Operative Management of Spinal Infections: A Comprehensive Surgical Guide
Key Takeaway
Spinal infections, encompassing pyogenic vertebral osteomyelitis, discitis, and epidural abscesses, present complex challenges requiring prompt diagnosis and decisive surgical intervention. This comprehensive guide details the pathogenesis, biomechanical considerations, and step-by-step operative techniques for managing spinal infections. Emphasizing evidence-based approaches, it covers anterior debridement, structural grafting, and posterior instrumentation, providing orthopedic surgeons and neurosurgeons with the critical protocols necessary to eradicate infection, decompress neural elements, and restore spinal stability.
Introduction to Spinal Infections
Spinal infections represent a heterogeneous group of debilitating conditions, encompassing pyogenic vertebral osteomyelitis (PVO), discitis, spinal epidural abscess (SEA), and postoperative surgical site infections. Historically associated with high morbidity and mortality, the management of spinal infections has evolved significantly. Modern operative orthopaedics dictates a multidisciplinary approach, combining targeted antimicrobial therapy with aggressive surgical debridement, neural decompression, and biomechanical stabilization.
This chapter synthesizes seminal literature and advanced surgical principles to provide a comprehensive, textbook-level guide for orthopedic residents, fellows, and practicing spine consultants. The focus remains strictly on evidence-based operative management, biomechanical considerations, and meticulous surgical techniques required to eradicate infection while preserving or restoring spinal integrity.
Pathophysiology and Biomechanics
Vascular Anatomy and Pathogenesis
The pathogenesis of spinal infections is intimately tied to the vascular anatomy of the vertebral column. As described in classic anatomical studies, the intervertebral disc in adults is largely avascular, relying on diffusion through the cartilaginous endplates for nutrition.
Infections typically seed the spine via three primary routes:
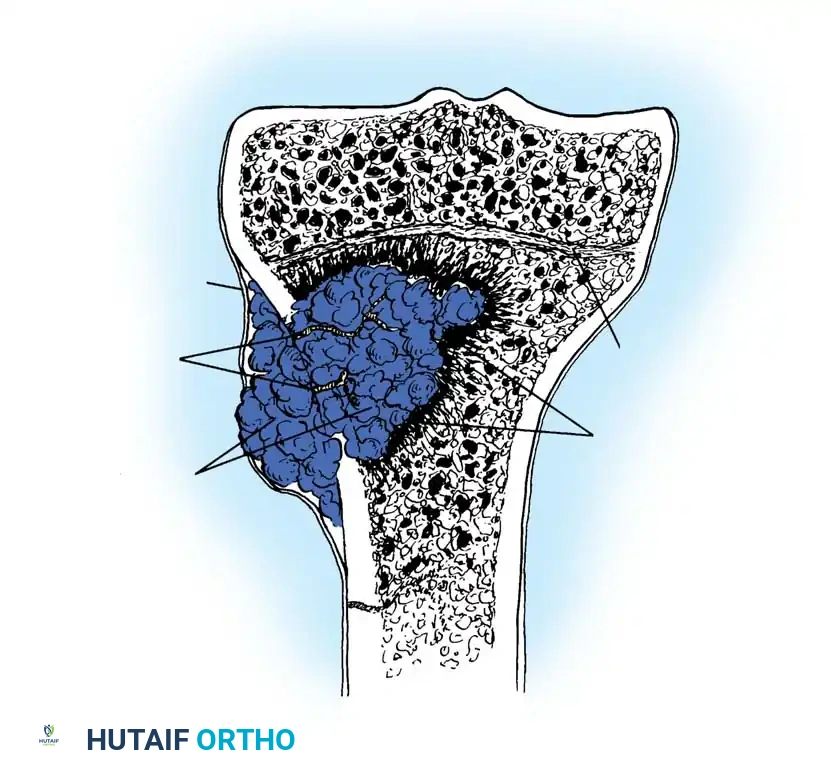
1. Hematogenous Dissemination: The most common route. Arterial spread typically lodges bacteria in the highly vascularized subchondral bone adjacent to the endplate. Venous spread, facilitated by retrograde flow through Batson’s valveless venous plexus, is particularly relevant in genitourinary infections.
