" Fracture
Bora and Didizian highlighted the potentially disabling nature of intraarticular fractures at the base of the fifth metacarpal. This joint is highly mobile, permitting approximately 30 degrees of normal flexion and extension, alongside the crucial rotation necessary for power grasp and palmar cupping.
The pathoanatomy is directly analogous to a Bennett fracture of the thumb. The extensor carpi ulnaris (ECU) tendon inserts robustly onto the dorsal base of the fifth metacarpal. When an intraarticular fracture separates the base, the unopposed pull of the ECU displaces the metacarpal shaft proximally and dorsally, while the small articular fragment remains tethered to the hamate by the strong volar ligaments.
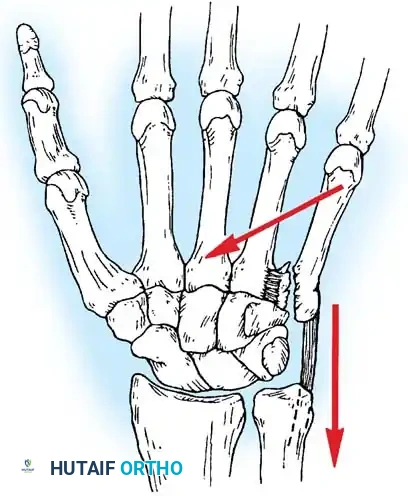
💡 SURGICAL PEARL:
Failure to anatomically reduce a fifth metacarpal base fracture results in a malunion that severely compromises the 30 degrees of essential CMC mobility, leading to profound weakness of grip and chronic, painful arthrosis.
Radiographic Diagnosis
Standard AP and lateral views are insufficient for a complete evaluation. A specialized radiograph taken with the hand in 30 degrees of pronation is required to profile the fifth CMC joint and accurately assess the articular surface and the degree of proximal migration.
Operative Treatment
Acute fractures can frequently be managed by closed reduction (longitudinal traction with volar pressure on the metacarpal base) followed by percutaneous K-wire fixation into the hamate and the adjacent fourth metacarpal. The construct is then protected in a cast for 4 to 6 weeks.
For fractures that present late or heal in a displaced position, surgical intervention is required to restore function. While corrective osteotomy of the malunion is an option, resection arthroplasty (excision of the metacarpal base with ECU tendon reattachment or interposition) is often preferred to reliably eliminate pain while preserving motion.

