Comprehensive Orthopedic Review | Dr Hutaif General Ort -...
Key Takeaway
Learn more about Bop and how to manage it. A patient often has sustained a complex injury pattern when a comminuted coronoid fracture is present, which must be distinguished from a simpler olecranon fracture. Loss of the coronoid buttress can lead to residual elbow instability. If initial stabilization fails, revision surgery is crucial, focusing on stabilizing the coronoid and assessing collateral ligaments to restore joint congruity and stability.
Comprehensive Orthopedic Review | Dr. Hutaif's General Orthopedic Principles: Advanced Management of Complex Elbow Instability and Coronoid Fractures
Introduction & Epidemiology
Complex elbow instability represents a spectrum of challenging injuries characterized by disruption of multiple static and dynamic stabilizers of the elbow joint. These injuries frequently involve osseous pathology, particularly coronoid fractures, in conjunction with significant ligamentous disruption. The term "terrible triad injury" (radial head fracture, coronoid fracture, and lateral ulnar collateral ligament (LUCL) injury) is a well-recognized subset, but other patterns such as trans-olecranon fracture-dislocations with coronoid involvement also present significant management dilemmas. The common unifying factor is a compromised ulnohumeral articulation, often compounded by radial head and collateral ligament deficiencies, leading to persistent instability and a high propensity for poor outcomes if not adequately addressed.
The incidence of elbow fracture-dislocations is relatively low compared to other joint injuries, but the functional implications are substantial, particularly given the elbow's critical role in upper extremity function. These are typically high-energy trauma events, often resulting from a fall onto an outstretched hand (FOOSH) with an axial load, valgus or varus stress, and rotational forces. The complexity of these injuries necessitates a thorough understanding of elbow anatomy, biomechanics, and a systematic approach to diagnosis and treatment. Inadequate initial assessment or sub-optimal surgical management, as highlighted by the original seed content regarding failed bony stabilization of the coronoid, can lead to chronic instability, stiffness, post-traumatic arthritis, and significant functional impairment. The coronoid process, specifically, serves as a critical anterior buttress against posterior subluxation of the ulna on the humerus and provides attachment for the anterior bundle of the medial collateral ligament (MCL) and the joint capsule. Its integrity is paramount for maintaining ulnohumeral stability.
Surgical Anatomy & Biomechanics
A profound understanding of the intricate osseous and soft tissue anatomy of the elbow is fundamental to the successful management of complex instability patterns.
Osseous Anatomy
The elbow joint comprises three articulations within a single synovial capsule: the ulnohumeral, radiohumeral, and radioulnar joints.
*
Humerus:
The distal humerus features the trochlea medially (articulating with the ulna) and the capitellum laterally (articulating with the radial head). The trochlea is critical for ulnohumeral congruity, and its shape dictates the elbow's arc of motion. The medial and lateral epicondyles serve as origins for collateral ligaments and muscle groups.
*
Ulna:
*
Olecranon:
Forms the posterior aspect of the trochlear notch, providing a posterior buttress and the primary attachment for the triceps. Fractures here often disrupt the joint surface and overall stability.
*
Coronoid Process:
This anterior projection from the proximal ulna is arguably the most critical bony stabilizer against posterior translation and varus stress. Its anterior facet articulates with the trochlea. The sublime tubercle, located at its anteromedial base, is the primary attachment site for the anterior bundle of the MCL. Fractures of the coronoid are classified by Regan and Morrey (Type I: tip, Type II: <50% articular, Type III: >50% articular) and O'Driscoll et al. (Type I: tip/anteromedial, Type II: anterolateral, Type III: basal). The anteromedial facet of the coronoid, often involved in terrible triad injuries, contributes significantly to stability.
*
Radius:
*
Radial Head:
The concave articular surface articulates with the capitellum. The radial head functions as a secondary stabilizer to valgus stress and axial load. Fractures of the radial head are common and contribute significantly to instability, particularly in terrible triad injuries. Its absence or malreduction can lead to increased stress on the collateral ligaments and recurrent instability.
Ligamentous Anatomy
The primary soft tissue stabilizers are the medial and lateral collateral ligament complexes.
*
Medial Collateral Ligament (MCL) Complex:
The primary restraint to valgus stress.
*
Anterior Bundle (aMCL):
The strongest and most critical component, taut throughout the entire range of motion, originating from the anterior aspect of the medial epicondyle and inserting onto the sublime tubercle of the coronoid. Its integrity is paramount for elbow stability, especially for resisting valgus forces.
