Proximal Row Carpectomy: Surgical Anatomy, Biomechanics & Indications

Key Takeaway
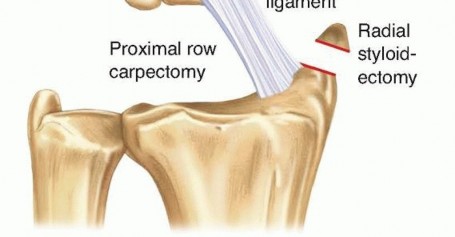
Proximal Row Carpectomy (PRC) is a wrist excisional arthroplasty involving removal of the scaphoid, lunate, and triquetrum. It converts the wrist into a radiocapitate articulation, treating advanced wrist degeneration such as SNAC and SLAC wrist, and Kienböck disease. PRC aims to preserve motion and alleviate pain while simplifying carpal kinematics.
Proximal Row Carpectomy
Introduction & Epidemiology
Proximal row carpectomy (PRC) is a well-established excisional arthroplasty of the wrist involving the removal of the scaphoid, lunate, and triquetrum. This procedure effectively converts a complex intercarpal articulation into a simplified radiocapitate articulation, aiming to preserve motion while alleviating pain associated with advanced pancarpal or radioscaphoid arthrosis. PRC is typically indicated for specific patterns of wrist degeneration where the lunate fossa of the radius and the head of the capitate remain relatively preserved.
The development of PRC as a viable surgical option arose from the understanding of specific degenerative pathways within the carpus. Conditions such as scaphoid nonunion advanced collapse (SNAC) and scapholunate advanced collapse (SLAC) wrist represent the most frequent indications for PRC. These conditions, along with advanced Kienböck disease, chronic perilunate dislocations, and scaphoid osteonecrosis, collectively represent a significant burden of wrist pathology leading to pain, decreased range of motion, and functional impairment. Epidemiologically, SLAC and SNAC wrists are the most common forms of degenerative wrist arthritis, often stemming from traumatic events like scaphoid fractures or scapholunate ligamentous dissociations. While a precise incidence of PRC is challenging to quantify due to variations in surgical indications and geographical practice patterns, it remains a cornerstone procedure in the armamentarium of reconstructive wrist surgeons, offering a balance between motion preservation and pain relief compared to more restrictive procedures like total wrist fusion. The success of PRC hinges on meticulous patient selection and precise surgical technique.
Surgical Anatomy & Biomechanics
The wrist joint is a highly complex articulation comprising eight carpal bones arranged into proximal and distal rows, articulating with the distal radius and ulna proximally, and the metacarpals distally.
Carpal Bones and Articulations
The proximal carpal row consists of the scaphoid, lunate, and triquetrum. The pisiform, located volar to the triquetrum, is functionally considered a sesamoid bone within the flexor carpi ulnaris (FCU) tendon. The scaphoid bridges the proximal and distal carpal rows, making it a critical component in carpal kinematics. The lunate articulates with the lunate fossa of the distal radius and the head of the capitate. The triquetrum articulates with the triquetral facet of the distal ulna via the triangular fibrocartilage complex (TFCC) and the hamate distally.
The distal carpal row comprises the trapezium, trapezoid, capitate, and hamate. The capitate is the largest carpal bone and forms a central pillar for carpal stability and motion. Its proximal articular surface, the capitate head, typically articulates with the lunate.
Ligamentous Structures
The stability of the carpus relies heavily on a complex network of intrinsic and extrinsic ligaments.
*
Intrinsic ligaments
: These connect carpal bones within a row or between rows. Key intrinsic ligaments include the scapholunate interosseous ligament (SLIL), lunotriquetral interosseous ligament (LTIL), and the capitohamate ligament. Degeneration or rupture of these ligaments, particularly the SLIL, is central to the development of SLAC wrist.
