Colles Fractures: Epidemiology, Surgical Anatomy, and Biomechanics
Key Takeaway
A Colles fracture is a prevalent distal radius fracture, typically occurring within 2.5 cm of the articular surface, often presenting with a characteristic "dinner fork" deformity. It commonly results from a fall on an outstretched hand (FOOSH), particularly affecting osteoporotic elderly women. Understanding its epidemiology, surgical anatomy, and biomechanics, including radial length, inclination, and volar tilt, is crucial for accurate diagnosis and effective management.
Introduction & Epidemiology
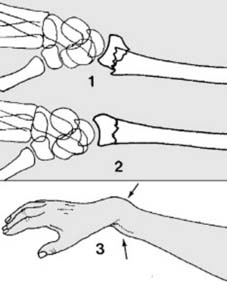
Colles fractures represent a significant and prevalent injury within orthopedic trauma, characterized by a fracture of the distal radius typically occurring within 2.5 cm of the articular surface. As elucidated in the foundational understanding, it is the most common fracture encountered in clinical practice, often presenting with a characteristic "dinner fork" deformity when displaced. The injury primarily affects middle-aged and elderly women, with osteoporosis being a significant contributing factor to both incidence and fracture morphology. The typical mechanism involves a fall on an outstretched hand (FOOSH) with the wrist in extension and pronation, driving the distal radial fragment dorsally and radially.
This seminal observation underscores the critical biomechanical forces at play.

Epidemiologically, distal radial fractures account for approximately one-sixth of all fractures seen in emergency departments. The bimodal distribution reflects distinct patient populations: younger individuals often sustain high-energy trauma, while older adults, particularly postmenopausal women, are susceptible to low-energy falls due to diminished bone mineral density. The latter group's susceptibility is intrinsically linked to age-related osteopenia and osteoporosis, altering the bone's structural integrity and increasing the propensity for fracture. The characteristic displacement patterns associated with Colles fractures are central to both diagnosis and treatment planning.
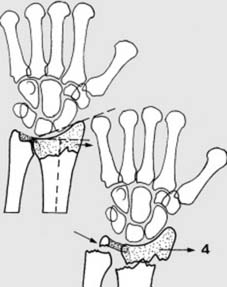
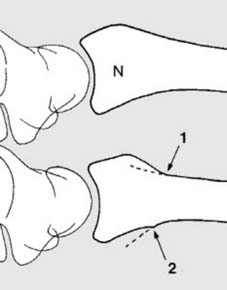
The six characteristic features of a displaced Colles fracture include:
* Dorsal displacement of the distal fragment.
* Radial displacement of the distal fragment.
* Dorsal angulation of the distal fragment.
* Radial angulation (apex ulnar) of the distal fragment.
* Shortening of the radius.
* Supination of the distal fragment (less consistently observed, often due to pronator quadratus integrity).
These displacements, often resulting from a dorsally directed force (F) and the inherent obliquity of impact, lead to the classic deformity.
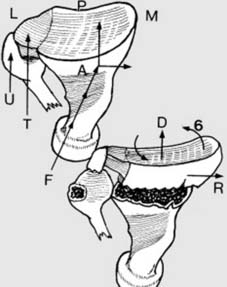
The triangular fibrocartilage complex (TFC) and ulnar styloid (U) are critical components of the distal radioulnar joint (DRUJ), which can be intimately involved in these fracture patterns. Understanding these deformities is paramount for accurate reduction and restoration of normal wrist kinematics.

While the classic Colles fracture typically spares the radiocarpal joint itself (distal fragment remains intact), a multitude of associated injuries can complicate these presentations, including DRUJ instability, ulnar styloid fractures, and various carpal ligamentous injuries. A thorough understanding of the specific fracture pattern and associated soft tissue compromise is crucial for optimal patient management and prevention of long-term sequelae such as malunion, nonunion, and degenerative arthrosis.
