Clavicle Fractures: Unraveling Girdle and Humerus Injuries
Key Takeaway
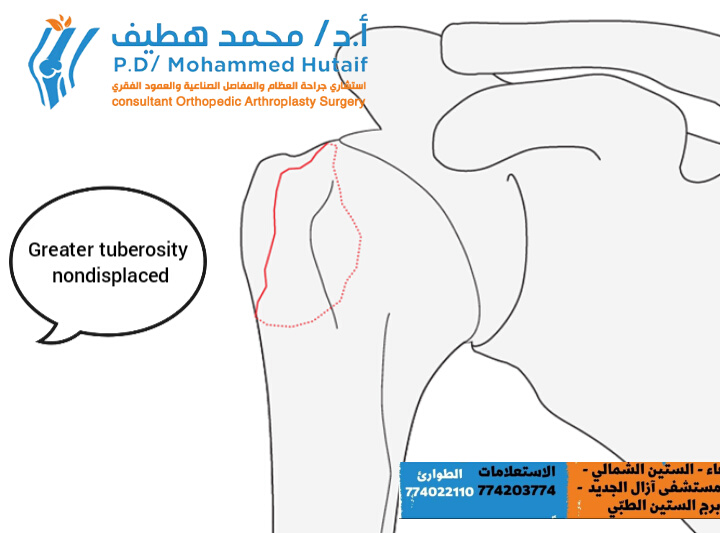
This topic focuses on Clavicle Fractures: Unraveling Girdle and Humerus Injuries, Clavicular injuries, affecting the shoulder **girdle**, commonly result from direct blows or falls on an outstretched hand, potentially impacting the function of the **humerus**. Fractures predominantly occur in the central clavicle, often presenting as greenstick or undisplaced types. These typically heal rapidly with minimal intervention, diagnosed via clinical findings and radiographs, highlighting the shoulder's resilience.
Clavicle Fractures: Unraveling Girdle and Humerus Injuries
Introduction & Epidemiology
Clavicle fractures represent a common injury, accounting for approximately 2-5% of all fractures in adults and up to 10-15% of all fractures in children. Historically, these injuries were predominantly managed non-operatively, a paradigm largely rooted in the perception of the clavicle as a non-critical structural element and the high rate of healing observed, particularly in pediatric populations. However, evolving understanding of shoulder girdle biomechanics, long-term functional outcomes, and advancements in surgical techniques have led to a reevaluation of this conservative approach, especially for significantly displaced fractures in active adults.
The clavicle, forming the anterior component of the shoulder girdle, serves as a strut between the sternum and the scapula, protecting vital neurovascular structures, facilitating upper extremity range of motion, and transmitting forces from the axial skeleton to the arm. Its exposed subcutaneous position makes it vulnerable to direct and indirect trauma.
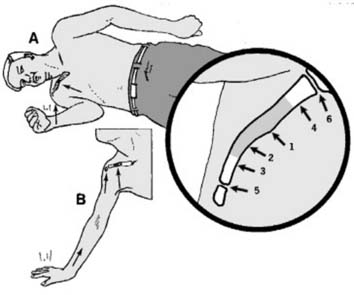
Most clavicular injuries (approximately 94%) result from a direct blow to the point of the shoulder, typically from a fall directly onto the side (Mechanism A in Illustration 1). Less commonly, the force may be transmitted proximally up the arm from a fall on an outstretched hand (Mechanism B in Illustration 1). In individuals under 30 years of age, road traffic accidents and sporting injuries are the most common etiologies.
Fractures of the clavicle are classically divided into three anatomical zones, based on Allman's classification or Neer's modification, corresponding to the medial, middle, and lateral thirds:
*
Middle Third (Zone 1 or Group I):
This central 3/5 segment is involved in approximately two-thirds of all clavicular fractures. Within this group, fractures at the junction of the middle and outer thirds are particularly common. These fractures are often comminuted or significantly displaced due to muscle forces.