*
Posterior Bundle (pMCL):
Taut in flexion, contributes to stability in flexion beyond 90 degrees.
*
Transverse Ligament (Cooper's Ligament):
Intracapsular, offers little to no stability.
*
Lateral Collateral Ligament (LCL) Complex:
The primary restraint to varus stress and posterolateral rotatory instability (PLRI).
*
Lateral Ulnar Collateral Ligament (LUCL):
The critical component, originating from the lateral epicondyle and inserting onto the supinator crest of the ulna. Disruption of the LUCL is central to posterolateral rotatory instability and is universally present in terrible triad injuries.
*
Radial Collateral Ligament (RCL):
Originates from the lateral epicondyle, blends with the annular ligament.
*
Annular Ligament:
Encircles the radial head, maintaining its articulation with the ulna.
*
Accessory Lateral Collateral Ligament (ALCL):
Extends from the annular ligament to the supinator crest.
Biomechanics of Stability
Elbow stability is a complex interplay of osseous congruity, ligamentous integrity, and surrounding musculature.
*
Primary Stabilizers (50% contribution):
* Ulnohumeral articulation (especially coronoid buttress and trochlear depth).
* Anterior bundle of the MCL.
* LUCL.
*
Secondary Stabilizers (50% contribution):
* Radial head (provides a significant contribution to valgus stability and axial load bearing).
* Joint capsule.
* Muscular origins and insertions around the elbow (flexor-pronator mass medially, extensor-supinator mass laterally).
The mechanism of injury often dictates the pattern of instability. A FOOSH injury with supination and valgus stress typically leads to posterolateral rotatory instability, sequentially disrupting the LUCL, then tearing the anterior capsule, and finally leading to coronoid fracture (typically anteromedial coronoid) and radial head fracture, culminating in the terrible triad. The coronoid acts as a key anterior buttress. Loss of this buttress, even with an intact radial head and collateral ligaments, can lead to recurrent subluxation or dislocation. If the initial bony stabilization of the coronoid fails, as described in the seed content, the primary buttress against posterior subluxation is lost, necessitating revision with particular attention to restoring the coronoid. The critical importance of assessing and repairing/reconstructing collateral ligaments, particularly the LUCL in posterolateral rotatory instability and the aMCL in valgus instability, cannot be overstated.
Indications & Contraindications
The decision-making process for operative versus non-operative management of complex elbow instability is contingent upon numerous factors, primarily the stability of the elbow after initial assessment and reduction, the displacement and size of coronoid and radial head fractures, and the integrity of the collateral ligaments.
Indications for Operative Management
- Elbow Instability: Any elbow that remains unstable after closed reduction, or that dislocates or subluxes through a functional arc of motion (e.g., 30-100 degrees of flexion).
-
Displaced Coronoid Fractures:
- Regan & Morrey Type II or III fractures, particularly if displaced >2mm or involving >10-15% of the articular surface.
- O'Driscoll Type I (anteromedial facet) fractures, especially if involving the sublime tubercle and associated with instability, often requiring repair or internal fixation to re-establish MCL integrity.
- O'Driscoll Type II (anterolateral) and Type III (basal) fractures with significant displacement or comminution, particularly if they compromise the ulnohumeral articulation.
- Terrible Triad Injuries: Displaced radial head fracture, coronoid fracture, and LUCL disruption. This is almost universally an operative indication.
- Trans-Olecranon Fracture-Dislocations: These complex injuries combine olecranon and coronoid fractures with elbow dislocation, requiring meticulous anatomical reduction and stable fixation.
- Open Fractures: Require urgent surgical debridement and stabilization.
- Neurovascular Compromise: Acute neurovascular injury necessitates immediate surgical exploration and repair.
- Failure of Prior Fixation: As highlighted in the original seed content, failed bony stabilization, especially of the coronoid, necessitates revision to restore the articular buttress and overall stability. This often involves removal of failed hardware, debridement, potential bone grafting, and more robust fixation.
- Gross Joint Incongruity: Articular step-off or gap that cannot be anatomically reduced non-operatively.
Contraindications for Operative Management
- Non-displaced, Stable Coronoid Fractures: Regan & Morrey Type I fractures or other coronoid fractures that are non-displaced and do not result in instability when tested through a full range of motion.