*
Extrinsic ligaments
: These connect the carpal bones to the radius or metacarpals. Important extrinsic ligaments on the volar side include the radioscaphocapitate (RSC), long radiolunate (LRL), short radiolunate (SRL), and ulnotriquetral (UT) ligaments. On the dorsal side, the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments are crucial. The integrity of the volar extrinsic ligaments, particularly the RSC, is critical for maintaining stability of the capitate after PRC by preventing volar subluxation of the capitate head relative to the lunate fossa of the radius.

Neurovascular Considerations
The dorsal wrist capsule is supplied by branches of the posterior interosseous artery and nerve. The radial artery courses volarly near the scaphoid. The superficial radial nerve and dorsal sensory branch of the ulnar nerve are vulnerable during dorsal approaches. Careful dissection is required to protect these structures.
Biomechanics of the Carpus and Post-PRC State
Normal carpal kinematics involve a synchronous movement of the proximal row relative to the distal radius and a complex interplay between the proximal and distal rows. The proximal row is often described as an intercalated segment without direct muscular attachments, moving primarily under the influence of forces transmitted through the distal row and the surrounding ligaments. The proximal row flexes with radial deviation and extends with ulnar deviation.
In PRC, the scaphoid, lunate, and triquetrum are removed, effectively eliminating the proximal carpal row. The new articulation is formed between the head of the capitate and the lunate fossa of the distal radius. This transformation simplifies the carpus from two rows to a single functional row composed of the distal carpal bones. The success of this new articulation depends on several factors:
*
Congruity
: The proximal capitate articular surface is relatively, although not completely, congruous with the lunate facet of the radius. Some degree of incongruity is expected, but excessive incongruity, especially if associated with pre-existing radial lunate fossa chondromalacia, can lead to persistent pain and early progression of arthritis.
*
Ligamentous Support
: The integrity of the volar extrinsic ligaments, particularly the radioscaphocapitate ligament, is paramount. This ligament prevents volar subluxation of the capitate and helps to centralize the capitate head within the lunate fossa, ensuring stable tracking during wrist motion.
*
Capsular Integrity
: A robust dorsal and volar capsular repair contributes significantly to the stability of the new radiocapitate joint.
*
Range of Motion
: PRC typically preserves approximately 50-60% of pre-injury range of motion and 70-80% of grip strength compared to a normal wrist. This is superior to total wrist fusion and comparable to, or slightly better than, four-corner fusion in some metrics.

Indications & Contraindications
PRC is indicated for degenerative wrist conditions where the pathology primarily involves the radiocarpal and midcarpal joints but spares the lunate fossa of the radius and the capitate head. The primary goal is pain relief while preserving a functional range of motion.
Indications
-
Scaphoid Nonunion Advanced Collapse (SNAC) Wrist
: This common condition arises from a long-standing scaphoid nonunion leading to altered carpal kinematics. The scaphoid collapses into a flexed posture, causing abutment and degenerative changes between the scaphoid and the radial styloid, and subsequent midcarpal arthritis between the capitate and the abnormally positioned scaphoid. This eventually progresses to radiocarpal arthritis.

-
Scapholunate Advanced Collapse (SLAC) Wrist
: Resulting from chronic scapholunate ligament dissociation, the scaphoid assumes a volar flexed (DISI) posture, leading to similar degenerative changes as SNAC. Arthritis typically initiates at the radioscaphoid joint, progresses to the capitolunate articulation, and eventually involves the entire midcarpal joint.

-
Kienböck Disease (Stage IIIb and IV)
: Avascular necrosis of the lunate. In advanced stages (IIIb with carpal collapse, IV with pancarpal arthritis), PRC can provide pain relief by removing the necrotic lunate and establishing a new articulation. It is crucial to ensure the capitate head and lunate fossa are well-preserved.
- Chronic or Missed Perilunate Dislocation : When carpal instability has led to irrecoverable articular damage of the proximal carpal row, PRC can be a salvage option, provided the radial lunate fossa and capitate head are suitable.