*
Lateral Third (Zone 2 or Group II):
Fractures of the outer 1/5 of the clavicle are much less common, accounting for 15-25% of cases. These are further subclassified by Neer based on their relationship to the coracoclavicular ligaments, which dictate stability.
*
Medial Third (Zone 3 or Group III):
Fractures of the inner 1/5 of the clavicle are the least common, representing only 5-10% of cases. These often involve significant force and require careful assessment for associated sternoclavicular (SC) joint injuries or mediastinal compromise.
In addition to fractures, injuries to the clavicle can include subluxations and dislocations of its articulations. The acromioclavicular (AC) joint (5 in Illustration 1) is a common site of injury, typically from direct trauma to the shoulder. Fractures of the clavicle involving the AC joint are uncommon (approximately 2.8% of clavicle fractures). The sternoclavicular (SC) joint (6 in Illustration 1) can also be affected, though dislocation is rare, usually resulting from high-energy trauma, and can be associated with life-threatening complications.
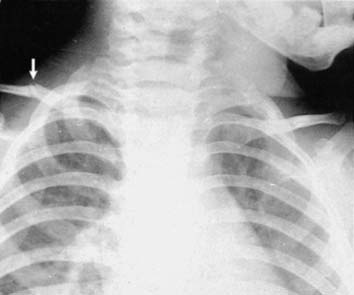
Illustration 2 depicts common patterns of fracture. Greenstick fractures are frequently observed in pediatric populations, particularly at the junction between the middle and outer thirds. Radiographic evaluation in children may not always clearly demonstrate the fracture line, necessitating comparison views of the contralateral shoulder to identify subtle cortical abnormalities or angulation.
Surgical Anatomy & Biomechanics
The clavicle is a unique long bone, possessing an S-shape and being the first bone to ossify (intramembranous ossification) and the last to fuse (20-25 years of age). It lacks a medullary cavity in its middle third, instead featuring dense cortical bone, which transitions to cancellous bone at its flared ends.
Clavicular Zones and Ligamentous Attachments
- Medial Clavicle: Articulates with the sternum via the sternoclavicular joint, a true synovial saddle joint. Stabilizing ligaments include the anterior and posterior sternoclavicular ligaments, costoclavicular ligament (rhomboid ligament), and interclavicular ligament. Muscle attachments include the sternocleidomastoid superiorly (causing superior displacement of the medial fragment in midshaft fractures) and pectoralis major inferiorly.
- Middle Clavicle: This is the weakest point, at the transition from convex to concave curvature. It is largely devoid of direct muscle attachment, but the forces from the sternocleidomastoid and trapezius (superiorly) and pectoralis major and deltoid (inferiorly) acting on the fragments cause characteristic displacement. The weight of the arm and pull of the pectoralis major and latissimus dorsi cause inferior and medial displacement of the distal fragment, while the sternocleidomastoid pulls the proximal fragment superiorly.
- Lateral Clavicle: Articulates with the acromion via the acromioclavicular joint, a plane synovial joint. Key stabilizers are the strong coracoclavicular ligaments (conoid and trapezoid, which resist superior displacement of the clavicle relative to the coracoid) and the weaker acromioclavicular ligaments. The deltoid and trapezius muscles attach here. Neer's classification for lateral clavicle fractures is critical, distinguishing types based on their relationship to the coracoclavicular ligaments and thus their stability.

Illustration 3: Demonstrates the ligamentous and muscular attachments to the clavicle, highlighting their role in fracture displacement.
Neurovascular Structures
The inferior aspect of the clavicle, particularly the middle and medial thirds, is in close proximity to critical neurovascular structures within the thoracic outlet:
*
Subclavian Artery and Vein:
Pass posterior to the clavicle.
*
Brachial Plexus:
Inferior to the subclavian artery.
*
Lung Apex and Pleura:
Medial to the first rib and posterior to the medial clavicle.
Fracture fragments, particularly in comminuted or highly displaced injuries, can impinge upon or lacerate these structures, necessitating urgent surgical intervention. Careful dissection and protection of these structures are paramount during open reduction and internal fixation (ORIF). The supraclavicular nerves, sensory branches of the cervical plexus, cross the operative field and are often sacrificed or at risk during surgical approaches, leading to an area of numbness inferior to the incision.