FINGER METACARPOPHALANGEAL DISLOCATIONS
Pathoanatomy of Complex Dislocations
Metacarpophalangeal (MCP) dislocations occur less frequently than interphalangeal dislocations but present a significantly greater challenge. They are most common in the index finger. Kaplan’s seminal description of the pathoanatomy remains the gold standard for understanding this complex injury.
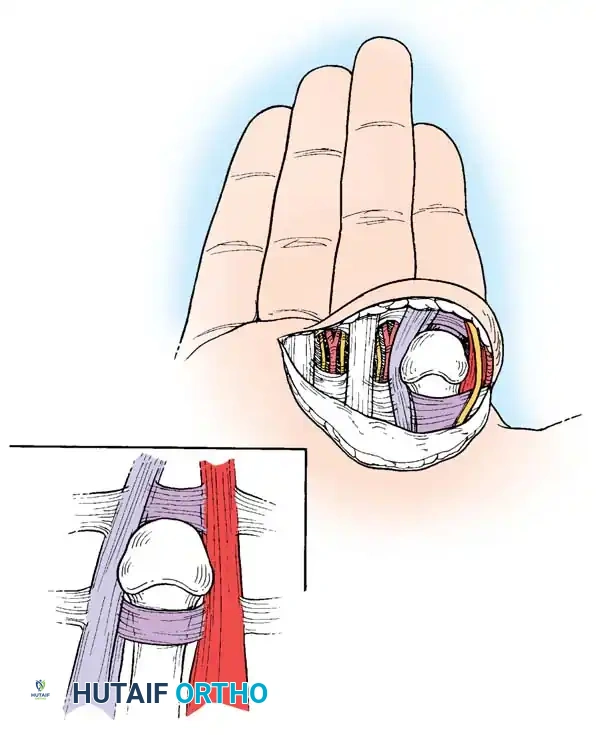
The primary lesion is the avulsion of the volar fibrocartilaginous plate from its weakest attachment—the volar aspect of the metacarpal neck.
1. The volar plate displaces dorsally over the metacarpal head, becoming wedged tightly between the base of the proximal phalanx and the metacarpal head.
2. The flexor tendons and the pretendinous band displace ulnarly.
3. The lumbrical muscle displaces radially.
4. The lateral collateral ligaments become abnormally displaced, locking the proximal phalanx in a dorsal, hyperextended position.
The metacarpal head is effectively strangulated in a "noose." Distally, the natatory ligament sits dorsal to the metacarpal head; proximally, the superficial transverse metacarpal ligament extends across the metacarpal neck volarly.
Closed Reduction Maneuver
Incomplete dislocations (subluxations) are easily reduced. However, complete dislocations require a specific maneuver. Approximately 50% can be reduced closed if performed correctly.
🚨 SURGICAL WARNING:
NEVER apply simple longitudinal traction to a complex MCP dislocation. Traction tightens the constricting bands (natatory and superficial transverse ligaments) around the metacarpal head, converting a reducible dislocation into an irreducible one.
The Correct Maneuver:
1. Hyperextend the MCP joint.
2. Apply firm, distally directed pressure against the dorsal base of the proximal phalanx, sliding it over the metacarpal head.
3. Once the articular surface clears the head, flex the joint. This maneuver attempts to push the interposed volar plate back to its normal anterior position.
Open Reduction: The Volar Approach (Kaplan)
If closed reduction fails, open reduction is mandatory. Kaplan's volar approach directly addresses the constricting structures.
🔪 Surgical Technique: Kaplan Volar Approach
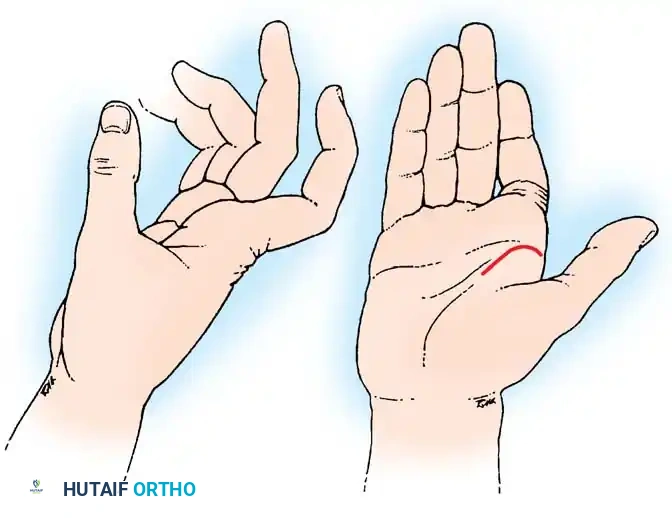
- Incision: Begin in the thenar crease at the radial base of the index finger and extend it proximally into the proximal palmar crease.
- Release Constrictions: Identify and divide the transverse fibers of the taut natatory ligament distally.
- Superficial Transverse Ligament: Make a longitudinal incision through the transverse fibers of the superficial transverse metacarpal ligament. Extend this release to the ulnar side of the first lumbrical muscle to decompress the metacarpal neck.
- Volar Plate Division: The critical step is addressing the volar plate. Incise the free edge of the torn ligament down to the junction of the periosteum with the proximal phalanx. Crucially, the incision must penetrate the entire thickness of the plate.
- Reduction: With the constrictions released, the base of the proximal phalanx will easily return to its anatomical position over the metacarpal head. The flexor tendons, volar plate, and neurovascular bundles are then restored to their normal volar alignment.
- Closure: Close the skin routinely and immobilize the finger in a functional position (MCP flexed 70 degrees) for approximately 1 week before initiating early active motion.