- Stable Reduced Elbow: If the elbow can be concentrically reduced and remains stable through a functional arc of motion (e.g., 30-100 degrees of flexion), non-operative management with controlled early motion may be considered.
- Severe Patient Comorbidities: Medical conditions that preclude safe surgical intervention.
- Severe Soft Tissue Compromise: Extensive open wounds, severe degloving injuries, or impending compartment syndrome may necessitate staged surgical approaches or external fixation initially to allow soft tissue recovery before definitive internal fixation. Active infection is an absolute contraindication to immediate internal fixation.
Operative vs. Non-Operative Indications
| Feature | Operative Indication | Non-Operative Indication |
|---|---|---|
| Elbow Stability | Unstable after closed reduction; persistent subluxation/dislocation | Stable after closed reduction, through functional ROM (0-120 deg) |
| Coronoid Fracture Type | Regan & Morrey Type II/III; O'Driscoll Type I (anteromedial facet) with instability | Regan & Morrey Type I (tip), non-displaced, stable |
| Coronoid Displacement | >2mm articular displacement; significant comminution compromising buttress | <2mm non-articular displacement, stable |
| Associated Injuries | Radial head fracture (displaced/comminuted); LCL/MCL disruption (e.g., terrible triad) | Isolated injury without significant ligamentous instability |
| Open Fracture | Present (urgent operative debridement and stabilization) | Absent |
| Neurovascular Compromise | Present (urgent exploration and repair) | Absent |
| Soft Tissue Status | Stable, amenable to open approach | Unstable, severe swelling, extensive degloving (may need staging) |
| Prior Fixation Failure | Documented hardware failure, non-union, or recurrent instability | - |
| Articular Incongruity | Significant step-off or gap leading to instability | Concentric reduction with minimal step-off (<1-2mm) |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for anticipating challenges and optimizing outcomes in complex elbow instability cases.
Imaging
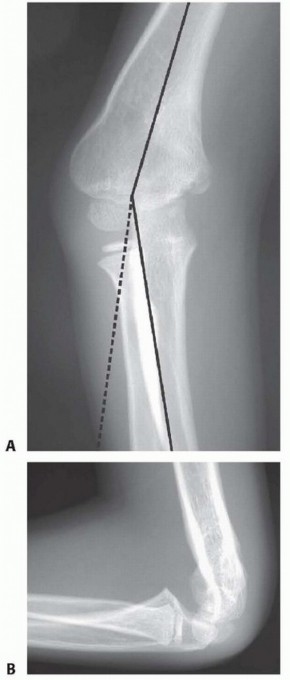
- Standard Radiographs: AP, lateral, and oblique views of the elbow are the initial screening tools. These provide basic information on fracture patterns, dislocation, and gross alignment. Stress views (valgus/varus) under fluoroscopy may be cautiously performed in the emergency setting after reduction to assess collateral ligament integrity, though this is often deferred until surgical exploration.
-
Computed Tomography (CT) Scan:
Indispensable for complex elbow fracture-dislocations. A high-resolution CT scan with 3D reconstructions provides detailed information regarding:
- Coronoid fracture morphology, size, and displacement (especially anteromedial facets).
- Radial head fracture pattern and comminution.
- Olecranon fracture pattern and articular involvement.
- Articular congruity and presence of intra-articular loose bodies.
-
This imaging modality helps immensely in surgical planning for plate and screw placement.

- Magnetic Resonance Imaging (MRI): Less frequently used acutely but can be beneficial if ligamentous injuries are suspected but not clearly delineated by clinical examination or stress radiographs, particularly in chronic instability or if occult pathology is suspected.
Pre-operative Templating and Equipment
- Fracture-Specific Implants: Review CT scans to template appropriate plates and screws for coronoid, radial head, and olecranon fractures. Small fragment sets (1.5, 2.0, 2.4 mm screws, specialty coronoid plates, hook plates) are typically required.
- Ligamentous Repair/Reconstruction: Suture anchors (2.0-3.5 mm) for epicondylar reattachment of MCL and LUCL, high-strength sutures for direct repair, or graft material for reconstruction (e.g., palmaris longus, gracilis) if primary repair is not feasible, especially in revision cases.
- Radial Head Replacement: If radial head fixation is not possible (e.g., severe comminution or prior failed fixation), plan for radial head arthroplasty (monoblock or modular implants).
- Fluoroscopy: Essential for intraoperative assessment of reduction, fixation, and stability through range of motion.