- Scaphoid Osteonecrosis or Preiser Disease : Avascular necrosis of the scaphoid in the absence of a fracture, leading to collapse and subsequent arthrosis.
- Wrist Deformity or Contracture : In select cases where the primary pathology involves irreparable damage to the proximal carpal row leading to degenerative arthritis, PRC may be considered.
Contraindications
- Degeneration of the Lunate Fossa of the Radius : The most critical contraindication. If there is significant chondromalacia, osteochondral defects, or eburnation of the lunate fossa, the new radiocapitate articulation will fail, leading to continued pain and rapid progression of arthritis. This must be carefully assessed pre-operatively with imaging (e.g., CT or MRI) and intra-operatively.
- Degeneration of the Capitate Head : Similar to radial fossa degeneration, significant arthritic changes on the capitate head will compromise the success of the PRC.
- Pan-carpal Arthritis : While PRC addresses proximal carpal pathology, if there is widespread severe arthritis involving the distal carpal row (e.g., capito-hamate joint, trapezio-trapezoid joint, etc.) that will not be alleviated by proximal row excision, other procedures like total wrist fusion may be more appropriate.
- Significant Carpal Collapse : While PRC is performed for collapsed wrists (SNAC/SLAC), severe, long-standing collapse with significant adaptive changes in the distal carpal row and radius may make stable reduction of the capitate into the radial lunate fossa challenging or impossible.
- Infection : Active wrist infection is an absolute contraindication to elective arthroplasty.
- Inadequate Patient Compliance/Rehabilitation Potential : Patients must be able to adhere to a post-operative rehabilitation protocol.
- Voluntary Wrist Dislocation : A rare contraindication where extreme laxity or voluntary dislocation precludes stable radiocapitate articulation.
Table: Indications and Contraindications for Proximal Row Carpectomy
| Category | Indication for Proximal Row Carpectomy | Contraindication for Proximal Row Carpectomy |
|---|---|---|
| Pathology | SNAC wrist (Stage II-IV) | Significant degeneration/arthrosis of the radial lunate fossa |
| SLAC wrist (Stage II-IV) | Significant degeneration/arthrosis of the capitate head | |
| Kienböck disease (Stage IIIb-IV) with preserved radiocapitate joint | Pre-existing severe pancarpal arthritis (beyond radiocapitate involvement) | |
| Chronic/missed perilunate dislocation with salvageable articular surfaces | Active wrist infection | |
| Scaphoid osteonecrosis/Preiser disease with preserved radiocapitate joint | Significant collapse precluding stable capitate-radius articulation | |
| Post-traumatic arthritis primarily involving the proximal row | Severe osteoporosis or osteopenia complicating fixation (if used) | |
| Patient Factors | Persistent pain and limited function refractory to conservative management | Unrealistic patient expectations regarding motion or pain relief |
| Desire for motion preservation (compared to fusion) | Inability or unwillingness to comply with post-operative rehabilitation | |
| Adequate bone stock and soft tissue envelope | ||
| Imaging Findings | Preserved cartilage of the radial lunate fossa and capitate head on imaging | Evidence of advanced chondromalacia or eburnation on imaging (CT/MRI) |
| Extensive distal carpal pathology that would not be addressed |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is essential for a successful PRC.
Pre-Operative Planning
- Clinical Assessment : Detailed history of pain, functional limitations, prior treatments, and physical examination including range of motion, grip strength, and neurovascular status.
-
Radiographic Evaluation
:
- Standard PA, lateral, and oblique views : To assess carpal alignment, collapse patterns (e.g., dorsal intercalated segmental instability - DISI in SLAC), and initial signs of arthritis. A true lateral view is critical for assessing carpal collapse.
- Wrist traction views : Can sometimes help to open up the joint space and better visualize articular surfaces.
-
Advanced Imaging
:
- CT scan : The gold standard for evaluating bone morphology and articular cartilage integrity, particularly the lunate fossa of the radius and the capitate head. It provides detailed assessment of osteophytes and degenerative changes.