2. Direct Inoculation: Occurs secondary to penetrating trauma, spinal injections, or open surgical procedures.
3. Contiguous Spread: Extension from adjacent soft tissue infections, such as retropharyngeal abscesses or psoas abscesses.
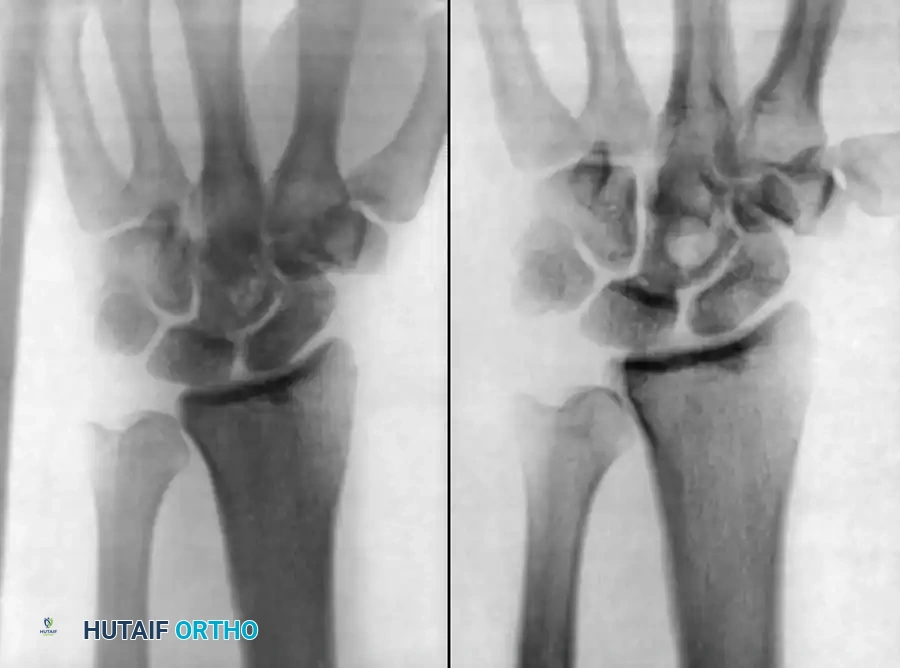
Once established in the vertebral metaphysis, the infection rapidly destroys the endplate and invades the avascular intervertebral disc, leading to discitis.
Biomechanical Consequences of Infection
The destruction of the anterior column (vertebral body and disc) leads to profound biomechanical instability.
* Loss of Load-Bearing Capacity: The anterior column supports approximately 80% of axial loads. Destruction leads to anterior collapse.
* Kyphotic Deformity: As the anterior column collapses, the spine hinges on the intact posterior elements, resulting in progressive focal kyphosis.
* Neural Compression: Retropulsion of infected bone, disc material, or the formation of an epidural abscess can directly compress the spinal cord or cauda equina.
Clinical Pearl: The biomechanical principle of treating spinal osteomyelitis is identical to treating a spinal tumor: radical resection of the diseased anterior column followed by robust structural reconstruction and stabilization.
Clinical Evaluation and Diagnostic Modalities
Presentation and Laboratory Markers
The classic triad of spinal infection—back pain, fever, and neurological deficit—is present in a minority of patients. Insidious, unrelenting back pain that worsens at night is the most consistent symptom.
Laboratory evaluation must include:
* Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP): CRP is highly sensitive and responds rapidly to treatment, making it the ideal marker for monitoring therapeutic efficacy.
* Blood Cultures: Positive in up to 50-60% of hematogenous pyogenic infections.
Advanced Imaging
- Magnetic Resonance Imaging (MRI): The gold standard. T1-weighted images show decreased signal in the vertebral body and disc, while T2-weighted and STIR sequences demonstrate hyperintensity (edema). Gadolinium enhancement is critical for delineating epidural abscesses.
- Computed Tomography (CT): Essential for preoperative planning to assess the extent of bony destruction, endplate integrity, and the presence of sequestra.
Image-Guided Biopsy
When blood cultures are negative, a CT-guided percutaneous needle biopsy is mandatory before initiating empiric antibiotics.
Surgical Pitfall: Initiating broad-spectrum antibiotics prior to obtaining a definitive tissue or blood culture can result in a "culture-negative" infection, severely complicating long-term targeted antimicrobial therapy. Withhold antibiotics in neurologically stable patients until a biopsy is obtained.