- Arthroscopy Tower: May be considered for diagnostic purposes, lavage, or removal of small loose bodies, particularly in minimally displaced cases.
Patient Positioning
The patient is typically positioned supine on a radiolucent operating table.
*
Arm on a Hand Table:
Allows the elbow to be flexed, extended, and rotated freely, facilitating C-arm access. The hand table should be securely clamped and positioned to allow full visualization of both medial and lateral aspects of the elbow.
*
Tourniquet:
A pneumatic tourniquet on the proximal arm is routinely used for improved visualization and hemostasis.
*
Consideration for Dual Approaches:
Often, both medial and lateral approaches are required. Position the patient to allow easy access to both aspects without repositioning. A sterile preparation and drape should encompass the entire upper extremity from shoulder to hand.
*
Ulnar Nerve Protection:
Pre-operative marking of the ulnar nerve course, especially in revision cases, is prudent.
Detailed Surgical Approach / Technique
The surgical management of complex elbow instability necessitates a systematic and comprehensive approach addressing all components of the injury: osseous fixation, ligamentous repair, and restoration of joint congruity. The order of repair typically follows the "ring concept" of elbow stability, working from inside-out or outside-in as dictated by the injury pattern, but consistently prioritizing stable fixation of the coronoid buttress. In the context of failed bony stabilization, as per the seed content, revision surgery demands even greater precision.
General Principles of Management
- Restore Articular Congruity: Achieve anatomical reduction of all intra-articular fracture fragments, particularly the coronoid and radial head, to minimize post-traumatic arthritis.
- Stabilize Osseous Structures: Provide rigid internal fixation for coronoid, radial head, and olecranon fractures.
- Repair/Reconstruct Collateral Ligaments: Reattach avulsed ligaments or reconstruct severely damaged ones, prioritizing the LUCL and aMCL.
- Ensure Stable, Concentric Reduction: Dynamically assess elbow stability through a full arc of motion under fluoroscopy after all repairs.
Surgical Approaches
Often, a combination of approaches is required.
1. Medial Approach (for Coronoid, MCL, Ulnar Nerve Management)
- Incision: A straight posteromedial or curvilinear incision centered over the medial epicondyle.
- Ulnar Nerve Identification and Protection: The ulnar nerve must be carefully identified, neurolysed, and protected throughout the exposure. Anterior transposition of the ulnar nerve is often recommended, particularly in revision surgery, to prevent iatrogenic injury and allow for a more aggressive repair without tension on the nerve.
- Internervous Plane: The flexor-pronator mass is identified. The interval between the flexor carpi ulnaris (FCU) and the flexor digitorum superficialis (FDS) is utilized. The FCU is retracted posteriorly, and the FDS anteriorly.
- Capsulotomy: The anterior capsule is exposed. A longitudinal incision allows access to the coronoid process.
-
Coronoid Fracture Reduction and Fixation:
This is the most critical step for restoring the anterior buttress.
- Direct Visualization: For larger fragments, direct reduction is ideal. Smaller or highly comminuted fragments, especially anteromedial facets, may be reduced with sutures passed through the fragment and then through drill holes in the ulna (suture lasso technique) or via small K-wires.
-
Fixation Techniques:
- Suture Lasso/Pull-Out Sutures: For smaller coronoid tip fractures or anteromedial facet fractures. High-strength sutures are passed through the fragment, then through drill holes from anterior to posterior in the ulna, and tied over a posterior bone bridge or button.
- Lag Screws: For larger, non-comminuted coronoid fragments, small lag screws (e.g., 2.0 or 2.4 mm) can provide compression and stable fixation.
- Buttress Plate: A small fragment buttress plate (e.g., specifically designed coronoid plate or a 1/3 tubular plate) applied to the anterior face of the ulna can provide excellent stability for larger basal or comminuted fractures. This requires careful dissection to apply the plate anteriorly, ensuring screw length avoids penetration into the posterior cortex or articular surface.
- Anterior Plating: For larger coronoid fragments, anterior plating offers robust fixation.
- Suture Anchors: For avulsion type fractures or reattachment of the sublime tubercle with the MCL.
- Tension Band: Can be used for olecranon fractures, potentially combined with coronoid fixation if part of a trans-olecranon pattern.
- Revision Consideration: In failed fixation, previous hardware is removed. The fracture site is debrided of any fibrous tissue or necrotic bone. Bone grafting (autograft or allograft) may be necessary for non-unions or bone defects. The approach must be adapted to address scar tissue and potentially altered anatomy.