- MRI scan : Useful for assessing soft tissue structures (ligaments, TFCC) and early chondral changes, as well as evaluating for avascular necrosis.
- Arthrography : Rarely used now but can delineate ligamentous injuries.
- Patient Counseling : Comprehensive discussion of the goals of surgery (pain relief, motion preservation), expected outcomes, potential complications, and post-operative rehabilitation. Manage expectations regarding complete pain elimination or full restoration of motion.
- Anesthesia Consultation : General anesthesia is typical, often with a regional block (e.g., interscalene or axillary block) for post-operative pain management.
Patient Positioning
- Supine Position : The patient is positioned supine on the operating table.
- Hand Table : The ipsilateral upper extremity is abducted onto a specialized hand table, providing adequate space for surgical manipulation and fluoroscopy.
- Tourniquet : A pneumatic tourniquet is applied to the upper arm for maintaining a bloodless field.
- Arm Positioning : The forearm is typically pronated to allow optimal access to the dorsal aspect of the wrist. Some surgeons prefer a neutral position or slight supination depending on their specific approach. Padding is meticulously applied to pressure points.
- Fluoroscopy : The C-arm image intensifier is positioned to allow real-time intraoperative radiographic assessment, typically in PA and lateral planes.
Detailed Surgical Approach / Technique
Proximal row carpectomy is typically performed via a dorsal longitudinal approach to the wrist.
1. Incision and Exposure
-
Skin Incision
: A straight or slightly curvilinear longitudinal incision is made over the dorsal wrist, typically centered just ulnar to Lister's tubercle, extending from the distal radius to the base of the third metacarpal. This allows access while minimizing neurovascular injury.
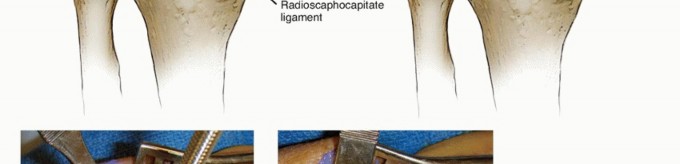
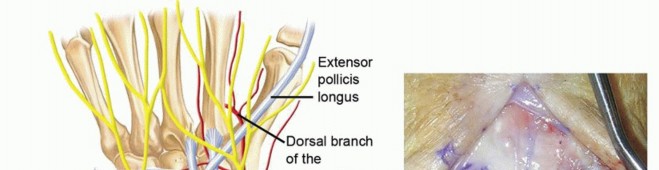
- Superficial Dissection : Meticulous dissection through the subcutaneous tissue. Identify and protect the dorsal sensory branch of the radial nerve radially and the dorsal sensory branch of the ulnar nerve ulnarly. These structures are highly variable in their course and susceptible to iatrogenic injury.
-
Extensor Retinaculum
: The extensor retinaculum is identified. The interval between the third (extensor pollicis longus, EPL) and fourth (extensor digitorum communis, EDC) dorsal compartments is typically chosen for capsular access. Alternatively, the interval between the second (extensor carpi radialis longus/brevis, ECRL/ECRB) and third compartments can be used, particularly if radial styloidectomy is also planned.
-
The retinaculum can be incised longitudinally over the chosen interval. A common technique is to incise the retinaculum and reflect it as a flap, often based radially or ulnarly, to be repaired at closure.

-
The retinaculum can be incised longitudinally over the chosen interval. A common technique is to incise the retinaculum and reflect it as a flap, often based radially or ulnarly, to be repaired at closure.
-
Tendon Management
: The extensor tendons (typically EDC) in the fourth compartment are retracted radially. The EPL (third compartment) may be retracted ulnarly. Care is taken to avoid excessive tension on the tendons.

2. Capsulotomy
-
Dorsal Wrist Capsule
: A longitudinal capsulotomy is performed. It is crucial to preserve the important volar extrinsic ligaments, particularly the radioscaphocapitate ligament. The dorsal capsule can be incised and elevated as an H-shaped flap or a single longitudinal flap, to be repaired later. Care is taken not to over-dissect the volar capsule, which provides essential stability to the new radiocapitate articulation.