Indications for Surgical Intervention
While many spinal infections can be managed with prolonged intravenous antibiotics and rigid orthoses, surgical intervention is definitively indicated under the following circumstances:
- Neurological Deficit: Progressive motor weakness, myelopathy, or cauda equina syndrome secondary to epidural abscess or bony retropulsion.
- Spinal Instability or Deformity: Significant anterior column destruction leading to progressive kyphosis or mechanical instability.
- Failure of Medical Management: Persistent bacteremia, intractable pain, or rising inflammatory markers despite 3 to 4 weeks of culture-directed intravenous antibiotics.
- Epidural Abscess: Particularly in the cervical or thoracic spine where the epidural space is narrow and the spinal cord is highly vulnerable.
- Intractable Pain: Severe mechanical back pain that prevents mobilization.
Operative Principles and Surgical Approaches
The surgical management of spinal infections is dictated by the location of the pathology. Because pyogenic vertebral osteomyelitis predominantly affects the anterior column, the anterior approach is the workhorse for debridement and reconstruction.
1. Anterior Debridement and Structural Grafting (The Gold Standard)
Indications: Extensive anterior column destruction, anterior epidural abscess, kyphotic deformity.
Positioning and Exposure (Lumbar Spine):
* The patient is placed in the lateral decubitus position.
* A retroperitoneal approach is utilized to access the lumbar spine. This avoids contamination of the peritoneal cavity.
* The psoas muscle is carefully mobilized. In the presence of a psoas abscess, purulent material is evacuated immediately.
* Segmental vessels over the affected vertebral bodies are identified, ligated, and divided to mobilize the great vessels (aorta/vena cava).
Step-by-Step Debridement (Corpectomy):
1. Annulotomy and Discectomy: Radical excision of the infected intervertebral disc is performed.
2. Corpectomy: Using osteotomes, rongeurs, and a high-speed burr, the infected, necrotic bone of the vertebral body is resected until healthy, bleeding cancellous bone is encountered.
3. Epidural Decompression: The posterior longitudinal ligament (PLL) is identified and resected if an epidural abscess is present, allowing direct visualization and decompression of the thecal sac.
4. Endplate Preparation: The adjacent healthy endplates are meticulously prepared to bleeding bone to ensure optimal graft incorporation.
Reconstruction:
* Autograft: Tricortical iliac crest bone graft (ICBG) remains the gold standard for its osteoinductive and osteoconductive properties.
* Allograft/Titanium Cages: Modern literature supports the use of titanium mesh cages packed with autograft or allograft. Titanium is highly biocompatible and resists bacterial biofilm formation better than stainless steel.
Surgical Warning: Avoid using non-structural cancellous bone alone in the anterior column, as it will rapidly resorb in the infected bed, leading to graft subsidence and catastrophic kyphotic collapse.
2. Posterior Instrumentation and Stabilization
Indications: Supplementation of anterior column reconstruction, multi-level instability, or cases where the anterior approach is contraindicated due to severe medical comorbidities.
Biomechanics of Posterior Fixation:
Posterior pedicle screw instrumentation acts as a tension band, neutralizing flexion forces and preventing anterior graft subsidence. Historically, surgeons feared placing hardware in an infected field. However, contemporary evidence demonstrates that rigid stabilization actually promotes infection eradication by eliminating micromotion, which is detrimental to revascularization and immune cell migration.
Surgical Technique:
1. The patient is positioned prone on a radiolucent Jackson table.
2. A standard midline incision and subperiosteal dissection are performed, exposing the posterior elements.
3. Pedicle screws are inserted at least one level above and one level below the infected segment.
4. If a posterior epidural abscess is present, a laminectomy is performed for decompression.
5. Rods are contoured to restore physiological sagittal alignment and secured.
Clinical Pearl: When performing a laminectomy for an anteriorly situated infection without posterior instrumentation, you risk destabilizing the only remaining intact column. Always instrument if a laminectomy is performed in the setting of anterior column osteomyelitis.
3. Single-Stage vs. Two-Stage Procedures
- Single-Stage (Anterior-Posterior): Preferred in modern practice. The patient undergoes anterior debridement and grafting, followed immediately by posterior instrumentation under the same anesthetic.