-
MCL Repair/Reconstruction:
If avulsed from the medial epicondyle or sublime tubercle, the MCL anterior bundle is meticulously repaired. Suture anchors are typically used to reattach the ligament to the medial epicondyle. Direct repair of tears can be performed with non-absorbable sutures.
-
Here, an image demonstrating coronoid fixation or a medial approach would be highly relevant.
-
Here, an image demonstrating coronoid fixation or a medial approach would be highly relevant.
2. Lateral Approach (for Radial Head, LCL)
- Incision: A straight lateral incision centered over the lateral epicondyle or a Kocher interval incision.
- Internervous Plane: The Kocher interval between the anconeus (posteriorly, radial nerve innervation) and the extensor carpi ulnaris (ECU) (anteriorly, posterior interosseous nerve innervation) is the preferred approach.
- Protection of Nerves: The posterior cutaneous nerve of the forearm (branch of the radial nerve) should be identified and protected in the subcutaneous layer.
-
Radial Head Fracture Management:
- Internal Fixation: For amenable fracture patterns (e.g., Mason Type II/III), open reduction and internal fixation (ORIF) with low-profile plates and screws is performed. Care is taken to ensure hardware is flush and does not impinge on rotation.
- Radial Head Arthroplasty: For severely comminuted or unsalvageable radial head fractures, or in revision cases with failed fixation, radial head replacement is indicated. This restores radial head length, provides stability, and helps resist valgus and axial loading.
- Excision: Rarely indicated, and generally avoided in the context of complex instability, as it removes a crucial secondary stabilizer and often exacerbates instability.
-
LCL Repair/Reconstruction:
The LUCL is consistently torn in terrible triad injuries and needs repair. It is typically avulsed from the lateral epicondyle. Suture anchors are placed into the isometric point on the lateral epicondyle (slightly posterior and proximal to the center of rotation), and high-strength sutures are used to reattach the avulsed ligament. For chronic instability or highly compromised tissue, reconstruction with a tendon graft may be required.
-
An image demonstrating LCL repair or radial head fixation would fit well here.

-
An image demonstrating LCL repair or radial head fixation would fit well here.
3. Posterior Approach (for Olecranon Fractures)
- Incision: A posterior midline incision, extending proximally and distally as needed.
- Exposure: The triceps aponeurosis is incised, and the olecranon is exposed.
- Fixation: Olecranon fractures are typically fixed with tension band wiring or pre-contoured olecranon plates, achieving anatomical reduction and stable fixation. This approach can be combined with medial or lateral windows for complex fracture-dislocations.
Revision Surgery Considerations (Emphasis from Seed Content)
When bony stabilization has failed, as described in the prompt, revision surgery presents unique challenges:
*
Hardware Removal:
All failed or loose hardware must be removed carefully to avoid further neurovascular damage.
*
Debridement and Bone Grafting:
Non-unions or malunions require debridement of fibrous tissue from the fracture site. Bone grafting is often necessary to fill defects and promote healing, particularly for coronoid non-unions.
*
Soft Tissue Dissection:
Significant scarring from previous surgery makes dissection more challenging. Meticulous identification and protection of neurovascular structures (especially the ulnar nerve) is paramount.
*
Robust Fixation:
The revision implant strategy must provide more robust and biomechanically sound fixation. This may involve larger plates, locking plates, or combined fixation methods (e.g., anterior coronoid plating with supplementary suture lasso).
*
Collateral Ligament Reassessment:
Often, the collateral ligaments have also failed or are attenuated. Reassessment and potentially reconstruction of the LUCL and/or MCL are critical.
*
Spanning External Fixator:
As the seed content mentions, "A spanning external fixator can be considered as a secondary option when adequate fixation and stability cannot be achieved." This is typically a bridging procedure to protect the internal fixation, unload the joint, or provide stability when internal fixation is deemed insufficient or contraindicated (e.g., severe soft tissue compromise, highly comminuted non-reconstructible fractures). It allows for early controlled motion while providing stability, though it "would not address the articular incongruity currently present" directly, necessitating the primary focus on internal reduction and fixation.
Final Assessment of Stability
After all osseous and ligamentous repairs are completed, a rigorous intraoperative assessment of elbow stability is critical:
*
Dynamic Fluoroscopy:
Perform a full range of motion (flexion, extension, pronation, supination) under fluoroscopy.