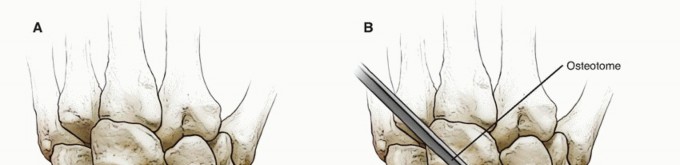
3. Excision of the Proximal Carpal Row
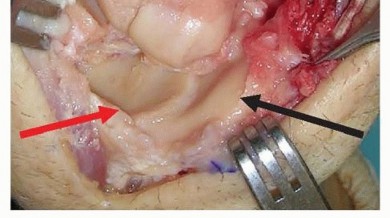
- Initial Assessment : Once the capsule is opened, the degenerative changes of the proximal carpal row and their articulation with the distal radius and capitate head are assessed.
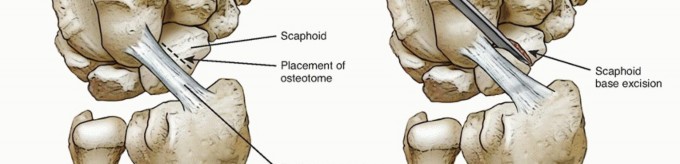
-
Scaphoid Excision
: The scaphoid is typically removed first.
- The dorsal aspect of the scapholunate interosseous ligament is identified and carefully transected.
- The dorsal radiocarpal ligaments are incised as needed to mobilize the scaphoid.
- Using small osteotomes, rongeurs, and curved scissors, the scaphoid is carefully dissected free from its ligamentous attachments (both intrinsic and extrinsic) and delivered from the wound.
-
Attention should be paid to the deep volar radioscaphocapitate ligament, which should be preserved.

-
Lunate Excision
: Following scaphoid removal, the lunate is more accessible.
- The remaining portions of the scapholunate ligament and the lunotriquetral ligament are transected.
- The dorsal radiolunate ligamentous attachments are carefully released.
-
The lunate is extracted.

-
Triquetrum Excision
: The triquetrum is typically the most challenging bone to remove due to its deeper and more ulnar position.
- The lunotriquetral ligament and dorsal radiocarpal ligament attachments are already partially released.
- Carefully release the triquetrum from its articulation with the hamate and any remaining ulnar attachments (e.g., ulnotriquetral ligament dorsally).
-
A small elevator or curved rongeur can facilitate its removal.

- Bone Fragment Removal : Meticulously inspect the joint for any remaining small bone fragments or osteophytes, which could cause impingement or irritation.
4. Assessment and Articular Surface Preparation
-
Radial Lunate Fossa and Capitate Head
: With the proximal row removed, the lunate fossa of the distal radius and the head of the capitate are now fully exposed. This is the critical stage for assessing their articular cartilage.
- Inspect for any chondromalacia, eburnation, or significant osteophytes. If severe damage to either surface is noted at this stage, the suitability of PRC must be re-evaluated.
- Minor osteophytes on the radial styloid or capitate head can be removed with a rongeur or small osteotome.
-
If significant chondral damage is discovered on the radial lunate fossa, a switch to a four-corner fusion or total wrist fusion may be indicated, or a concomitant radial styloidectomy may be performed if the damage is primarily radial-sided.
5. Creation of the New Articulation and Stabilization
-
Capitate Reduction
: Gently reduce the head of the capitate into the lunate fossa of the radius. The goal is to achieve a concentric, stable, and smooth articulation throughout the arc of wrist motion.
- Maneuver the wrist through flexion, extension, radial deviation, and ulnar deviation to ensure the capitate tracks smoothly within the radial fossa without impingement.