- Two-Stage: Indicated in highly septic, hemodynamically unstable patients. The anterior debridement is performed first to achieve source control. The patient is resuscitated in the ICU, and posterior stabilization is performed 3 to 7 days later.
Specific Clinical Scenarios
Spinal Epidural Abscess (SEA)
SEA is a surgical emergency. The pathophysiology involves both direct mechanical compression of the spinal cord and septic thrombophlebitis of the epidural venous plexus, leading to spinal cord ischemia and irreversible infarction.
* Cervical/Thoracic SEA: Requires emergent surgical decompression (laminectomy for posterior abscesses, corpectomy for anterior abscesses) due to the narrow spinal canal.
* Lumbar SEA: May occasionally be managed medically if the patient is neurologically intact, but threshold for surgery must remain extremely low.
Pediatric Discitis
Unlike adults, children possess vascular channels that penetrate the cartilaginous endplate directly into the intervertebral disc. Consequently, pediatric discitis is often a primary infection of the disc itself.
* Presentation: Refusal to walk, irritability, loss of lumbar lordosis.
* Management: Overwhelmingly non-operative. Intravenous antibiotics followed by oral therapy and immobilization (e.g., spica cast or TLSO) yield excellent results. Surgery is strictly reserved for severe deformity or neurological compromise, which is exceedingly rare.
Postoperative Spinal Infections
Deep surgical site infections (SSIs) following spinal instrumentation occur in 1-4% of cases.
* Early Infections (< 30 days): Typically present with wound drainage, erythema, and fever. Management requires emergent return to the operating room for aggressive irrigation and debridement (I&D). Do not remove the instrumentation if it is rigidly fixed. Retained hardware can be sterilized in vivo with thorough debridement and prolonged culture-directed antibiotics.
* Delayed Infections (> 30 days): Often caused by low-virulence organisms (e.g., Cutibacterium acnes). If the fusion mass is solid, the instrumentation can be safely removed during the debridement.
Postoperative Protocols and Rehabilitation
Antimicrobial Therapy
Surgical debridement must be followed by a prolonged course of culture-directed antibiotics, managed in conjunction with an Infectious Disease specialist.
* Intravenous Phase: Typically 6 weeks of IV antibiotics via a peripherally inserted central catheter (PICC).
* Oral Phase: May be extended for an additional 6 to 12 weeks depending on the organism and the patient's clinical response.
Monitoring Efficacy
- CRP Kinetics: CRP levels should halve every 48 to 72 hours following successful surgical source control. A plateau or secondary rise in CRP warrants immediate re-evaluation with contrast-enhanced MRI to rule out recurrent abscess formation.
- ESR: Normalizes much slower than CRP and is less useful for acute postoperative monitoring.
Mobilization and Bracing
- Patients treated with rigid anterior-posterior instrumentation can typically be mobilized on postoperative day one without the need for external orthoses.
- Patients treated with anterior grafting alone or those with poor bone quality (osteoporosis) should be mobilized in a rigid Thoracolumbosacral Orthosis (TLSO) for 6 to 12 weeks to protect the graft until radiographic fusion is evident.
Conclusion
The operative management of spinal infections demands a profound understanding of spinal biomechanics, meticulous surgical technique, and aggressive medical management. The paradigm has shifted from prolonged immobilization to early, radical anterior debridement, structural reconstruction, and rigid posterior instrumentation. By adhering to these evidence-based principles, the orthopedic surgeon can reliably eradicate infection, decompress compromised neural elements, and restore the structural integrity of the spinal column, thereby optimizing patient outcomes in this challenging clinical arena.
📚 Medical References
- spinal infections. Spine State Art Rev 3:385, 1989.
- Lu J, Ebraheim NA, Nadim Y, et al: Anterior approach to the cervical spine: surgical anatomy, Orthopedics 23:841, 2000.
- Maciejczak A, Radke A, Kowalewski J, et al: Anterior transsternal approach to the upper thoracic spine, Acta Chir Hung 38:83, 1999.
- Mack MJ, Regan JJ, McAfee PC, et al: Video-assisted thoracic surgery for the anterior approach to the thoracic spine, Ann Thorac Surg 59:1100, 1995.
- McAfee PC, Bohlman HH, Riley LH Jr, et al: The
You Might Also Like