*
Stress Testing:
Apply gentle varus and valgus stress throughout the range of motion. Assess for any residual gapping, subluxation, or dislocation.
*
Palpation:
Palpate the joint for crepitus or instability.
*
Concentric Reduction:
Confirm concentric reduction of the ulnohumeral and radiohumeral joints. If residual instability persists, further reinforcement (e.g., additional ligament repair, more robust fixation, or external fixator application) must be considered.
*
An image depicting the final fixation or an intraoperative view of stability assessment would be appropriate here.

*
Closure:
Close wounds in layers. A drain may be considered. Apply a sterile dressing and a well-padded posterior splint in a stable position (e.g., 90 degrees flexion, neutral forearm).
Complications & Management
Complex elbow instability injuries and their surgical management are associated with a significant rate of complications. Proactive recognition and appropriate management are crucial for preserving elbow function.
Early Complications
-
Infection:
Superficial (skin) or deep (joint, hardware). Incidence varies but can be up to 5-10% in complex cases.
- Management: Superficial infections may respond to oral antibiotics. Deep infections require surgical debridement, intravenous antibiotics, and potentially hardware removal (if stable union is achieved) or staged reconstruction.
-
Neurovascular Injury:
Most commonly the ulnar nerve due to its superficial course and proximity to the medial epicondyle. Incidence can range from 2-10%.
- Management: Intraoperative recognition and repair. Post-operative neuropathy often requires observation, nerve gliding exercises, and rarely, re-exploration or anterior transposition.
-
Recurrent Instability/Dislocation:
Can occur due to inadequate fixation, missed ligamentous injury, or hardware failure. Incidence can be up to 10-15%.
- Management: Early re-dislocation requires urgent reduction and re-evaluation. May necessitate revision surgery, more robust fixation, or addition of a spanning external fixator.
-
Hardware Failure:
Breakage or loosening of plates/screws.
- Management: Revision surgery with more robust hardware, potentially bone grafting.
Late Complications
-
Stiffness (Loss of Range of Motion):
The most common complication, affecting up to 50% of patients. Often due to heterotopic ossification, capsular contracture, or prolonged immobilization.
- Management: Aggressive physical therapy, dynamic splinting, manipulation under anesthesia, or surgical capsular release (arthroscopic or open) for refractory cases.
-
Heterotopic Ossification (HO):
Ectopic bone formation around the joint, restricting motion. Incidence can be 10-20%, higher in traumatic brain injury or severe trauma.
- Management: Prophylaxis with NSAIDs (e.g., Indomethacin) or low-dose radiation post-operatively. For established HO, surgical excision is performed once the bone is mature (typically 6-12 months post-injury).
-
Post-Traumatic Arthritis:
Common long-term sequela, especially with articular incongruity or significant chondral damage.
- Management: Activity modification, NSAIDs, intra-articular injections. For severe cases, osteotomy, interposition arthroplasty, or total elbow arthroplasty (TEA) may be considered, though TEA is not indicated in younger, active patients as per the seed content ("Total elbow arthroplasty is not indicated due to the patient's age and injury pattern").
-
Non-union/Malunion:
Failure of fracture healing or healing in an unacceptable position.
- Management: Revision surgery with bone grafting, stable fixation, and possibly an external fixator.
-
Chronic Pain:
Can be multifactorial (arthritis, nerve irritation, soft tissue scarring).
- Management: Multimodal pain management, physical therapy, nerve blocks, or surgical intervention for specific causes.
-
Ulnar Nerve Neuropathy:
Chronic irritation or entrapment, sometimes due to scarring or hardware.
- Management: Observation, nerve gliding, or surgical decompression and anterior transposition if symptoms persist or worsen.
Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Elbow Stiffness | 30-50% | Intensive physical therapy, dynamic splinting, manipulation under anesthesia, arthroscopic or open capsular release. |
| Heterotopic Ossification (HO) | 10-20% | Prophylaxis (NSAIDs/radiation). For mature HO, surgical excision. |
| Post-Traumatic Arthritis | 20-30% | Activity modification, NSAIDs, injections. Severe cases: Osteotomy, interposition arthroplasty, Total Elbow Arthroplasty (TEA) for older, low-demand patients (contraindicated in young, active patients due to implant longevity and high stress demands). |
| Recurrent Instability | 5-15% | Revision ORIF of osseous components, ligamentous repair/reconstruction (LUCL, MCL), spanning external fixator, radial head replacement. |
| Surgical Site Infection | 2-10% | Superficial: Oral antibiotics. Deep: Surgical debridement, IV antibiotics, hardware retention/removal depending on stability and timing. |
| Ulnar Nerve Neuropathy | 5-15% | Observation, nerve gliding exercises. Persistent/worsening symptoms: Surgical decompression, anterior transposition. |
| Non-union/Malunion | 5-10% | Revision ORIF, bone grafting (autograft/allograft), more robust internal fixation (e.g., locking plate, external fixator), debridement of fibrous tissue. |
| Hardware Failure | 5-10% | Revision surgery with removal of failed hardware, new or more robust fixation. Addresses underlying biomechanical reasons for failure. If union achieved, elective hardware removal. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical determinant of functional outcome following complex elbow instability surgery. The goal is to achieve a stable, pain-free elbow with a functional range of motion while protecting the surgical repairs. Early, controlled motion is prioritized to prevent stiffness, but balanced against the need to protect healing osseous and ligamentous structures. Protocols must be individualized based on the initial injury severity, the stability achieved intraoperatively, and the patient's response.
General Principles
- Protect Repairs: Initially, the elbow is protected in a hinged brace, restricting motion to a safe arc.
- Early Motion: Controlled passive and active-assisted range of motion (AAROM) exercises begin early to prevent stiffness and improve fluid dynamics.
- Gradual Progression: Increase range of motion and strengthening progressively over several months.
- Patient Education: Emphasize compliance with the protocol and avoidance of contraindicated activities.
- Pain and Edema Control: Essential for patient comfort and participation in therapy.
Phases of Rehabilitation
Phase 1: Acute/Protective Phase (Weeks 0-6)
-
Immobilization:
- Immediately post-op: Well-padded posterior splint in a stable position (e.g., 90 degrees flexion, neutral forearm).
- Days 3-7: Transition to a hinged elbow brace (e.g., dynamic or static-progressive), locked in a safe arc of motion (e.g., 30-90 degrees flexion) as determined by intraoperative stability.
-
Range of Motion (ROM):
- Initiate passive and active-assisted ROM within the prescribed stable arc, often starting with gentle flexion and extension, then gradually introducing supination/pronation.
- Gravity-assisted flexion, supine active extension.
- Avoid stressing the repair (e.g., no forceful passive stretching, no unassisted lifting).
-
Adjunctive Therapies:
- Ice, compression for edema and pain control.
- Scar massage once incision is healed.
- Hand, wrist, and shoulder ROM and strengthening to prevent stiffness in adjacent joints.
- Weight Bearing: Non-weight-bearing for the affected extremity. No lifting, pushing, or pulling.
Phase 2: Intermediate/Strengthening Phase (Weeks 6-12)
- Brace Use: Gradually unlock the hinged brace to increase the ROM as tolerated, eventually discontinuing it around 8-12 weeks if stability is confirmed.
-
ROM Progression:
- Progress to full active ROM in all planes (flexion, extension, pronation, supination).
- Gentle self-stretching and therapist-assisted stretching to regain end-range motion.
-
Strengthening:
- Begin with light isometric strengthening exercises for elbow flexors, extensors, pronators, and supinators.
- Progress to light resistance exercises with elastic bands or very light weights, ensuring no pain or instability.
- Activities of Daily Living (ADLs): Gradually incorporate light functional activities.
- Avoidances: No sudden impacts, forceful pushing/pulling, or ballistic movements.
Phase 3: Advanced/Return to Function Phase (Weeks 12+)
- ROM: Continue to work on achieving full, pain-free ROM.
-
Strengthening:
- Progressive resistance exercises, targeting overall upper extremity strength and endurance.
- Eccentric strengthening as appropriate.
- Proprioceptive exercises.
-
Functional Training:
- Sport-specific or work-specific activities.
- Gradual return to lifting and carrying activities.
-
Return to Activity:
- Return to light work/ADLs usually by 3-4 months.
- Return to heavy labor or contact sports typically requires 4-6 months, sometimes longer, depending on the severity of the initial injury and the progress of rehabilitation.
- Long-Term Follow-up: Regular clinical and radiographic follow-up to monitor for complications such as HO, arthritis, or hardware issues.