-
Pay particular attention to the midcarpal stability. The capitate should not sublux volarly. The integrity of the volar radioscaphocapitate ligament is crucial here.

-
K-wire Stabilization (Optional)
: While not universally performed, some surgeons opt to temporarily stabilize the capitate in the radial fossa with a 0.045" or 0.062" K-wire for 3-4 weeks, especially if initial stability feels suboptimal. This can be placed from the distal capitate into the radial shaft or from the dorsal capitate into the distal radius. This practice is less common now, as the preserved soft tissues are generally sufficient for stability.
6. Closure
- Capsular Repair : The dorsal wrist capsule is meticulously repaired using non-absorbable sutures (e.g., 2-0 or 3-0 braided non-absorbable). A strong capsular repair is paramount for providing dorsal stability to the new radiocapitate joint.
- Extensor Retinaculum Repair : The incised extensor retinaculum is repaired. If it was incised longitudinally, it can be oversewn. If a flap was created, it is reapproximated. Some surgeons may perform a Z-lengthening of the retinaculum if there is concern for extensor tendon impingement post-PRC, though this is rare.
- Subcutaneous and Skin Closure : Standard layered closure of the subcutaneous tissues and skin.
- Dressing and Splint : A sterile dressing is applied, followed by a well-padded sugar-tong splint or short arm cast, maintaining the wrist in a neutral position for initial immobilization.
Complications & Management
While PRC is generally a reliable procedure, a range of complications can occur. Understanding these and their management is crucial for optimal patient care.
Common Complications and Management
| Complication | Incidence (Approximate) | Salvage Strategies / Management |
|---|---|---|
| Progressive Radiocapitate Arthritis | 10-30% long-term | Most common reason for failure. Initial management: activity modification, NSAIDs, steroid injections. Surgical options: Total wrist fusion (most reliable for pain relief), four-corner fusion (if distal carpal row is pristine, rare as salvage for failed PRC), wrist denervation . |
| Persistent Pain | 5-20% | Rule out specific causes (e.g., hardware irritation, nerve entrapment, residual osteophytes, early arthritis). Management: conservative measures, targeted injections. Salvage: as above for progressive arthritis, radial styloidectomy if impingement. |
| Stiffness / Limited Range of Motion | Common | Aggressive hand therapy and stretching exercises. Dynamic splinting. Surgical: Capsular release, tenolysis. If severe and painful, conversion to total wrist fusion. |
| Decreased Grip Strength | Common | Physiotherapy focusing on strengthening. Often correlates with pain and stiffness. May improve with time and therapy, but some deficit is expected. |
| Nerve Injury | <5% (sensory) | Dorsal sensory branch of radial nerve or dorsal sensory branch of ulnar nerve paresthesias/neuroma. Management: observation for spontaneous recovery, nerve blocks, desensitization therapy. Surgical: neurolysis, neurectomy, or neuroma excision. |
| Infection | <1% | Superficial: wound care, oral antibiotics. Deep: surgical debridement, IV antibiotics. May necessitate hardware removal (if used) and rarely, further salvage surgery or total wrist fusion. |
| Extensor Tendon Irritation/Rupture | Rare | Due to prominent hardware (if used) or scar tissue. Management: removal of hardware, tenolysis. Tendon rupture requires repair or graft. |
| Capitate Instability/Subluxation | Rare | Typically volar subluxation if volar ligaments are compromised. Management: immobilization. If persistent and symptomatic: surgical capsular tightening, reconstruction of volar ligaments, or conversion to total wrist fusion. |
| CRPS (Complex Regional Pain Syndrome) | Rare | Early recognition and multidisciplinary management: physiotherapy, pharmacotherapy (e.g., gabapentin, amitriptyline), nerve blocks, psychological support. |
Discussion of Complications
The most significant long-term concern following PRC is the development of progressive arthritis between the capitate head and the lunate fossa of the radius. This risk is notably higher if there was pre-existing cartilage damage on these surfaces at the time of the initial surgery, highlighting the critical importance of meticulous pre-operative and intra-operative assessment. Patients should be counseled that PRC may not be a permanent solution and that a secondary procedure, most commonly total wrist fusion, may be necessary in the long term.