Surgical Anatomy & Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the distal radius and wrist complex is indispensable for the effective management of Colles fractures. The distal radius is a complex anatomical structure comprising the articular surfaces (scaphoid and lunate fossae), metaphysis, and diaphysis. Key anatomical landmarks and angles critical for restoration include:
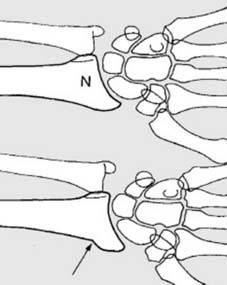
- Radial Length: The distance between the radial styloid and the ulnar head, typically 11-12 mm. Loss of radial length leads to positive ulnar variance, increasing load on the ulnar side of the wrist and potentially predisposing to ulnocarpal impingement or DRUJ pathology.
- Radial Inclination (Radial Angle): The angle formed by a line connecting the tips of the radial styloid and the ulnar aspect of the lunate fossa, and a line perpendicular to the long axis of the radius. Normal inclination is 22-23 degrees. Decreased radial inclination can lead to carpal instability and altered load transmission.
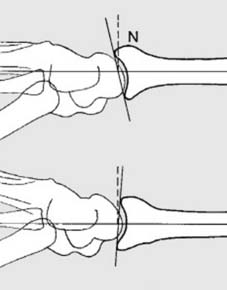
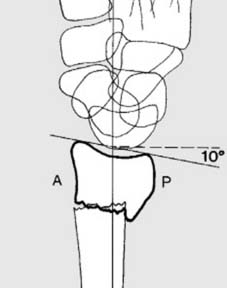
- Volar Tilt (Palmar Tilt): The angle between the articular surface of the distal radius and a line perpendicular to the long axis of the radius in the sagittal plane. Normal volar tilt is 11-12 degrees. Loss of volar tilt, leading to dorsal tilt, is a hallmark of Colles fracture and significantly impairs wrist function.
- Distal Radioulnar Joint (DRUJ): This complex synovial joint, composed of the sigmoid notch of the radius and the ulnar head, is stabilized by the triangular fibrocartilage complex (TFCC), which includes the dorsal and volar radioulnar ligaments. DRUJ stability is paramount for forearm rotation (pronation/supination). Fractures involving the distal radius often disrupt the DRUJ directly or indirectly, leading to instability or incongruity. Ulnar styloid fractures, common in Colles fractures, can indicate TFCC injury and potential DRUJ instability.
The intrinsic stability of the wrist is maintained by a complex interplay of bony architecture, static ligamentous restraints (intrinsic and extrinsic carpal ligaments, radioulnar ligaments), and dynamic muscle stabilizers (e.g., pronator quadratus). A FOOSH injury with the wrist in dorsiflexion concentrates axial load on the distal radius. The exact fracture pattern is influenced by the degree of wrist extension, pronation/supination at impact, bone quality, and the magnitude and vector of the applied force. The classic Colles fracture exhibits dorsal and radial displacement due to the leverage provided by the carpus and the deforming forces of the brachioradialis, extensor carpi radialis longus and brevis, and supinator muscles. The pronator quadratus, if intact, can sometimes prevent severe supination of the distal fragment but its integrity is often compromised in highly displaced fractures.
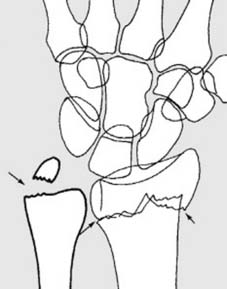
Understanding the specific fragments and their displacement relative to these anatomical parameters is critical for reduction. For instance, restoration of radial length and volar tilt is crucial for minimizing the risk of malunion and subsequent functional impairment. The integrity of the radial styloid and its articulation with the scaphoid, along with the lunate fossa's articulation with the lunate, dictate joint congruity and future arthritic risk. Disruption of these surfaces, particularly an intra-articular step-off or gap, can accelerate degenerative changes. The extent of comminution, both dorsal and volar, significantly impacts fracture stability and dictates the chosen fixation method.
The anatomy of the distal radius articular surface is complex, including the scaphoid and lunate fossae.
