Comprehensive Guide to Extensile Surgical Fibula Access: Anatomy, Approaches & Indications
Key Takeaway
The 'distal to proximal' approach for fibula surgery is a systematic technique vital for comprehensive access. It prioritizes early anatomical landmark identification, ensuring safe dissection around critical neurovascular structures like the common peroneal nerve. This approach is essential for treating diverse pathologies, from trauma and oncology to reconstructive procedures.
Introduction & Epidemiology
The fibula, though non-weight-bearing in primary axial load transmission, plays a critical role in ankle and knee stability, serving as an attachment point for numerous muscles and ligaments, and contributing significantly to the architecture of the distal tibiofibular syndesmosis. Its slender yet robust structure, coupled with its consistent vascular supply via the peroneal artery, also makes it a valuable source for autogenous bone graft, particularly in vascularized applications. Surgical access to the fibula is thus a fundamental skill for the orthopedic surgeon, enabling the treatment of a wide spectrum of pathologies from trauma to oncological resections and reconstructive procedures.
The approach to the fibula employs a classic extensile exposure, offering access to nearly all parts of the bone. This extensibility allows for tailored interventions, whether a localized cortical window or a near-total fibulectomy. The incidence of fibula pathology requiring surgical intervention is substantial. Fibula fractures, often accompanying tibial shaft fractures or as part of ankle fracture complexes, represent a significant portion of orthopedic trauma. Malignancies, both primary and metastatic, osteomyelitis, and chronic compartment syndromes also necessitate direct fibular access. Furthermore, the role of the fibula as a source of vascularized bone graft has expanded its surgical relevance in the reconstruction of diverse bone defects throughout the body. The "distal to proximal" approach is a systematic technique that prioritizes early identification of key anatomical landmarks and ensures progressive and safe dissection along the fibular shaft, especially important when navigating the varying neurovascular relationships along its course.
Surgical Anatomy & Biomechanics
A thorough understanding of the regional anatomy is paramount for safe and effective fibula exposure.
Osteology
The fibula is a long bone with a distinct head, neck, shaft, and lateral malleolus.
*
Fibular Head:
Articulates with the lateral condyle of the tibia, forming the proximal tibiofibular joint. The common peroneal nerve courses posteroinferiorly to the biceps femoris tendon, wrapping around the fibular neck.
*
Fibular Shaft:
Characterized by three borders (anterior, posterior, interosseous) and three surfaces (lateral, medial, posterior). Its cross-sectional shape changes along its length.
*
Lateral Malleolus:
The distal fibula forms the lateral malleolus, a crucial component of the ankle mortise. It articulates with the talus and forms the distal tibiofibular syndesmosis with the tibia.
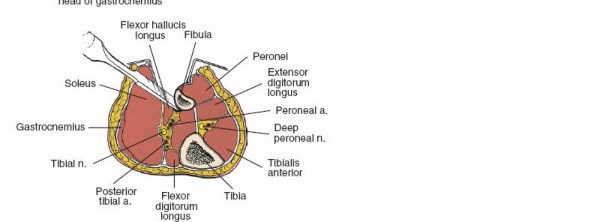
Musculature
The fibula serves as an origin or insertion point for muscles of three of the four leg compartments:
*
Anterior Compartment:
No direct origins from the fibula for the primary anterior compartment muscles (tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius), but the interosseous membrane separates it from the deep posterior compartment.
*
Lateral Compartment:
Contains the peroneus longus and brevis muscles, which originate from the lateral surface of the fibula. They are key landmarks in the posterolateral approach.
*
Deep Posterior Compartment:
Contains the tibialis posterior, flexor hallucis longus (FHL), and flexor digitorum longus. The FHL originates from the posterior surface of the fibula and the interosseous membrane, requiring careful detachment during posterior exposure.
*
Superficial Posterior Compartment:
Contains the gastrocnemius and soleus. The soleus originates in part from the posterior surface of the proximal fibula.
Neurovasculature
Preservation of critical neurovascular structures is non-negotiable.