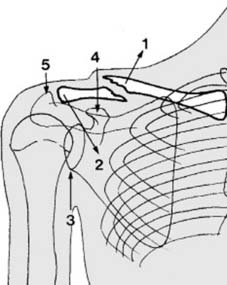
Illustration 4: A deeper anatomical view illustrating the proximity of the subclavian artery, vein, and brachial plexus to the posterior aspect of the clavicle, emphasizing the risks associated with fracture displacement and surgical intervention.
Indications & Contraindications
The decision for operative versus non-operative management of clavicle fractures has evolved significantly. While non-operative treatment remains the standard for many minimally displaced and stable fractures, particularly in children, evidence suggests superior functional outcomes and lower rates of symptomatic nonunion with surgical intervention for specific fracture patterns in adults.
Non-Operative Indications
- Minimally displaced middle-third clavicle fractures (<1-2 cm shortening or displacement).
- Stable lateral clavicle fractures (Neer Type I, III, IV) without significant AC joint disruption.
- Medial clavicle fractures without significant displacement or neurovascular compromise.
- Greenstick fractures and physeal injuries (Salter-Harris I/II) in children.
- Patients with significant medical comorbidities that contraindicate surgery.
- Patients with low functional demands.
Operative Indications
Absolute Indications:
*
Open fractures:
Risk of infection and nonunion.
*
Neurovascular compromise:
Acute or impending injury to the brachial plexus or subclavian vessels, requiring immediate decompression and repair.
*
Skin tenting/impending skin compromise:
Sharp fracture fragments threatening skin perforation.
*
Ipsilateral floating shoulder:
Displaced clavicle fracture combined with a displaced scapular neck or body fracture.
*
Displaced medial clavicle fractures:
With retrosternal displacement causing tracheoesophageal compression or severe mediastinal injury.
Relative Indications (Adults):
*
Significant displacement/shortening:
Middle-third fractures with >2 cm shortening, >100% displacement (completely separated fragments), or significant angulation (e.g., >30 degrees).
*
Comminution:
Extensive comminution, particularly with Z-deformity, which increases the risk of nonunion.
*
Young, active, high-demand patients:
Desire for early return to activity and optimal functional outcome.
*
Symptomatic nonunion:
Persistent pain, weakness, or nerve impingement from a previously non-operatively managed fracture.
*
Distal clavicle fractures:
* Neer Type II (conoid and trapezoid ligaments ruptured, fragment medial to ligaments): High risk of nonunion due to superior displacement of the medial fragment.
* Neer Type V (fracture through the base of the coracoid process): Significant instability.
*
Medial clavicle fractures:
With significant displacement and symptomatic nonunion, or persistent instability of the SC joint.
*
Polytrauma patients:
Facilitates earlier mobilization and rehabilitation.
Contraindications
- Active infection in the surgical field.
- Severe medical comorbidities precluding safe anesthesia and surgery.
- Non-displaced fractures for which non-operative management is clearly indicated.
- Poor bone quality that may compromise hardware fixation.
Summary of Operative vs. Non-Operative Indications
| Indication Type | Non-Operative Management | Operative Management (ORIF) |
|---|---|---|
| Middle Third | Minimally displaced (<2 cm shortening, <100% displacement), stable pediatric fractures | >2 cm shortening, >100% displacement, significant comminution, Z-deformity, impending skin compromise, ipsilateral floating shoulder, symptomatic nonunion |
| Lateral Third | Neer Type I, III, IV (stable) | Neer Type II, V (unstable), symptomatic nonunion, significant AC joint disruption (some Type III) |
| Medial Third | Minimally displaced, stable | Significant retrosternal displacement, neurovascular compromise, persistent SC joint instability, symptomatic nonunion |
| General | Patients with high surgical risk, low functional demand | Open fractures, neurovascular compromise, young/active patients seeking optimal outcome |

Illustration 5: Radiograph depicting a significantly displaced and shortened middle-third clavicle fracture, a common indication for operative fixation.