Variations in the fracture pattern can involve the distal articular surface.
Indications & Contraindications
The management of Colles fractures involves a judicious assessment of fracture characteristics, patient factors, and functional demands to determine whether operative or non-operative treatment is indicated. Initial assessment involves clinical examination for deformity, neurovascular status, and soft tissue integrity, complemented by orthogonal plain radiographs (PA, lateral, and oblique views) of the wrist to evaluate the fracture pattern, displacement, and articular involvement. Computed tomography (CT) scans may be indicated for complex intra-articular fractures, significant comminution, or when assessing DRUJ involvement, providing greater detail for pre-operative planning.
Initial radiographic assessment is fundamental.

Further imaging may be required to fully characterize the injury.
Non-Operative Indications
Non-operative management, typically involving closed reduction and cast immobilization, is generally reserved for stable, extra-articular or minimally displaced intra-articular fractures that can be adequately reduced and maintained.
Acceptable Reduction Parameters for Non-Operative Management:
*
Radial Length:
< 2-3 mm of shortening (relative to the uninjured side).
*
Radial Inclination:
< 5 degrees loss of normal inclination (i.e., maintaining > 15-18 degrees).
*
Volar Tilt:
Neutral to slight dorsal tilt (< 5-10 degrees dorsal angulation). While restoration of volar tilt is ideal, slight dorsal angulation may be acceptable in older, low-demand patients.
*
Intra-articular Step-off/Gap:
< 1-2 mm, if intra-articular.
*
DRUJ Congruity:
Stable and congruent.
Fractures failing to meet these criteria after closed reduction or demonstrating secondary displacement within the cast are considered unstable and typically require surgical intervention.
Operative Indications
Surgical management is indicated for unstable fractures that cannot be adequately reduced or maintained non-operatively, or for specific fracture patterns known to have poor outcomes with non-operative treatment.
Absolute Operative Indications:
*
Open fractures:
Require urgent debridement and stabilization to prevent infection.
*
Irreducible fractures:
Failure to achieve or maintain acceptable alignment after closed reduction attempts.
*
Neurovascular compromise:
Acute carpal tunnel syndrome or other neurovascular injury requiring decompression and fixation.
*
Compartment syndrome:
Rare but possible, requiring emergent fasciotomy and stabilization.
Relative Operative Indications (Unstable Fractures):
*
Intra-articular step-off/gap > 2 mm:
Associated with increased risk of post-traumatic arthritis.
*
Loss of radial length > 3 mm.
*
Dorsal angulation > 10 degrees
(some literature suggests > 0 degrees dorsal angulation relative to ipsilateral ulna or comparison to contralateral side as an indication).
*
Loss of radial inclination > 5 degrees
(i.e., < 15-18 degrees).
*
Significant comminution:
Especially of the dorsal or volar cortices, suggesting instability.
*
DRUJ instability or incongruity:
Particularly if associated with a displaced ulnar styloid fracture or TFCC tear.
*
Younger, high-demand patients:
Stricter criteria for anatomical reduction to optimize long-term function.
*
Elderly patients with good physiological reserve and functional demands:
Age alone is not a contraindication to surgery if functional goals warrant it.
Contraindications
-
Absolute Contraindications:
- Severe medical comorbidities precluding safe anesthesia and surgery (e.g., uncontrolled cardiac disease, severe coagulopathy).
- Acute infection at the surgical site.
- Non-viable limb.
-
Relative Contraindications:
- Poor soft tissue envelope.
- Extremely comminuted bone, offering poor purchase for fixation (may necessitate external fixation or non-operative approach in select cases).
- Patient non-compliance with post-operative protocols.