*
Common Peroneal Nerve:
The most vulnerable nerve during proximal fibula exposure. It lies superficially, crossing the posterior aspect of the fibular neck, then diving deep to divide into the superficial and deep peroneal nerves. Injury can lead to foot drop.
*
Superficial Peroneal Nerve:
Emerges from the lateral compartment distally to become subcutaneous, supplying sensation to the dorsum of the foot (excluding the first web space). It crosses the surgical field anteriorly in the distal leg.
*
Deep Peroneal Nerve:
Travels with the anterior tibial artery in the anterior compartment.
*
Peroneal Artery:
The primary vascular supply to the fibula, running in the deep posterior compartment along the posteromedial aspect of the fibula. It gives off numerous perforating branches that supply the fibular periosteum and cortex. This artery is the pedicle for vascularized fibula grafts.
*
Anterior Tibial Artery:
Located in the anterior compartment, anterior to the interosseous membrane.
*
Posterior Tibial Artery:
Located in the deep posterior compartment, medial to the peroneal artery.
Biomechanics
While the fibula bears only a small percentage of axial load (approximately 6-17%), its contributions to joint stability are crucial:
*
Ankle Stability:
The lateral malleolus forms the lateral wall of the ankle mortise. The distal tibiofibular syndesmosis, composed of the anterior and posterior inferior tibiofibular ligaments, interosseous ligament, and transverse tibiofibular ligament, maintains the integrity of the mortise and prevents talar displacement. Fibular length, rotation, and translation are critical for proper ankle mechanics.
*
Proximal Tibiofibular Joint:
A plane synovial joint providing minor stability to the knee and facilitating rotational movements of the ankle and foot.
Indications & Contraindications
The indications for surgical access to the fibula are diverse, spanning trauma, oncology, infection, and reconstructive surgery.
Indications
-
Partial Resection of the Fibula:
- During tibial osteotomy (e.g., high tibial osteotomy, ankle supramalleolar osteotomy) to facilitate correction of deformity and prevent stress shielding.
- As part of the treatment of tibial nonunion or malunion, to decompress the tibia and promote healing.
- Resection of the Fibula for Decompression: For chronic exertional compartment syndrome, although a fibulectomy for this indication is less common than fasciotomy, it can be considered in specific recalcitrant cases involving the deep posterior compartment or for the rare fibular stress fracture-related compartment syndrome.
- Resection of Tumors: Biopsy or en bloc resection of primary benign or malignant bone tumors (e.g., osteochondroma, osteosarcoma, metastatic lesions) or soft tissue tumors involving the fibula.
- Resection for Osteomyelitis: Debridement and segmental resection of fibular bone infected with acute or chronic osteomyelitis, often followed by reconstruction.
-
Open Reduction and Internal Fixation (ORIF) of Fibula Fractures:
- Isolated fibula shaft fractures that are displaced or comminuted.
- As part of ankle fracture fixation, addressing lateral malleolus fractures and syndesmotic injuries.
- Fractures of the proximal fibula (fibular head/neck) involving the proximal tibiofibular joint or associated with common peroneal nerve injury requiring exploration.
- Complex Pilon fractures, where fibula reconstruction provides indirect reduction of the tibia.
-
Removal of Bone Graft:
- Corticocancellous Strut Grafts: For nonunions, arthrodeses, or to fill bone defects.
- Vascularized Fibula Grafts: Dissected with their vascular pedicles (peroneal artery and venae comitantes) for microsurgical transfer to reconstruct large bone defects in other skeletal sites (e.g., mandible, long bones, spine).
- Arthrodesis: Resection of the distal fibula can be part of an ankle arthrodesis, allowing for preparation of the talar and tibial surfaces and facilitating compression.
Contraindications
Absolute contraindications are few and generally related to the patient's overall health status or local tissue viability.
*
Severe Local Infection:
Active cellulitis or abscess in the operative field mandates delay until infection is controlled.
*
Profound Soft Tissue Compromise:
Extensive open wounds, severe burns, or critical limb ischemia in the proposed surgical area may preclude or significantly complicate the approach.