Illustration 6: Radiograph demonstrating a comminuted distal clavicle fracture (likely Neer Type II), indicating the need for careful assessment of coracoclavicular ligament integrity and often requiring operative stabilization.
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is crucial for successful outcomes in clavicle fracture fixation, minimizing complications, and optimizing surgical efficiency.
Clinical Assessment
- Detailed history and physical examination, including a comprehensive neurovascular assessment of the ipsilateral upper extremity. Documentation of any pre-existing nerve deficits is critical.
- Assessment for skin tenting, open wounds, or signs of impending skin compromise.
- Evaluation for associated injuries, particularly to the chest wall, lung (pneumothorax), and shoulder girdle (e.g., glenoid or scapular fractures).
Imaging
- Standard Radiographs: Anteroposterior (AP) view of the shoulder with 10-15 degrees cephalic tilt (serendipity view) to better visualize the medial clavicle, and a true AP view of the clavicle. The cephalic tilt view helps to separate the clavicle from overlying structures and visualize vertical displacement.
- CT Scan: Indicated for complex fracture patterns (e.g., comminuted midshaft fractures), medial clavicle fractures (to assess retrosternal displacement and mediastinal involvement), suspected nonunions, or when contemplating the use of pre-contoured plates. CT angiography may be necessary if neurovascular injury is suspected.
- MRI: Rarely indicated for acute fractures, but may be useful for evaluating soft tissue injuries, such as rotator cuff tears, or for chronic pain after fracture healing.

Illustration 7: Standard AP radiograph of the clavicle, often insufficient on its own for full assessment of displacement, particularly in the medial third.
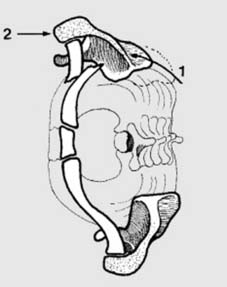
Illustration 8: A 45-degree cephalic tilt view (often referred to as a "serendipity view" for SC joint, or specifically a caudal tilt view for clavicle) which aids in delineating vertical displacement and overlapping structures, especially helpful for medial and comminuted midshaft fractures.
Hardware Selection
-
Midshaft Fractures:
- Plates: Low-profile, pre-contoured locking plates are the preferred implant. Superior plating is traditionally common, but anteroinferior plating may offer biomechanical advantages with potentially less hardware prominence, though requiring more meticulous dissection.
- Intramedullary Nailing: Less common, typically reserved for simple fracture patterns or cases where plate prominence is a major concern. Offers minimal soft tissue disruption but may not provide rigid fixation for comminuted fractures.
-
Distal Clavicle Fractures (Type II, V):
- Hook Plate: Provides temporary fixation by hooking under the acromion, but often causes impingement and requires subsequent removal.
- Distal Clavicle Specific Plates: Low-profile locking plates with extended lateral purchase are increasingly favored, sometimes combined with coracoclavicular ligament reconstruction (e.g., suture button fixation, allograft).
- Coracoclavicular Ligament Reconstruction: Independent reconstruction (e.g., use of suture button devices, allograft) can be used alone or in conjunction with plate fixation for Neer Type II fractures.
- Medial Clavicle Fractures: Small fragment plates (1/3 tubular or reconstruction plates), K-wires (rarely, due to migration risk), or tension band wiring.
Patient Positioning and Anesthesia
- Anesthesia: General endotracheal anesthesia is standard. Regional nerve blocks (e.g., interscalene block) can provide excellent post-operative pain control.
-
Positioning:
- Beach Chair Position: Preferred by many surgeons, allowing for concurrent assessment of shoulder range of motion and easier access to the AC joint if needed. The arm should be freely movable.
- Supine Position: With a rolled towel or bump placed longitudinally along the spine, elevating the ipsilateral shoulder. This allows the shoulder to fall posteriorly, opening up the fracture site and making reduction easier. The arm is typically draped free to allow intraoperative manipulation.