Operative vs. Non-Operative Indications
| Feature / Parameter | Non-Operative Management (Closed Reduction & Immobilization) | Operative Management (ORIF, External Fixation, Percutaneous Pinning) |
|---|---|---|
| Fracture Type | Stable, extra-articular or minimally displaced intra-articular fractures (e.g., AO 23-A2, Frykman Type I, II) | Unstable fractures; significantly displaced intra-articular fractures (e.g., AO 23-C, Frykman Type III-VIII); highly comminuted fractures (AO 23-A3, B3); open fractures; fractures with neurovascular compromise; irreducible fractures. |
| Radial Length | < 2-3 mm shortening | > 3 mm shortening |
| Radial Inclination | Maintained > 15-18 degrees | Loss > 5 degrees (i.e., < 15-18 degrees) |
| Volar Tilt | Neutral to slight dorsal tilt (< 5-10 degrees dorsal angulation) | Dorsal angulation > 10 degrees (some advocate > 0 degrees) |
| Intra-articular Step/Gap | < 1-2 mm | > 2 mm |
| DRUJ Stability | Stable | Unstable or incongruent |
| Comminution | Minimal to none | Significant dorsal or volar comminution |
| Soft Tissue | Intact, no open wounds | Open fracture, severe soft tissue compromise (consider external fixation) |
| Patient Factors | Low functional demand, poor surgical candidate due to comorbidities, compliant with cast care, reliable for follow-up | High functional demand, physiologically fit, younger patients, non-compliant with cast care or risk of secondary displacement in cast. |
| Secondary Displacement | Fracture maintains reduction within cast | Secondary displacement after initial closed reduction and immobilization |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful surgical outcomes for Colles fractures. This process begins with a comprehensive review of clinical findings and imaging studies.
Imaging Review
Beyond standard PA, lateral, and oblique radiographs, a contralateral wrist series is often useful for comparison, especially in assessing radial length, inclination, and volar tilt. A CT scan is invaluable for:
* Characterizing intra-articular extension and step-offs/gaps.
* Assessing comminution, particularly in the articular and metaphyseal regions (e.g., dorsal or volar impaction).
* Evaluating DRUJ congruity and the presence of associated ulnar styloid fractures or TFCC avulsions.
* Identifying subtle carpal injuries.
Planning should include consideration of specific hardware needs based on fracture pattern and bone quality, including plate size, screw length, and potential need for bone graft or substitutes if significant metaphyseal defects are present.
Anesthesia
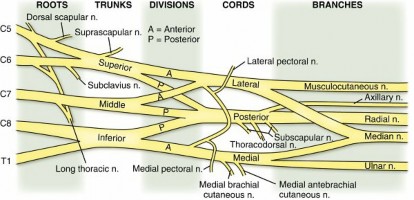
Regional anesthesia (e.g., interscalene or supraclavicular block) combined with monitored anesthesia care (MAC) or general anesthesia is commonly employed. Regional blocks offer excellent post-operative pain control and muscle relaxation, facilitating reduction.
Patient Positioning
The patient is typically positioned supine on the operating table. The affected arm is prepped and draped to allow access to the forearm, wrist, and hand.
*
Arm Table:
A specialized arm table is usually utilized to support the extremity.
*
Tourniquet:
A pneumatic tourniquet is applied to the upper arm to provide a bloodless field, which is crucial for detailed dissection and visualization of fracture fragments.
*
Finger Traps:
For reduction, particularly for external fixation or percutaneous pinning, the hand is suspended using finger traps with approximately 10-15 pounds of longitudinal traction. The elbow is flexed 90 degrees and positioned over the arm table. This setup helps to ligamentotaxis, gradually restoring radial length and anatomical alignment.
Proper positioning is critical for surgical access and reduction.

Traction can be applied to facilitate reduction prior to definitive fixation.

Fluoroscopy is indispensable throughout the procedure for confirming reduction and hardware placement. A C-arm is positioned to allow orthogonal views (PA and lateral) of the wrist without repositioning the limb. Pre-operative fluoroscopy images or plain radiographs help plan the intra-operative sequence.

Detailed Surgical Approach / Technique
The primary goal of surgical management is anatomical reduction of the articular surface and restoration of radial length, radial inclination, and volar tilt, followed by stable internal fixation to permit early mobilization.