*
Medical Instability:
Uncontrolled systemic diseases or severe coagulopathy precluding general anesthesia or major surgical intervention.
*
Inadequate Vascularity:
For vascularized fibula graft harvest, compromised peroneal artery flow or significant peripheral vascular disease.
Operative vs. Non-Operative Indications
| Indication Type | Operative Management | Non-Operative Management |
|---|---|---|
| Fractures |
* Displaced or unstable fibula shaft fractures.
Lateral malleolus fractures requiring ORIF (e.g., Danis-Weber B/C, bi/trimalleolar fractures). Fractures with syndesmotic instability. Fractures associated with compartment syndrome. Proximal fibula fractures with common peroneal nerve impingement or proximal tibiofibular joint dislocation. * Pathological fractures due to tumors. |
* Isolated, undisplaced, stable fibula shaft fractures.
Stable lateral malleolus fractures without syndesmotic compromise or significant talar shift (e.g., isolated Danis-Weber A, selected stable B). Stress fractures of the fibula. Minimally displaced avulsion fractures of the lateral malleolus. Select concomitant fibula fractures with stable tibial shaft fractures where fibula fixation is not required for overall limb stability or alignment (e.g., some low-energy spiral fibula fractures). |
| Nonunions/Malunions |
* Symptomatic tibial nonunion requiring fibulectomy.
Fibula nonunion causing pain or instability. Tibial malunion requiring corrective osteotomy with fibulectomy. |
* Asymptomatic fibula nonunion.
* Minimally symptomatic tibial malunion not significantly affecting function. |
| Tumors |
* Biopsy of suspicious fibula lesions.
Excision of benign symptomatic tumors. En bloc resection of malignant tumors (primary or metastatic). |
* Asymptomatic, benign, non-aggressive lesions (e.g., non-ossifying fibroma, fibrous dysplasia) observed with serial imaging.
* Lesions managed by systemic therapy (e.g., multiple myeloma, certain metastatic lesions) where local excision is not indicated. |
| Infection | * Surgical debridement and resection for fibular osteomyelitis (acute or chronic). |
* Early, mild acute osteomyelitis that responds to intravenous antibiotics without significant bone destruction.
* Cellulitis without underlying bone involvement. |
| Decompression | * Fibulectomy for specific, recalcitrant cases of chronic exertional compartment syndrome (less common than fasciotomy). | * Most cases of chronic exertional compartment syndrome, managed by conservative measures (activity modification, physical therapy) or fasciotomy alone. |
| Graft Harvest |
* Harvest of corticocancellous fibula graft for bone defects.
* Harvest of vascularized fibula graft for microvascular reconstruction. |
* Not applicable; this is an elective surgical procedure by definition. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing surgical outcomes and minimizing complications.
Pre-Operative Planning
-
Imaging Review:
- Plain Radiographs: Anteroposterior, lateral, and oblique views of the leg/ankle to assess fracture patterns, bone quality, and any existing hardware. Full-length views are essential for deformity analysis.
- Computed Tomography (CT): Highly valuable for complex fractures, comminution, articular involvement (e.g., pilon fractures), tumor staging, and detailed anatomical assessment for vascularized graft harvest (CT angiography to delineate peroneal artery anatomy). 3D reconstructions can aid in surgical simulation.
- Magnetic Resonance Imaging (MRI): Indicated for soft tissue pathology, tumor staging, osteomyelitis, and nerve evaluation.
- Surgical Strategy: Define the exact extent of fibula exposure required, potential need for hardware (plate and screw systems, external fixators), and strategies for nerve protection. For vascularized grafts, microvascular expertise should be confirmed.
- Patient Specifics: Review comorbidities, medication list (e.g., antiplatelets, anticoagulants), and allergies. Prophylactic antibiotics (e.g., cefazolin) should be administered within 60 minutes prior to incision. Deep vein thrombosis (DVT) prophylaxis should be initiated per institutional protocol.
Patient Positioning
The choice of patient position depends on the extent of fibula access required and whether concurrent approaches to the tibia are planned.