- Sterile Prep and Drape: The entire shoulder, chest, and ipsilateral upper extremity are prepped and draped to allow for wide exposure and free manipulation of the arm during reduction maneuvers.
Detailed Surgical Approach / Technique
Surgical repair of clavicle fractures aims to achieve anatomical reduction, stable internal fixation, and early functional rehabilitation. The specific technique varies based on fracture location and morphology.
General Principles for Open Reduction Internal Fixation (ORIF)
- Incision: A curvilinear incision parallel to the clavicle, typically 1-2 cm inferior to its superior border, allows for superior plating and minimizes the risk of supraclavicular nerve injury while allowing for better cosmesis than a straight incision. The length should be adequate to expose both fracture fragments and allow for plate placement without excessive soft tissue retraction.
-
Dissection:
- Sharp dissection through skin and subcutaneous tissue.
- Identification and careful retraction or sacrifice of the supraclavicular nerves. Patients should be counseled pre-operatively about potential numbness distal to the incision.
- Incise the platysma muscle (if applicable to the level of incision) and deepen the dissection to the periosteum.
- Elevate the periosteum minimally to expose the fracture fragments, preserving as much periosteal blood supply as possible.
-
Reduction:
- The fracture fragments are often significantly displaced by muscle pull. The medial fragment is typically pulled superiorly by the sternocleidomastoid, and the lateral fragment is pulled inferiorly and medially by the deltoid, pectoralis major, and gravity.
- Reduction often involves a combination of traction on the arm, manipulation of the fragments with reduction clamps (e.g., pointed reduction clamps, Verbrugge clamps), and counter-pressure on the chest wall.
- Temporary K-wire fixation can be used to maintain reduction while applying the plate.
- For highly comminuted fractures, achieving absolute anatomical reduction of all fragments may not be feasible or necessary. The goal is to restore overall length, alignment, and rotation of the clavicle.
-
Plate and Screw Fixation:
-
Plate Positioning:
- Superior Plating (Midshaft): Traditionally common. Plate is placed on the superior surface of the clavicle. This position is generally considered biomechanically acceptable for simple fracture patterns.
- Anteroinferior Plating (Midshaft): Increasingly favored due to biomechanical studies suggesting improved stability against bending and torsion, and potentially less hardware prominence on the superior surface. However, this requires more careful dissection to avoid neurovascular structures inferiorly.
-
Screw Insertion:
- Bicortical screw fixation is generally preferred for maximum stability. Screw lengths must be carefully measured to avoid neurovascular injury.
- At least 3 bicortical screws on each side of the fracture are ideal, ensuring adequate working length.
- Locking plates are advantageous in comminuted fractures or in osteoporotic bone, as they provide angular stability regardless of screw purchase in the far cortex.
-
Plate Positioning:
-
Wound Closure:
- Irrigation of the wound.
- Meticulous layered closure of the platysma (if cut), subcutaneous tissue, and skin. Drain placement is usually not necessary.
Specific Considerations by Fracture Type
1. Midshaft Clavicle Fractures (Group I)
- Approach: Curvilinear incision centered over the fracture site.
- Reduction: Achieve reduction by pulling the arm out to length, distracting the distal fragment laterally, and applying direct pressure. Use pointed reduction clamps or a Verbrugge clamp to hold reduction.
-
Fixation:
Pre-contoured locking compression plates are the standard.
- Superior plating: Plate is contoured to the S-shape of the clavicle. Screws are inserted carefully, avoiding the inferoposterior cortex where neurovascular structures lie.
- Anteroinferior plating: Plate is applied to the anterior or anteroinferior surface. This requires meticulous dissection of the deltopectoral fascia and protection of neurovascular structures. The plate contouring may be more challenging.
- Intramedullary Nailing: Less common for displaced comminuted fractures. Can be useful for simple transverse or short oblique fractures. Insertion can be antegrade or retrograde. Requires careful consideration of entry point and potential hardware migration.