Stiffness and decreased grip strength are expected to some degree, and patients should be prepared for this. Active and passive range of motion exercises initiated early in the post-operative period are key to minimizing this complication. Nerve injury, while uncommon, can be debilitating, emphasizing the need for careful soft tissue dissection.
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation program is critical for maximizing outcomes following PRC. The protocol aims to protect the surgical site while restoring motion, strength, and function.
Phase 1: Immobilization and Protection (Weeks 0-3/4)
- Goal : Protect the surgical site, minimize pain and swelling, allow soft tissue healing.
-
Immobilization
: A well-padded sugar-tong splint or short arm cast is applied post-operatively, maintaining the wrist in neutral to slight extension. The digits should remain free for motion.
- If K-wire fixation was used, wires are typically removed at 3-4 weeks.
- Elevation : Maintain the hand elevated above the heart to minimize swelling.
- Pain Management : Administer appropriate analgesia.
-
Early Motion (Active)
:
- Finger flexion/extension : Immediately begin gentle, active range of motion (AROM) exercises for the digits to prevent stiffness.
- Forearm rotation : Active pronation and supination, if comfortable and allowed by the splint/cast, to maintain elbow and forearm mobility.
- Shoulder/Elbow : Active range of motion for the shoulder and elbow to prevent stiffness.
- Wound Care : Keep the surgical site clean and dry. Monitor for signs of infection.
Phase 2: Early Motion and Scar Management (Weeks 3/4 - 6)
- Goal : Gradually increase wrist range of motion, initiate scar management, reduce edema.
- Splint Removal : The immobilization splint/cast is typically removed. A removable custom or prefabricated wrist splint is provided for protection during activity and at night.
-
Active Range of Motion (AROM) - Wrist
:
- Begin gentle, active flexion, extension, radial, and ulnar deviation of the wrist. The emphasis is on pain-free movement.
- Encourage smooth, controlled motions, avoiding jerky movements or forced stretching.
-
Passive Range of Motion (PROM) - Wrist
:
- Under the guidance of a hand therapist, gentle passive range of motion can be introduced as tolerated.
- Scar Management : Initiate scar massage to prevent adhesions.
- Edema Control : Continue with elevation, compression, and gentle massage as needed.
- Light Gripping : Gentle squeezing of a soft sponge or putty can be introduced to begin activating intrinsic hand muscles.
Phase 3: Strengthening and Functional Integration (Weeks 6-12)
- Goal : Progress to strengthening, normalize range of motion, improve functional use of the hand.
-
Strengthening Exercises
:
- Introduce light resistance exercises for wrist flexion, extension, and deviation using elastic bands, light weights, or putty.
- Progress to grip strengthening exercises (e.g., squeeze ball, hand grippers).
- Forearm pronation/supination with resistance.
- Advanced Range of Motion : Continue to work on achieving full pain-free AROM and PROM. Dynamic splinting may be considered if stiffness persists.
- Functional Activities : Incorporate activities of daily living (ADLs) that gradually increase the demands on the wrist.
- Proprioception/Coordination : Exercises to improve fine motor control and coordination.
Phase 4: Return to Activity (Weeks 12+)
- Goal : Progress to full strength, endurance, and return to work/sport-specific activities.
- Progressive Loading : Gradually increase the intensity and duration of strengthening exercises.
- Sport/Work-Specific Training : Tailor the rehabilitation program to the patient's specific vocational or avocational demands. This may involve specific drills or simulations.
- Endurance Training : Exercises designed to build wrist and forearm endurance.
- Return to Activity : A gradual return to strenuous activities, lifting, and sports, typically cleared by the surgeon based on objective measures of strength, motion, and the absence of pain. Full unrestricted activity may not be achieved for 4-6 months, or sometimes longer.