Reduction Maneuvers
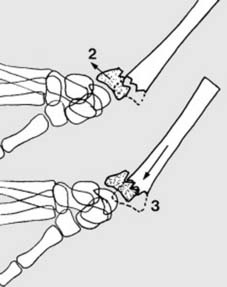
Regardless of the chosen fixation method, a satisfactory reduction is paramount. This often begins with manual traction to disimpact the fracture fragments. The classic reduction maneuver for a Colles fracture involves:
1.
Exaggerated Deformity:
Hyperdorsiflexion of the wrist to disengage impacted fragments.
2.
Traction:
Application of longitudinal traction along the axis of the forearm. This can be aided by finger traps or by direct manual traction.
3.
Correction of Displacement:
The surgeon then applies a volar and ulnar directed force to the distal fragment while counter-traction is applied to the elbow. This corrects dorsal and radial displacement, and restores radial length.
4.
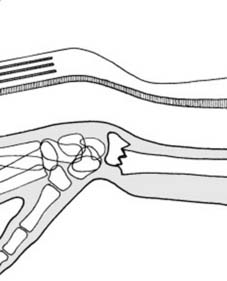
Palmarflexion and Ulnar Deviation:
The wrist is then pronated and gently brought into palmarflexion and ulnar deviation to maintain the reduction.
This maneuver addresses the classic dorsal and radial displacement, aiming to restore volar tilt and radial length.
For significantly comminuted fractures or those with articular depression, ligamentotaxis via external fixation or limited open reduction techniques may be necessary.
Fixation Options
1. Volar Locking Plate Fixation (VLP)
This is the current gold standard for unstable distal radial fractures, offering robust fixation and allowing for early range of motion.
-
Surgical Approach (Modified Henry's Approach):
- Incision: A longitudinal incision, typically 4-6 cm, is made on the volar aspect of the distal forearm, centered between the flexor carpi radialis (FCR) tendon and the radial artery. This typically begins approximately 1 cm proximal to the wrist crease and extends proximally.
- Dissection: The incision is carried through the skin and subcutaneous tissue. The superficial radial nerve branches should be identified and protected, although they are typically radial to the incision. The palmaris longus tendon (if present) and FCR tendon are identified.
- Internervous Plane: The interval between the FCR tendon (medial) and the radial artery/flexor pollicis longus (FPL) tendon (lateral) is developed. The FCR tendon is retracted ulnarly. The radial artery, lying lateral to the FCR sheath, is carefully retracted radially with the FPL.
- Pronator Quadratus Exposure: The pronator quadratus muscle lies directly on the volar aspect of the distal radius. The fascia overlying the pronator quadratus is incised.
-
Pronator Quadratus Release:
The pronator quadratus is subperiosteally elevated off the volar aspect of the distal radius, typically from its radial to its ulnar insertion, exposing the fracture site. Care must be taken to elevate the muscle as one unit to allow for later repair, which helps to cover the plate and may prevent flexor tendon irritation.
The surgical exposure for volar plating through the modified Henry's approach is critical.
-
Fracture Reduction:
- Once exposed, direct visualization assists in reduction. K-wires or bone clamps can be used to manipulate fragments.
- For articular step-offs, a bone tamp or small osteotome can be used to elevate depressed fragments from the dorsal side (via a separate small dorsal incision if needed) or directly from the volar side, often supported by temporary K-wires.
- Restoration of radial length, inclination, and volar tilt is confirmed with fluoroscopy.
-
Plate Application:
- The volar locking plate is positioned on the volar aspect of the distal radius. The distal end of the plate is placed proximal to the watershed line to minimize flexor tendon irritation.
- Plate Selection: Plates come in various designs (e.g., standard, extra-articular, variable angle locking). The choice depends on the fracture pattern and surgeon preference.
- Proximal Fixation: At least two cortical screws are placed proximally into the radial shaft to secure the plate.
-
Distal Locking Screws:
Multiple locking screws (typically 4-7) are directed into the distal fragment. These screws are designed to provide subchondral support, particularly for the scaphoid and lunate fossae. Variable angle locking screws allow for greater flexibility in targeting specific fragments. It is crucial to ensure screws do not penetrate the dorsal cortex or articular surface. Fluoroscopy in multiple planes (PA, lateral, 45-degree pronation/supination) is used to confirm screw length and position.