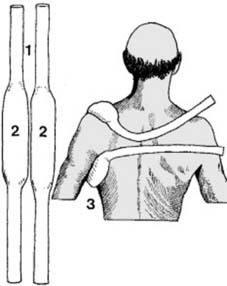
Illustration 9: Intraoperative view of a midshaft clavicle fracture being reduced with a pointed reduction clamp, prior to plate application.
Illustration 10: Intraoperative image demonstrating the application of a pre-contoured locking plate to the superior surface of a midshaft clavicle fracture after reduction has been achieved.
2. Lateral Clavicle Fractures (Group II, Neer Type II, V)
- These are more complex due to the involvement of the coracoclavicular (CC) ligaments and the AC joint.
- Approach: Incision centered over the distal clavicle and AC joint.
- Reduction: Restore alignment of the distal clavicle to the acromion and reduce any superior displacement of the medial fragment.
-
Fixation Options:
- Hook Plate: Placed on the superior surface of the clavicle with the hook engaging the undersurface of the acromion. Provides stability by holding the clavicle down to the scapula. Disadvantages include acromial erosion, impingement symptoms, and requirement for hardware removal (typically 3-6 months).
- Distal Clavicle Specific Locking Plate: These plates have multiple small screws for distal fragment fixation and can be combined with CC ligament reconstruction. They typically offer a lower profile than hook plates.
- Coracoclavicular (CC) Ligament Reconstruction/Repair: For Neer Type II fractures where CC ligaments are disrupted, reconstruction with suture buttons (e.g., TightRope, DogBone) or allograft can stabilize the clavicle relative to the coracoid. This is often performed in conjunction with a plate for added stability or alone for some patterns.
- Tension Band Wiring/Cerclage: K-wires and cerclage wires (often incorporating the coracoid) are historical options, but associated with high rates of hardware failure and migration.
Illustration 11: An intraoperative image depicting fixation of a distal clavicle fracture using a pre-contoured locking plate designed for the lateral clavicle, often with screws specifically targeting the coracoid process or combined with CC ligament repair.
3. Medial Clavicle Fractures (Group III)
- Rare, and usually managed non-operatively. Surgical fixation is challenging due to the small bone fragments, proximity to mediastinal structures, and high cosmetic concerns.
- Approach: Curvilinear incision over the sternoclavicular joint.
- Reduction: Careful manual reduction, potentially with traction on the arm. Retrograde displacement into the mediastinum is a true emergency and may require cardiothoracic surgeon involvement for safe reduction.
- Fixation: Small fragment plates (e.g., 1/3 tubular or reconstruction plates) are difficult to apply due to the small size of the medial fragment. Tension band wiring or screw fixation through the medial clavicle into the sternum (trans-articular, rarely recommended due to hardware migration risk and SC joint fusion) are options. Suture repair of the costoclavicular ligament may be considered for stability.

Illustration 12: Post-operative radiograph demonstrating stable fixation of a clavicle fracture with a plate and screws, highlighting good alignment and appropriate screw length.
Complications & Management
Despite advancements in surgical techniques, complications can occur with operative fixation of clavicle fractures. Meticulous surgical technique, appropriate patient selection, and comprehensive post-operative care are essential to minimize these risks.