-
Lateral Decubitus Position (Affected side uppermost):
This is the classic and preferred position for a comprehensive posterolateral approach to the fibula.
- The patient is placed on their side with the affected limb uppermost.
- Adequate padding of bony prominences (e.g., contralateral hip, knee, ankle, shoulder, ear) is crucial to prevent pressure sores or nerve palsies. A pillow between the knees can prevent sciatic nerve compression.
- The limb is exsanguinated by elevating it for 3 to 5 minutes, followed by the application of a pneumatic tourniquet as high as possible on the thigh. This provides a bloodless field, enhancing visualization.
- The entire limb, from the hip to the toes, should be prepped and draped to allow for full range of motion of the ankle and knee, and to access the entire length of the fibula.
-
-
Supine Position with Internal Rotation of the Leg:
Alternatively, if this approach is used in conjunction with a surgical approach to the tibia (e.g., anterior approach for pilon fractures, or medial approach for tibial shaft fixation), the patient can be placed supine.
- A sandbag or bump is placed underneath the ipsilateral buttock to internally rotate the leg, presenting the lateral aspect of the fibula.
- Tilting the operating table away from the operative side can further enhance internal rotation and improve exposure of the lateral compartment.
- Care must be taken to ensure stability of the limb and adequate padding.
- For extensive fibula exposure in this position, removal of the sandbag and external rotation of the leg may be required to adequately access the posteromedial aspects of the fibula, particularly for vascularized graft harvest.
- Tourniquet: A pneumatic tourniquet on the proximal thigh is standard. Inflation pressure should be set to supra-systolic levels, typically 100-150 mmHg above systolic blood pressure or a standardized pressure (e.g., 250-300 mmHg), not exceeding 2 hours of inflation time without periodic deflation.
Detailed Surgical Approach / Technique
The "distal to proximal" strategy for fibula access provides a systematic and safe method, particularly useful for extensile exposures and vascularized graft harvest, allowing early identification of the superficial peroneal nerve distally and cautious progression towards the common peroneal nerve proximally.
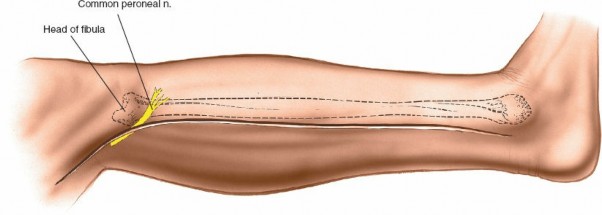
Incision
-
Skin Incision Marking:
The incision is typically longitudinal, centered over the posterolateral border of the fibula.
- For distal access (e.g., lateral malleolus fractures), the incision can start just inferior to the tip of the lateral malleolus and extend proximally along the fibula shaft.
- For extensile exposure, the incision usually originates approximately 1-2 cm posterior to the anterior border of the fibula distally (avoiding the superficial peroneal nerve which typically crosses anteriorly in the distal leg), curving slightly posteriorly in the middle third, and then following the posterior border of the fibula proximally towards the fibular head.
- Care should be taken to avoid placing the incision directly over the prominent fibular crest, which can lead to wound healing issues.
-
(Incision marking)
-
Skin and Subcutaneous Dissection:
- Incise the skin and subcutaneous tissue with a scalpel.
-
(Initial skin incision) - Carefully dissect through the subcutaneous fat. In the distal third of the leg, the superficial peroneal nerve typically emerges from the deep fascia approximately 10-15 cm proximal to the tip of the lateral malleolus, running anteriorly to the fibula. It may be encountered crossing the incision line if positioned too far anteriorly or extended distally. Isolate and retract any visible cutaneous nerves or veins to prevent injury.