Throughout the rehabilitation process, close communication between the surgeon and the hand therapist is essential to tailor the program to the individual patient's progress and specific needs. Patient education on proper body mechanics and activity modification remains crucial for long-term success.
Summary of Key Literature / Guidelines
Proximal row carpectomy has been a subject of extensive research, particularly comparing its outcomes to other motion-sparing procedures like four-corner fusion (4CF) and to total wrist fusion (TWF).
Long-Term Outcomes and Comparison with Other Procedures
- Pain Relief : Most studies consistently report good to excellent pain relief in 70-90% of patients undergoing PRC for appropriate indications. This is comparable to 4CF.
- Range of Motion : PRC typically preserves more wrist motion (especially flexion-extension arc, often 50-60% of the contralateral wrist) than 4CF, which tends to be more restrictive. A 2007 meta-analysis by Strauch et al. found that PRC resulted in greater mean flexion-extension arc (approximately 60°) compared to 4CF (approximately 45°).
- Grip Strength : Grip strength post-PRC is generally reported to be 70-80% of the contralateral side, which is comparable to 4CF.
- Complication Rates : Both PRC and 4CF have similar overall complication profiles, with progressive arthritis being the most common long-term issue for PRC, and nonunion for 4CF.
-
Progression to Arthritis
: Long-term follow-up studies, such as those by Culp and Osterman (2000) and Wyrick et al. (2018), have shown that progressive radiocapitate arthritis remains the primary reason for failure of PRC, often necessitating conversion to total wrist fusion in 10-30% of patients over 10-20 years. However, many patients achieve satisfactory long-term outcomes without needing further surgery.
- An important factor influencing the longevity of PRC is the pre-existence of chondromalacia of the capitate head or radial lunate fossa. Studies have demonstrated a significantly higher failure rate when these surfaces are not pristine at the time of surgery.
- Patient Satisfaction : High patient satisfaction rates are generally reported for PRC, often reflecting the preservation of useful motion and reduction in pain.
Clinical Guidelines and Recommendations
- Patient Selection : Current guidelines emphasize meticulous patient selection, particularly the critical assessment of the lunate fossa of the radius and the capitate head. A well-preserved radiocapitate joint is the single most important predictor of successful PRC outcomes. Advanced imaging (CT/MRI) is highly recommended for this assessment.
- Indications : PRC is a preferred motion-sparing option for SNAC, SLAC (Stages II-IV), and advanced Kienböck disease (Stages IIIb-IV) when the radiocapitate joint is healthy.
- Comparison to 4CF : The choice between PRC and 4CF often depends on surgeon preference, the specific pattern of arthritis, and the desired balance between motion and pain relief. Some argue that 4CF, by fusing the distal carpal row to the lunate, offers a more stable base, potentially leading to fewer long-term complications related to instability. However, 4CF is associated with higher rates of nonunion and less range of motion.
- Salvage Procedures : For failed PRC due to progressive arthritis, total wrist fusion remains the most reliable salvage procedure for achieving pain relief, though at the cost of all wrist motion.
Emerging Concepts and Future Directions
- Articular Cartilage Preservation : Research continues into strategies for improving the longevity of the radiocapitate articulation, including biological augmentation, use of interpositional materials, or resurfacing techniques, though these are largely experimental.
- Biomechanics : Further studies continue to refine our understanding of post-PRC carpal kinematics, with advanced imaging and computational modeling.
- Patient-Reported Outcomes (PROs) : Increasing emphasis on PROs as a measure of success, providing a more holistic view of patient benefit beyond traditional clinical metrics.
In conclusion, PRC remains a valuable and effective procedure for carefully selected patients with degenerative wrist conditions primarily affecting the proximal carpal row while sparing the key radiocapitate articulation. Its success hinges on precise surgical technique and a thorough understanding of carpal anatomy, biomechanics, and long-term outcomes.


Clinical & Radiographic Imaging