A well-applied volar locking plate provides stable fixation.

Post-fixation imaging confirms the reduction and hardware placement.
- Closure: The pronator quadratus is repaired over the plate. The subcutaneous tissues and skin are closed in layers.
2. External Fixation
External fixation is primarily used for highly comminuted, unstable fractures, open fractures, or in cases of severe soft tissue compromise, acting primarily by ligamentotaxis. It can also be used as a temporizing measure or as an adjunct to limited internal fixation (e.g., K-wires).
- Technique: Pins are typically placed in the radial shaft (proximal fragment) and the base of the second metacarpal (distal fragment) or, less commonly, the index finger proximal phalanx.
- Reduction: Longitudinal traction is applied via the external fixator to restore radial length and disimpact fragments. Manual manipulation and K-wires can aid in reduction and stabilize individual fragments (pin-fixation).
-
Frame Application:
The external fixator frame is then applied and locked to maintain reduction.
External fixation provides stability, especially in complex cases.
This is an example of an external fixator application.
3. Percutaneous Pinning
Used for relatively stable, extra-articular or minimally displaced intra-articular fractures that can be reduced closed but require additional stability beyond casting.
- Technique: After closed reduction, K-wires are inserted percutaneously through the radial styloid into the radial shaft, or from the dorsal-ulnar aspect of the radius across the fracture site to prevent dorsal displacement. Various pinning configurations exist (e.g., Kapandji, multiple divergent pins). Fluoroscopy is essential to guide pin placement and avoid neurovascular structures.
4. Dorsal Plating
Less common due to the risk of extensor tendon irritation and rupture. Reserved for specific indications, such as large dorsal comminution or irreducible dorsal fragments not amenable to volar plating.
- Approach: A dorsal longitudinal incision is made, and the extensor compartments are identified and retracted. The fracture is reduced, and a low-profile dorsal plate is applied. Great care is taken to ensure adequate soft tissue coverage of the plate.
Associated Injuries
- DRUJ Instability: Assessed intra-operatively after radial fixation. If unstable, the TFCC may require repair, or the DRUJ may need temporary K-wire stabilization in supination (for dorsal instability) or pronation (for volar instability).
- Ulnar Styloid Fractures: If significantly displaced at the base or associated with DRUJ instability, fixation may be considered (tension band wiring, screw fixation).
- Carpal Ligament Injuries: Suspected in cases of persistent carpal malalignment despite radial reduction. Requires further investigation (e.g., arthroscopy) and possible repair.
A comprehensive intraoperative evaluation is important, including assessing the DRUJ.
Complications & Management
Despite meticulous surgical technique, complications following Colles fracture management can occur, ranging from minor annoyances to debilitating sequelae. Proactive identification and appropriate management are crucial for optimizing patient outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence (Approximate) | Etiology | Salvage Strategy Colles fracture is one of the most common fractures that we manage in orthopedics, especially in the elderly female population. Its distinct patterns of displacement necessitate specific surgical approaches to ensure optimal functional recovery and minimize long-term complications.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for restoring function and preventing complications following surgical fixation of Colles fractures. Protocols are typically individualized based on fracture stability, method of fixation, bone quality, and patient comorbidities, but generally follow an accelerated course with stable internal fixation.
Phase 1: Immobilization & Early Motion (Weeks 0-2/3)
- Goal: Protect fracture fixation, minimize swelling, initiate early pain-free range of motion (ROM) to adjacent joints, and prevent stiffness.
- Immobilization: A removable wrist splint (volar or sugar-tong) is often used for comfort and protection, especially when not performing exercises. The splint is usually worn full-time, only removed for exercises and hygiene. For less stable fixation or when external fixators are used, continuous splinting or casting may be required for a longer duration.