-
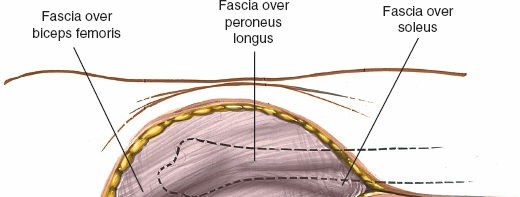(Subcutaneous dissection, identifying fascial layers)
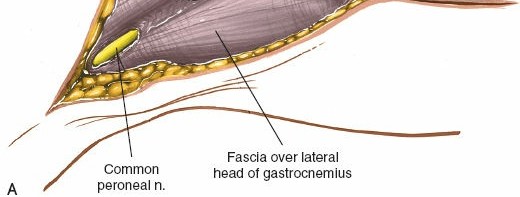
Internervous Plane & Deep Dissection
The posterolateral approach utilizes the interval between the lateral compartment (peroneus longus and brevis) and the superficial posterior compartment (soleus). However, to access the fibula itself, the lateral compartment muscles are retracted, and the deep posterior compartment is entered.
-
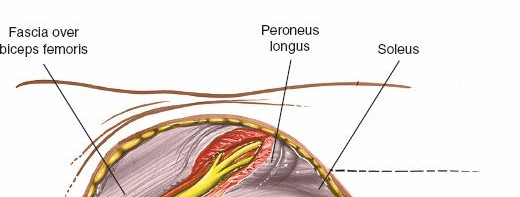
Fascial Incision:
Identify the deep fascia of the leg. Incise the fascia longitudinally along the posterior aspect of the fibula.
-
(Incising fascia over the fibula, exposing the muscle plane)
-
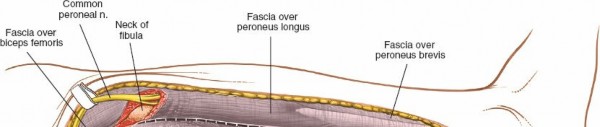
- Exposing the Lateral Compartment: The peroneus longus and brevis muscles become visible. These muscles originate from the lateral surface of the fibula.
-
Mobilization of Peroneals:
Starting distally, elevate the peroneus longus and brevis muscles anteriorly from the lateral surface of the fibula. This is typically performed subperiosteally or just outside the periosteum. Retract these muscles using blunt retractors (e.g., Hohmanns, army-navy). This exposes the lateral surface of the fibula.
-
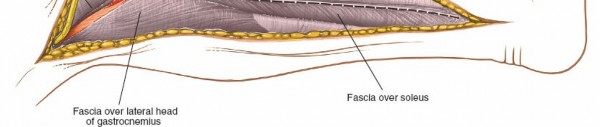
(Elevating peroneals anteriorly, exposing the lateral aspect of the fibula)
-
-
Posterior Fibula Exposure (Deep Posterior Compartment):
- With the lateral compartment retracted anteriorly, identify the soleus muscle, which forms the superficial layer of the posterior compartment. The origin of the soleus from the posterior aspect of the fibula must be detached.
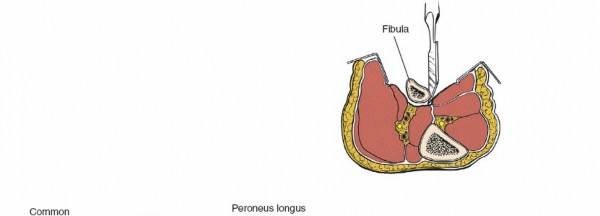
- Deep to the soleus, the flexor hallucis longus (FHL) muscle originates from the posterior surface of the fibula and the interosseous membrane. The FHL is carefully elevated off the fibula.
- This subperiosteal elevation of the FHL must be performed with extreme caution as the peroneal artery and its venae comitantes run immediately deep to the FHL, tightly apposed to the posteromedial surface of the fibula. These vessels are the primary blood supply to the fibula and the pedicle for vascularized grafts.
-
(Retraction to expose posterior aspect, demonstrating soleus origin detachment) - The periosteum is incised longitudinally along the fibula and elevated using periosteal elevators. This provides a clear, bloodless plane for fibular access.