Table of Common Complications
| Complication | Incidence | Management / Salvage Strategies |
|---|---|---|
| Nonunion | 2-15% (lower with ORIF vs. non-op for displaced fractures) | Revision ORIF, often with structural or cancellous autogenous bone graft (iliac crest, fibula) or allograft. Plate exchange to a stiffer construct or dual plating. |
| Malunion | Highly variable, often asymptomatic; symptomatic in 10-30% of non-op treated displaced fractures | Asymptomatic: Observation. Symptomatic (pain, impingement, dysesthesia): Corrective osteotomy and ORIF, potentially with bone graft. |
| Hardware Prominence / Irritation | 10-50% (higher with superior plating, hook plates) | Hardware removal after fracture union. For hook plates, removal is often mandatory due to acromial impingement. |
| Infection | 1-5% (superficial or deep) | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, IV antibiotics, hardware retention if fracture is united; hardware removal and debridement if nonunion or ongoing infection. |
| Neurovascular Injury | <1% (brachial plexus, subclavian vessels, pneumothorax) | Intraoperative: Immediate repair, vascular/thoracic surgery consultation. Post-operative (e.g., pseudarthrosis with nerve impingement): Excision of bone spur, neurolysis, revision fixation. |
| Wound Dehiscence | 1-5% | Local wound care, secondary closure, debridement if necrotic tissue. |
| Refracture | 1-5% (often after hardware removal or inadequate healing) | Repeat ORIF, often with a stronger construct or bone graft. |
| Stiffness / Range of Motion Loss | Variable, often multifactorial | Intensive physical therapy, pain management. Rarely, manipulation under anesthesia or arthroscopic capsular release. |
| CRPS (Complex Regional Pain Syndrome) | Rare, but debilitating | Multidisciplinary pain management, physical therapy, sympathetic blocks. |
| Sural Nerve Dysfunction (from graft harvest) | Up to 10-20% (for fibula graft) | Observation, neurolysis if persistent and severe. |
Management Strategies
- Nonunion: The most significant complication of clavicle fractures, particularly in displaced midshaft fractures treated non-operatively, with reported rates as high as 15-30%. Risk factors include significant displacement/shortening, comminution, polytrauma, smoking, and early return to activity. Operative treatment of symptomatic nonunion involves meticulous debridement of the fibrous tissue at the fracture site, freshening of bone ends, anatomical reduction, rigid internal fixation (often with a stronger plate or dual plating), and autogenous bone grafting (e.g., from the iliac crest or distal radius) to stimulate healing.
- Malunion: Often asymptomatic. If symptomatic (pain, neurological symptoms, shoulder dysfunction, cosmetic deformity), a corrective osteotomy with ORIF may be considered.
- Hardware Prominence: Given the subcutaneous location of the clavicle, hardware prominence is common and a leading cause of patient dissatisfaction, often necessitating hardware removal. This is typically performed after complete radiographic union, usually 12-18 months post-operatively.
- Infection: Requires prompt recognition and aggressive management. Superficial infections may respond to oral antibiotics. Deep infections often require surgical debridement, intravenous antibiotics, and potentially hardware removal if the fracture is united or if the infection cannot be controlled with implants in situ.
- Neurovascular Injury: While rare, direct injury to the subclavian vessels or brachial plexus can be devastating. Careful surgical technique, particularly when drilling and inserting screws, is paramount. Proximal screw holes carry the highest risk. Intraoperative neurovascular consultation should be readily available for suspected injuries.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for optimizing functional outcomes, restoring range of motion, and ensuring a safe return to activity while protecting the fracture fixation. Protocols are typically phased and individualized, depending on the fracture pattern, fixation stability, and patient factors.
Phase I: Protection and Pain Control (0-6 weeks)
- Goals: Protect fixation, minimize pain and swelling, initiate early controlled motion.
- Immobilization: Sling immobilization is typically used for comfort and to protect the repair. The duration varies but often 2-4 weeks.
-
Motion:
- Passive Range of Motion (PROM): Gentle pendulum exercises, passive shoulder flexion to 90 degrees, and external rotation to 30 degrees (with elbow at side) are initiated early. Avoid active abduction and flexion beyond 90 degrees for the initial weeks.
- Elbow/Wrist/Hand: Active range of motion and strengthening exercises for the elbow, wrist, and hand are encouraged immediately to prevent stiffness and maintain circulation.
- Weight Bearing: No lifting, pushing, or pulling with the affected arm. Avoid weight-bearing through the arm.
- Wound Care: Maintain clean, dry incision site.
Phase II: Early Active Motion and Strengthening (6-12 weeks)
- Goals: Restore full pain-free range of motion, initiate gentle strengthening. Progression is contingent on radiographic evidence of healing and clinical stability.
-
Motion:
- Active-Assisted Range of Motion (AAROM): Progress to AAROM and then full AROM as tolerated, including flexion, abduction, and rotation.