Open Reduction: The Dorsal Approach (Becton et al.)
Many contemporary hand surgeons prefer the dorsal approach advocated by Becton et al., citing several distinct advantages:
1. It provides direct, unparalleled exposure of the fibrocartilaginous volar plate, which is the primary mechanical block to reduction.
2. The digital neurovascular bundles are safely out of the surgical field, minimizing iatrogenic injury risk.
3. Occult osteochondral fractures of the metacarpal head can be easily visualized, reduced, and internally fixed.
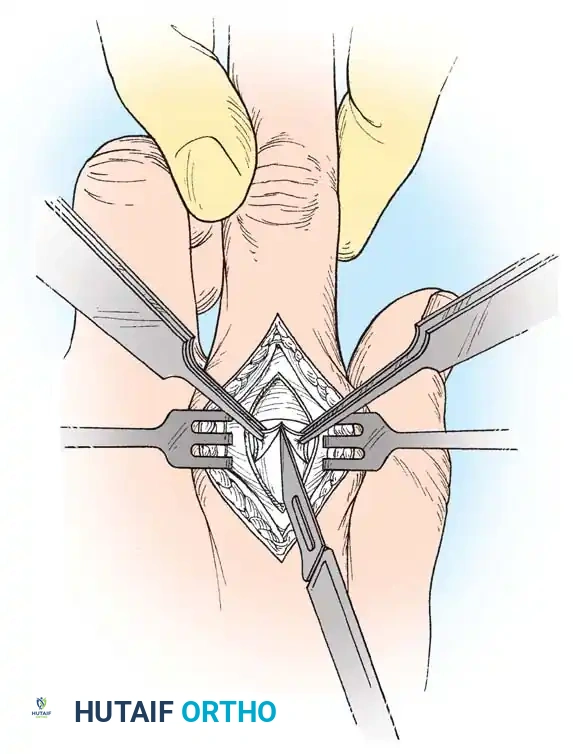
🔪 Surgical Technique: Becton Dorsal Approach
- Incision: Make a 4-cm dorsal midline longitudinal incision centered over the dislocated MCP joint.
- Deep Dissection: Split the underlying extensor tendon longitudinally. Incise the dorsal joint capsule in the same plane.
- Identify the Volar Plate: The displaced volar plate will be visible draped over the dorsal aspect of the metacarpal head. Note: It can be difficult to distinguish from articular cartilage due to its similar color and smooth texture.
- Incision of the Plate: Make a small exploratory incision to confirm the tissue is indeed the volar plate. Once confirmed, complete a longitudinal split through the substance of the plate.
- Reduction: Flex the patient's wrist volarly to release tension on the flexor tendons. Apply gentle traction to the finger and flex the MCP joint. The split volar plate will slide around the metacarpal head, allowing seamless reduction.
- Joint Inspection: Thoroughly irrigate the joint and inspect for any loose osteochondral fragments that may have been sheared off during the dislocation.
- Closure: Repair the extensor tendon and close the skin.
- Postoperative Protocol: Splint the MCP joint in slight flexion to prevent hyperextension for 3 weeks, but initiate early protected active flexion exercises to prevent stiffness.
FRACTURES OF THE METACARPAL SHAFT AND NECK
Indications for Operative Intervention
While the majority of isolated metacarpal shaft and neck fractures can be managed non-operatively with functional bracing or casting, surgical stabilization is strictly indicated in the following scenarios:
* Open fractures requiring debridement.
* Multiple metacarpal fractures (loss of the intrinsic splinting effect).
* Unacceptable angular deformity (especially in the index and long fingers, which tolerate less angulation than the mobile ring and small fingers).
* Rotational malalignment (clinical "scissoring" or overlapping of the digits during active flexion).
* Significant shortening (>3-5 mm) disrupting the intrinsic muscle balance.
Surgical Techniques and Fixation Strategies
1. Intramedullary Kirschner Wire Fixation
For transverse or short oblique fractures, intramedullary K-wire fixation provides excellent axial alignment with minimal soft-tissue stripping.
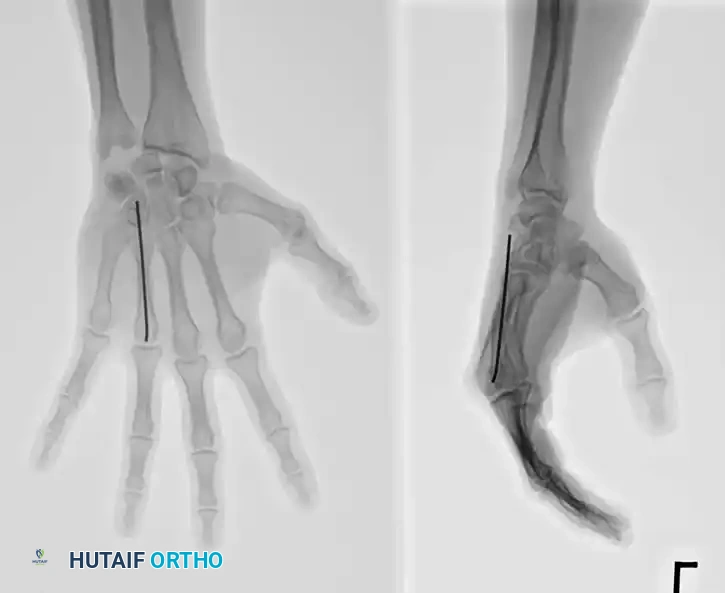
Technique: Introduce a 0.062-inch K-wire at the fracture site. Drill it retrograde out through the skin at the metacarpal base. While drilling, force a slight bow in the wire (convex toward the palm) and hold the wrist in flexion so the wire emerges safely on the dorsum of the wrist. Reduce the fracture anatomically. Drill the wire anterograde into the distal fragment, stopping just proximal to the articular surface of the MCP joint. Cut the proximal end beneath the skin.