-
(Periosteal stripping or subperiosteal dissection) -
(Exposure of a segment of the fibula) -
(Further proximal dissection, nearing the common peroneal nerve)
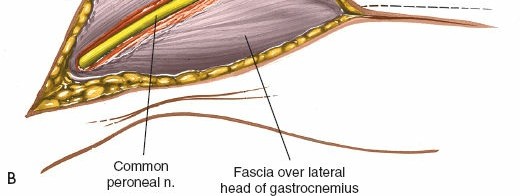
Proximal Extension and Common Peroneal Nerve Protection
As the dissection proceeds proximally, the
common peroneal nerve
becomes the critical structure to protect.
* The nerve curves around the posterior aspect of the fibular neck, running inferior to the biceps femoris tendon insertion.
* In the proximal third of the leg, direct access to the fibula often requires identifying and carefully retracting this nerve. It should be visually identified before any instrument is placed around the fibular neck. Blunt dissection along its course, ensuring it is free from traction or compression, is paramount.
*

(Image showing the common peroneal nerve protection)
Specific Procedures
-
Fracture Fixation:
Once the fracture site is exposed, anatomical reduction is achieved using various clamps, reduction forceps, and temporary Kirschner wires. Plate and screw fixation is then applied according to AO principles, striving for stable fixation.
-
(Specific step for a procedure, e.g., applying a plate)
-
- Fibulectomy (Partial or Segmental): The periosteum is incised circumferentially around the fibula at the desired resection margins. A reciprocating saw or osteotome is used to create clean cuts. The intervening segment is carefully removed, ensuring no injury to surrounding soft tissues, especially the peroneal artery located posteromedially.
-
Vascularized Fibula Graft Harvest:
This procedure requires meticulous dissection.
- After exposing the fibula and detaching the FHL, the peroneal artery and its venae comitantes are identified and isolated.
- Side branches supplying the surrounding muscles are carefully ligated and divided.
- The interosseous membrane is incised along the chosen length of the graft.
- The proximal and distal ends of the fibula segment are osteotomized.
- The graft, with its intact vascular pedicle, is then carefully mobilized and harvested. The length of the pedicle and the integrity of the vessels are paramount for successful microvascular anastomosis.
-
(Demonstrating vascular pedicle for graft harvest)
Closure
- Hemostasis: Ensure meticulous hemostasis of all small bleeding vessels.
- Deep Fascia: The deep fascia can be closed, if possible, without tension, to help restore anatomical planes and reduce dead space. This may not always be feasible or necessary, especially after extensive dissection.
- Subcutaneous Tissue: Close the subcutaneous layer with absorbable sutures to approximate skin edges and reduce tension.
-
Skin Closure:
Close the skin with staples or non-absorbable sutures.
-
(Post-procedure image, wound closure) -
(Final closure/dressing)
-
- Dressing: Apply a sterile dressing. A drain may be considered if significant dead space or bleeding is anticipated.
Complications & Management
Despite meticulous surgical technique, complications can arise, necessitating prompt recognition and appropriate management.
Common Complications and Management
| Complication | Incidence (%) | Salvage Strategies |
|---|---|---|
| Nerve Injury | 1-5% (Common Peroneal) |
*
Prevention:
Meticulous dissection, early identification, and careful retraction of the common peroneal and superficial peroneal nerves.
Intraoperative: If nerve is transected, primary repair or nerve grafting, depending on the defect. Postoperative: Observe for signs of recovery. If no recovery by 3-6 months, consider nerve exploration and neurolysis, repair, or transfer (e.g., anterior tibial tendon transfer for foot drop). Foot drop brace for supportive care. |
| Vascular Injury | <1% (Major vessels) |
*
Prevention:
Careful subperiosteal dissection, particularly along the posteromedial aspect of the fibula to protect the peroneal artery.
Intraoperative: Direct repair of the vessel with microsurgical technique. Ligation of smaller branches. If major vessel injury is not amenable to repair, consider vascular consultation for bypass grafting. For vascularized fibula grafts, monitor graft viability closely. Postoperative: Vigilant monitoring for signs of ischemia (pallor, pulselessness, paresthesias, pain, paralysis, poikilothermia). Doppler assessment. |
| Infection | 1-5% |
*
Prevention:
Strict aseptic technique, prophylactic antibiotics, meticulous hemostasis.