-
Exercises:
- Finger ROM: Active flexion and extension of all fingers and thumb (hook fist, full fist, straight fist, table top). These are crucial to prevent digital stiffness and maintain tenodesis effect.
- Elbow ROM: Active flexion and extension.
- Shoulder ROM: Active elevation, rotation, and abduction to prevent "frozen shoulder."
- Wrist ROM (Passive/Assisted): For stable volar locking plate fixation, gentle passive and active-assisted wrist flexion/extension, radial/ulnar deviation, and forearm pronation/supination may begin as early as 1-2 weeks post-operatively, within pain-free limits. This is typically initiated under the guidance of a hand therapist. The goal is to avoid forceful movements that could compromise fixation.
- Edema Management: Elevation, gentle massage, and compression garments (e.g., tubigrip) are encouraged.
- Pain Management: As prescribed, aiming for functional pain levels to allow participation in therapy.
Phase 2: Progressive ROM & Strengthening (Weeks 3-6/8)
- Goal: Achieve full, pain-free wrist and forearm ROM, restore grip strength, and improve fine motor skills.
- Discontinuation of Splint: Once sufficient fracture healing is evident radiographically and clinically stable, the protective splint is gradually discontinued, typically by 4-6 weeks for volar locking plates. For external fixators, pins are usually removed between 6-8 weeks, followed by a period of splinting and then progressive motion.
- Active & Passive Wrist ROM: Intensify efforts to regain full wrist flexion, extension, pronation, supination, and radial/ulnar deviation. Gentle sustained stretches are introduced.
-
Strengthening:
- Isometric exercises: For wrist flexors, extensors, pronators, and supinators.
- Light resistance exercises: Using therapy putty, stress balls, and gradually progressing to light weights (e.g., 0.5-1 kg) for wrist flexion, extension, and rotation.
- Grip strengthening: With soft objects initially, progressing to hand grippers.
- Scar Management: Gentle scar massage, silicone sheeting, or topical agents to prevent scar adhesion and hypertrophy.
- Sensory Re-education: If nerve injury or paresthesia was present.
Phase 3: Advanced Strengthening & Return to Activity (Weeks 8-12+)
- Goal: Maximize strength, endurance, power, and return to functional activities, including sports and work.
- Progressive Resistance Exercises: Increase weight and resistance for all wrist, forearm, and hand muscles.
- Functional Activities: Incorporate tasks specific to the patient's work, hobbies, or sports (e.g., throwing, gripping tools, typing).
- Proprioception and Coordination: Balance exercises, activities requiring fine motor control.
- Impact Loading: Gradually introduce activities involving impact or weight-bearing through the wrist (e.g., push-ups, modified planks) as tolerated and with radiographic evidence of solid union.
- Return to Sport/Work: A gradual return is advised, typically after 3-6 months, depending on the demands of the activity and individual progress. Full radiographic union is usually confirmed.
Special Considerations
- Elderly Patients: May require a slower progression, focusing on basic activities of daily living (ADLs) and fall prevention.
- Non-Operative Cases: Immobilized for 4-6 weeks in a cast. Following cast removal, rehabilitation proceeds similarly to post-operative protocols, albeit often with more initial stiffness.
- Complex Regional Pain Syndrome (CRPS): Vigilance for CRPS symptoms (pain out of proportion, swelling, skin changes, allodynia). Early diagnosis and aggressive multimodal management (medications, sympathetic blocks, desensitization, physical therapy) are critical.
Throughout all phases, patient education regarding proper body mechanics, activity modification, and adherence to the home exercise program is vital. Close communication between the surgeon, physical/occupational therapist, and patient ensures optimal outcomes.
Summary of Key Literature / Guidelines
The management of Colles fractures has evolved significantly over the past several decades, driven by advancements in surgical techniques, understanding of biomechanics, and evidence-based medicine. Contemporary literature and guidelines emphasize anatomical reduction and stable fixation, particularly for displaced intra-articular fractures, to minimize the risk of post-traumatic arthritis and optimize functional outcomes.