Alternatively, closed percutaneous pinning can be performed. With the MCP joint acutely flexed (to tighten the collateral ligaments and control the distal fragment), introduce a K-wire through the metacarpal head and advance it across the fracture site under fluoroscopic guidance.


2. Interfragmentary Screw Fixation
Long oblique or spiral fractures of the metacarpal shaft (where the fracture length is at least twice the diameter of the diaphysis) are ideally suited for interfragmentary lag screw fixation.
This technique provides absolute stability, allowing for immediate postoperative mobilization. It requires minimal periosteal stripping and avoids the hardware prominence associated with dorsal plating. Typically, two or three 1.5 mm or 2.0 mm cortical screws are utilized, placed perpendicular to the fracture plane to maximize compression.


3. Plate and Screw Fixation
Short oblique, transverse, or highly comminuted fractures with unacceptable displacement require rigid stabilization with plate and screw constructs. Dorsal plating provides a strong biomechanical construct against the volar bending forces exerted by the intrinsic muscles.

Care must be taken to limit periosteal stripping to preserve the fracture hematoma and blood supply. Low-profile titanium plates (1.5 mm to 2.0 mm systems) are preferred to minimize irritation of the overlying extensor tendons.

In cases of severe comminution or bone loss, bridge plating techniques can be employed to maintain length and rotation while secondary bone healing occurs.

Postoperative Rehabilitation
Regardless of the fixation method chosen, the primary goal of metacarpal fracture surgery is to achieve sufficient stability to allow for early active range of motion (ROM).
* Days 1-5: Edema control, elevation, and immediate active ROM of the unaffected digits.
* Week 1-4: If rigid internal fixation (screws/plates) is achieved, active ROM of the affected digit is initiated under the guidance of a hand therapist. A custom thermoplastic splint is used between exercise sessions.
* Week 4-6: K-wires (if used) are typically removed at 4 weeks once clinical callus is evident. Progressive strengthening begins at 6 weeks.
* Radiographic Healing: Note that with rigid anatomical reduction (especially with lag screws), primary bone healing occurs without visible callus formation. Clinical union (absence of pain at the fracture site) dictates the advancement of therapy rather than radiographic consolidation.
By adhering to strict biomechanical principles, respecting the delicate soft-tissue envelope, and executing precise surgical techniques, the orthopedic surgeon can reliably restore the complex anatomy and function of the medial metacarpals.
📚 Medical References
- metacarpal fractures secondary to gunshot wounds, J Hand Surg 31A:1083, 2006.
- Bain GI, Mehta JA, Heptinstall RJ, et al: Dynamic external fi xation for injuries of the proximal interphalangeal joint, J Bone Joint Surg 80B:1014, 1998.
- Becton JL, Christian JD, Goodwin HN, et al: A simplifi ed technique for treating the complex dislocation of the index metacarpophalangeal joint, J Bone Joint Surg 57A:698, 1975.
- Belsole RJ, Greene TL: The confi guration of tension-band wires in hand fractures: the “sidewinder technique,” Tech Orthop 1:5, 1986.
- Bohart PG, Gelberman RH, Vandell RF, et al: Complex dislocations of the metacarpophalangeal joint, Clin Orthop Relat Res 164:208, 1982.
- Bora FW Jr, Didizian NH: The treatment of injuries to the carpometacarpal joint of the little fi nger, J Bone Joint Surg 56A:1459, 1974.
- Bowers WH: The proximal interphalangeal joint volar plate, II: a clinical study of hyperextension injury, J Hand Surg 6A:77, 1981.
- Büchler U, Fischer T: Use of a minicondylar plate for metacarpal and phalangeal periarticular injuries, Clin Orthop Relat Res 214:53, 1987.
- Büchler U, Gupta A, Ruf S: Corrective osteotomy for post-traumatic malunion of the phalanges in the hand, J Hand Surg 21B:33, 1996.
- Clendenin MB, Smith RJ: Fifth metacarpal/hamate arthrodesis for posttraumatic osteoarthritis, J Hand Surg 9A:374, 1984.
- Creighton JJ Jr, Steichen JB: Complications in phalangeal and metacarpal fracture management: results of extensor tenolysis, Hand Clin 10:111, 1994.
- Curtis RM: Capsulectomy of the interphalangeal joints of the fi ngers, J Bone Joint Surg 36A:1219, 1954.
- Diao E: Metacarpal fi xation, Hand Clin 13:557, 1997.
- Eaton RG, Malerich MM:
You Might Also Like