Key Considerations
- Heterotopic Ossification Prophylaxis: NSAIDs (e.g., Indomethacin 25mg TID for 3-6 weeks) or low-dose radiation may be administered post-operatively in high-risk patients to minimize HO development.
- Ulnar Nerve Management: Continue nerve gliding exercises if the nerve was involved.
- Individualized Approach: Constant communication between the surgeon, physical therapist, and patient is crucial to adapt the protocol as needed based on individual healing and progress. Overly aggressive rehabilitation can jeopardize repairs, while overly conservative approaches can lead to debilitating stiffness.
Summary of Key Literature / Guidelines
The management of complex elbow instability and coronoid fractures has evolved significantly, driven by a deeper understanding of elbow biomechanics and advances in surgical techniques. Key literature and current guidelines emphasize comprehensive assessment and systematic operative intervention.
- Coronoid Classification and Importance: The work of Regan and Morrey (1989) provided the initial classification of coronoid fractures (Type I-III), highlighting their association with elbow dislocations. O'Driscoll et al. (2001) later refined this, emphasizing the critical role of anteromedial coronoid facet fractures in terrible triad injuries and their distinct contribution to varus posteromedial rotatory instability. Their research underscores that the coronoid is not merely a structural component but a key buttress against posterior translation and a vital attachment for the anterior bundle of the MCL.
- Terrible Triad Paradigm: The seminal work by Hotchkiss (1996) and O'Driscoll et al. (2000) established the "terrible triad" injury as a distinct and highly unstable pattern involving radial head fracture, coronoid fracture, and LUCL rupture. The consensus in literature is that these injuries are almost universally operative, requiring anatomical reduction and stable fixation of all three components.
-
Prioritizing Stabilization:
Current guidelines advocate for a logical sequence of stabilization:
- Coronoid Fixation: This is often the first and most crucial step, as restoring the anterior buttress provides fundamental ulnohumeral stability. Techniques vary, but direct reduction and stable internal fixation (suture lasso, lag screws, or anterior buttress plating) are preferred. The decision to fix a coronoid fracture is not solely based on size but more critically on its impact on stability. Even small, displaced anteromedial facet fractures often require fixation.
- Radial Head Management: Displaced radial head fractures are either fixed (ORIF with low-profile implants) or replaced with an arthroplasty, especially in comminuted or unsalvageable cases. Radial head excision alone is strongly discouraged in complex instability, as it removes a vital secondary stabilizer.
- Ligamentous Repair: Repair of the LUCL is paramount for posterolateral rotatory stability and typically involves reattachment to the lateral epicondyle using suture anchors. The MCL (anterior bundle) repair is performed if valgus instability persists after osseous fixation.
- Early Motion: The principle of early, controlled range of motion (CPM or active-assisted) has become standard of care. This is a delicate balance: sufficient stability must be achieved intraoperatively to permit early motion without jeopardizing repairs. Prolonged immobilization is strongly associated with severe stiffness and poor outcomes.
- Role of External Fixation: A spanning external fixator serves as a valuable secondary option, especially in highly comminuted fractures or cases with persistent instability despite adequate internal fixation. It can protect repairs, allow for early motion, and manage soft tissue injuries. However, as noted in the original content, it does not directly address articular incongruity, which must be managed by internal fixation first.
- Revision Surgery: The literature supports aggressive revision surgery for failed internal fixation or recurrent instability, particularly when the coronoid buttress is compromised. This involves removal of failed hardware, debridement, potential bone grafting, and more robust fixation strategies, often combined with comprehensive collateral ligament reconstruction. Meticulous neurovascular dissection due to scarring is critical.
- Complication Management: Awareness and proactive management of complications, particularly stiffness and heterotopic ossification (with prophylaxis like NSAIDs or radiation), are highlighted across multiple guidelines to optimize long-term function. Total elbow arthroplasty, while an option for severe post-traumatic arthritis, is generally reserved for older, low-demand patients due to the inherent limitations of current implant designs in younger, active individuals.
In summary, the academic discourse consistently emphasizes that successful treatment of complex elbow instability hinges on a systematic, comprehensive surgical approach that meticulously restores osseous anatomy, repairs disrupted ligaments, ensures concentric reduction, and allows for early, controlled rehabilitation. The paramount importance of the coronoid process as a stabilizing buttress is a recurring theme, and its anatomical restoration remains a cornerstone of successful intervention, especially in revision settings where initial stabilization has failed.
Clinical & Radiographic Imaging

You Might Also Like