Classification Systems
Several classification systems are utilized to describe distal radial fractures, aiding in communication, prognosis, and treatment planning:
*
Frykman Classification (1967):
Based on articular involvement (radiocarpal and/or DRUJ) and presence of ulnar styloid fracture. While comprehensive, it does not explicitly address comminution or displacement severity, which are critical for treatment decisions.
*
AO/OTA Classification (2018 revision):
A more comprehensive, alphanumeric system (23-A, B, C for extra-articular, partial articular, complete articular respectively, with further subdivisions) that categorizes fractures by location, articular involvement, and stability. It is widely used in research and highly detailed.
*
Universal Classification (Cooney et al., 1980s):
Categorizes fractures based on displacement and comminution, providing prognostic information regarding stability and outcome with conservative treatment.
*
Fernandez Classification (1990):
Mechanistically based, categorizing fractures by the primary mode of injury (e.g., bending, shearing, compression), which helps in understanding the injury pattern and planning reduction strategies.
Evidence-Based Treatment Principles
Current guidelines, often derived from systematic reviews and randomized controlled trials, support:
*
Non-operative Management:
Remains appropriate for stable, minimally displaced, extra-articular fractures with acceptable radiographic parameters, especially in low-demand elderly patients.
*
Volar Locking Plate Fixation (VLP):
The preferred surgical method for unstable and displaced distal radial fractures, offering superior stability, anatomical reduction, and earlier return to function compared to percutaneous pinning or external fixation in many cases. Multiple studies demonstrate VLP's effectiveness in maintaining reduction and allowing early rehabilitation.
*
External Fixation:
Still has a role in managing highly comminuted fractures, open fractures, or those with severe soft tissue compromise, often in conjunction with limited internal fixation (hybrid fixation). It's particularly useful for maintaining length and alignment through ligamentotaxis.
*
Intra-articular Fractures:
Anatomical reduction of articular step-off/gap (< 1-2 mm) is critical to reduce the incidence of post-traumatic arthritis. Arthroscopy-assisted reduction may be considered for complex intra-articular fractures to directly visualize and reduce articular fragments.
*
DRUJ Management:
Concomitant DRUJ instability should be addressed. If unstable after radial fixation, treatment may range from TFCC repair to temporary K-wire stabilization.
*
Outcomes:
Functional outcomes are generally good with appropriate management. However, malunion remains a significant concern, leading to pain, decreased range of motion, and grip strength. Patient-reported outcome measures (e.g., PRWE, DASH scores) are increasingly used to assess functional recovery.
*
Bone Quality:
Osteoporosis is a critical consideration. Poor bone quality can lead to hardware loosening, loss of reduction, and difficulties in fixation. Management often includes optimization of bone health (e.g., calcium, vitamin D, anti-resorptive agents).
Key Literature & Ongoing Debates
- SWIFFT Trial: A multicenter randomized controlled trial comparing volar locking plate to external fixation for unstable distal radial fractures, which showed comparable functional outcomes at 1 year, suggesting external fixation remains a viable option for certain fracture patterns.
- Optimal Volar Tilt: While anatomical volar tilt (11-12 degrees) is the goal, the exact threshold for "acceptable" dorsal angulation remains debated, especially in elderly, low-demand patients where slight dorsal tilt may be tolerated without significant functional deficit.
- Role of Arthroscopy: The utility of arthroscopy in routine distal radius fracture management is still under investigation. It offers direct visualization of articular reduction and identification of ligamentous injuries, but increases operative time and complexity.
- Bone Grafting: The necessity of bone grafting for metaphyseal defects, particularly in osteoporotic bone, is debated. While some advocate for routine grafting, the stability provided by modern locking plates often negates this need, with graft reserved for large defects.
In conclusion, the contemporary management of Colles fractures is guided by a blend of anatomical principles, biomechanical understanding, and robust clinical evidence, aiming to restore wrist function, prevent complications, and meet patient-specific demands. The emphasis on anatomical reduction and stable internal fixation, predominantly with volar locking plates, represents the standard of care for most unstable distal radial fracture patterns.
You Might Also Like