Management: * Superficial: Oral antibiotics, local wound care. * Deep/Osteomyelitis: * Surgical debridement, irrigation, cultures, targeted intravenous antibiotics, removal of hardware if infected and stable bone (or staged removal/re-fixation). Negative pressure wound therapy, muscle flaps, or free tissue transfer may be required for chronic defects. |
| Nonunion/Malunion | 5-15% (Fracture) |
*
Prevention:
Stable internal fixation, anatomical reduction, adequate vascularity.
Management: * Nonunion: Revision surgery with debridement, stable internal fixation (e.g., larger plate, compression, lengthening), bone grafting (autograft or allograft), biological augmentation (e.g., bone morphogenetic proteins), or electrical stimulation. * Malunion: * Corrective osteotomy and fixation, often with associated soft tissue releases. |
| Wound Complications | 5-10% |
*
Prevention:
Atraumatic tissue handling, careful skin incision placement (avoiding tension), meticulous closure, avoiding hematoma formation.
Management: * Hematoma: Evacuation. * Dehiscence: Local wound care, secondary closure, or skin grafting/flap coverage for larger defects. * Necrosis: * Debridement of necrotic tissue, local wound care, possible plastic surgery consultation for reconstruction. |
| Compartment Syndrome | Rare (Iatrogenic) |
*
Prevention:
Minimizing tissue trauma, careful hemostasis, avoiding prolonged tourniquet time (especially if combined with other approaches).
Management: * Emergent fasciotomy of all four compartments to relieve pressure. |
| Ankle Instability | Variable |
*
Prevention:
For fibulectomy, careful assessment of stability and consideration of reconstruction (e.g., fusion) if significant segment resected.
Management: * Physical therapy to strengthen surrounding musculature. Ankle bracing or orthotics. Surgical stabilization (e.g., ligament reconstruction, arthrodesis) if persistent instability causes pain and functional impairment after significant fibulectomy, especially if the distal syndesmosis or lateral malleolus is compromised. |
| Donor Site Morbidity | Variable |
*
Prevention (for graft harvest):
Careful patient selection, pre-operative vascular assessment.
Management: * Pain control, physiotherapy for muscle weakness, managing minor wound complications. Rarely, nerve injury (e.g., superficial peroneal nerve neuroma) may require local injection or excision. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for achieving optimal functional recovery and preventing secondary complications. Protocols vary significantly based on the specific indication, extent of intervention, and patient factors.
Immediate Post-Operative Phase (Days 0-14)
- Pain Management: Implement a multimodal analgesia strategy (e.g., NSAIDs, acetaminophen, opioids, regional blocks) to minimize pain and facilitate early mobilization.
- Wound Care: Monitor incision for signs of infection, hematoma, or dehiscence. Maintain a clean, dry, sterile dressing. Staple/suture removal typically at 2-3 weeks.
-
Immobilization:
- Fracture Fixation: Often involves a bulky soft dressing, posterior splint, or short leg cast to provide initial comfort and protection.
- Fibulectomy/Graft Harvest: Similar immobilization for soft tissue protection.
-
Weight Bearing (WB):
- Fractures (unstable): Non-weight bearing (NWB) or touch-down weight bearing (TDWB) with crutches or a walker.
- Stable Fractures/Fibulectomy: May progress to protected weight bearing (PWB) in a boot or brace as tolerated, based on surgeon preference and intraoperative stability.
- Elevation: Keep the operative limb elevated above heart level to minimize swelling.
-
Early Motion:
- For fracture fixation, if stable, early ankle range of motion (ROM) may be initiated.
- For vascularized fibula grafts, strict NWB and elevation are maintained, with vigilance for graft viability.
Subacute Phase (Weeks 2-6)
- Immobilization/Protection: Transition from cast to a removable CAM walker boot or functional brace, allowing for hygiene and controlled ROM.
-
Weight Bearing:
Gradual progression of weight bearing based on radiographic healing, pain levels, and surgical stability.
- Fractures: Often progresses to PWB, then FWB over 4-8 weeks.