- Scapular Stabilization: Begin gentle isometric and isotonic exercises for scapular retractors and depressors (e.g., rows, prone extension).
-
Strengthening:
- Initiate light resistance exercises for the shoulder girdle and rotator cuff (e.g., internal/external rotation with resistance bands, light deltoid raises below 90 degrees).
- Progressive strengthening for elbow, wrist, and hand.
- Weight Bearing: Gradually increase weight-bearing activities. Avoid heavy lifting.
Phase III: Advanced Strengthening and Return to Activity (12+ weeks)
- Goals: Maximize strength and endurance, restore full function, prepare for sport-specific or work-specific activities. Return to full activity depends on solid radiographic union and achievement of full strength.
-
Strengthening:
- Progressive resistive exercises for all planes of shoulder motion.
- Focus on functional movements and sport-specific drills (if applicable).
- Plyometric exercises may be introduced for athletes.
-
Return to Activity:
- Non-contact sports: Often allowed 3-4 months post-surgery, once full strength and ROM are achieved and radiographs show solid union.
- Contact sports/heavy labor: Typically 4-6 months post-surgery, sometimes longer, requiring complete radiographic union and full strength recovery.
- Monitoring: Continued monitoring for pain, weakness, and hardware-related symptoms.
Summary of Key Literature / Guidelines
The management of clavicle fractures has undergone a significant paradigm shift, largely influenced by landmark studies and subsequent meta-analyses.
Historically, the majority of clavicle fractures were treated non-operatively with sling immobilization, based on early literature suggesting high union rates and acceptable outcomes. However, the prevalence of symptomatic malunion and nonunion, especially in significantly displaced midshaft fractures, prompted a re-evaluation.
A pivotal study was the Canadian Orthopaedic Trauma Society (COTS) randomized controlled trial (2007) , which compared operative fixation with non-operative treatment for displaced midshaft clavicle fractures in adults. This study demonstrated significantly improved functional outcomes (DASH scores), a lower rate of nonunion (4.6% vs. 13.9%), and a faster return to activity in the operatively treated group. This study was instrumental in broadening the indications for surgical intervention in displaced adult midshaft clavicle fractures.
Subsequent meta-analyses have largely supported these findings, demonstrating that ORIF for displaced midshaft clavicle fractures:
* Reduces the risk of nonunion.
* Improves functional scores (e.g., DASH, Constant-Murley).
* May accelerate return to work and sport.
* Has a higher rate of complications requiring reoperation (primarily for symptomatic hardware removal), but a lower overall complication rate compared to non-operative treatment.
For distal clavicle fractures , the evidence is less conclusive but generally supports operative intervention for Neer Type II fractures due to their high nonunion rates (approaching 30-40% with non-operative treatment) and instability. The optimal surgical technique for these fractures remains a subject of debate, with various plates, hook plates, and coracoclavicular ligament reconstruction techniques (e.g., suture button devices) showing good results. Hook plates, while effective for stabilization, often necessitate removal due to subacromial impingement.
Medial clavicle fractures remain largely managed non-operatively due to their rarity, challenges in surgical access, and proximity to vital structures. Surgical intervention is typically reserved for high-energy injuries with significant displacement, neurovascular compromise, or symptomatic nonunion.
Current guidelines from organizations like the Orthopaedic Trauma Association (OTA) and the American Academy of Orthopaedic Surgeons (AAOS) generally advocate for individualized treatment based on fracture location, displacement, patient age, activity level, and comorbidities. The trend has shifted towards offering operative fixation for significantly displaced or shortened middle-third clavicle fractures in active adults, and for unstable distal clavicle fractures. The choice of implant (e.g., superior vs. anteroinferior plating) continues to be debated, with biomechanical studies often favoring anteroinferior plating for rigidity but superior plating for ease of application and lower potential for deep neurovascular injury.
Ongoing research continues to refine surgical techniques, implant design, and rehabilitation protocols to further optimize outcomes and minimize complications for this common and functionally important injury.
You Might Also Like