- Fibulectomy/Graft Harvest: May have longer NWB periods (6-12 weeks) to allow for soft tissue healing and, for grafts, revascularization and incorporation.
-
Physical Therapy:
- Range of Motion: Gentle active and passive ankle ROM exercises (dorsiflexion, plantarflexion, inversion, eversion).
- Strengthening: Isometrics of ankle musculature.
- Edema Control: Compression stockings, elevation.
Remodeling & Strengthening Phase (Weeks 6-12+)
- Weight Bearing: Progression to full weight bearing as tolerated, typically out of the boot/brace for most activities.
-
Physical Therapy:
- Advanced Strengthening: Concentric and eccentric strengthening of all ankle muscle groups (resistance bands, calf raises, toe raises).
- Proprioception and Balance: Single-leg stance, wobble board, balance exercises.
- Gait Training: Address any compensatory gait patterns.
- Scar Mobilization: To prevent adhesions and improve soft tissue pliability.
- Functional Progression: Gradual return to activities of daily living. Low-impact activities are introduced before high-impact.
Return to Activity Phase (Months 3-6+)
- Continued Strengthening & Conditioning: Sport-specific training, agility drills.
- Impact Loading: Gradually introduce running, jumping, and cutting activities.
- Monitoring: Continue to monitor for pain, swelling, and functional limitations. Radiographic assessment of bone healing.
- Specific considerations for vascularized fibula grafts: Longer periods of protection and slower progression are typical due to the need for graft integration and remodeling. Monitoring for hypertrophy of the graft may be required.
Summary of Key Literature / Guidelines
The surgical approach to the fibula is deeply rooted in anatomical principles established by foundational texts and surgical atlases.
- Classic Surgical Anatomy: Works by Henry (1957) and Hoppenfeld and deBoer (1984) provided definitive descriptions of surgical approaches to the lower extremity, including the posterolateral fibular approach, delineating critical internervous planes and neurovascular structures. These references remain indispensable for understanding the anatomical basis of the technique.
- AO Principles of Fracture Management: The Arbeitsgemeinschaft für Osteosynthesefragen (AO Foundation) has extensively detailed principles for internal fixation of fibula fractures, particularly in the context of ankle and pilon fractures. Their guidelines emphasize anatomical reduction, stable fixation, and preservation of soft tissues, which are integral to successful outcomes. Specific plate designs (e.g., 1/3 tubular, reconstruction, locking plates) and their indications are well-defined.
- Vascularized Fibula Graft (VFG) Literature: Research by Taylor (1975) and subsequent microvascular surgeons established the reliability of the VFG as a reconstructive option. The anatomical basis of the peroneal artery and its perforators has been thoroughly studied, defining the utility of the VFG in various oncological, traumatic, and congenital bone defects. Studies by Chang (1989) and Wei et al. (1999) further refined VFG harvest techniques and expanded its applications, reporting high success rates for graft viability and functional outcomes, albeit with specific donor site morbidity considerations.
- Compartment Syndrome Management: While fibulectomy for compartment syndrome is less common than fasciotomy, the literature on chronic exertional compartment syndrome (CECS) and acute compartment syndrome (ACS) provides a framework for understanding indications and alternative decompression strategies. Reviews by Styf (1989) and Frassica and O'Keefe (2000) offer comprehensive overviews of these conditions.
- Outcomes of Fibula Fracture Fixation: Numerous clinical studies and systematic reviews have evaluated the outcomes of ORIF for fibula fractures, particularly in the context of ankle instability. These studies consistently demonstrate that anatomical reduction and stable fixation are paramount for restoring ankle kinematics and preventing post-traumatic arthritis.
- Future Directions: Ongoing research focuses on optimizing patient-specific implants using 3D printing, advanced imaging techniques for pre-operative planning (e.g., high-resolution CT angiography for VFG harvest), and enhancing rehabilitation protocols to accelerate functional recovery while minimizing complications. The role of biological augmentation (e.g., PRP, stem cells) in fibula fracture healing and graft incorporation also remains an active area of investigation.
Clinical & Radiographic Imaging