Nutritional Rickets: Epidemiology, Pathophysiology, and Orthopedic Surgical Management
Key Takeaway
Nutritional rickets is a bone mineralization disorder primarily from vitamin D or calcium deficiency, leading to defective endochondral ossification. While initial treatment is medical, severe skeletal deformities like genu varum, coxa vara, or pathologic fractures often necessitate orthopedic surgical intervention to correct alignment and improve function.
Nutritional Rickets: Your Nutritional Guide to Treatment
Introduction & Epidemiology
Nutritional rickets, primarily a disorder of impaired mineralization of growth plate cartilage and bone matrix, remains a significant global health concern. While preventable, its persistent prevalence, particularly in vulnerable populations, underscores the need for robust diagnostic and management strategies, including surgical interventions for its orthopedic sequelae.
The fundamental pathophysiology involves inadequate availability or utilization of vitamin D, calcium, or phosphate, leading to defective endochondral ossification and osteomalacia. The most common forms are:
-
Vitamin D–Deficiency Rickets:
- Historically rare in developed nations after vitamin D fortification of milk and other foods, but resurgence has been noted in specific at-risk populations.
-
High-Risk Populations:
- Asian immigrants, especially those with darker skin pigmentation and limited sun exposure.
- Patients with dietary peculiarities, including strict vegan diets without supplementation or those with lactose intolerance avoiding fortified dairy.
- Premature infants, due to inadequate vitamin D stores at birth and rapid growth.
- Patients with malabsorption syndromes (e.g., celiac sprue, inflammatory bowel disease, cystic fibrosis), impairing intestinal absorption of fat-soluble vitamins and calcium.
- Patients receiving long-term parenteral nutrition without adequate vitamin D or mineral supplementation.
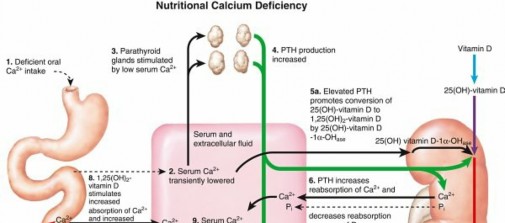
- Pathophysiology: Decreased intestinal absorption of calcium and phosphate leads to hypocalcemia. This stimulates secondary hyperparathyroidism (HPT) in an attempt to normalize serum calcium. Elevated parathyroid hormone (PTH) enhances renal phosphate excretion and increases bone resorption, further exacerbating bone demineralization.
-
Laboratory Findings:
- Low-normal serum calcium level (often maintained by high PTH).
- Low serum phosphate level (due to PTH-mediated renal excretion).
- Increased alkaline phosphatase (ALP) level (a marker of osteoblast activity and bone turnover, elevated in response to impaired mineralization).
- Low serum 25-hydroxyvitamin D [25(OH)D] level.
- Increased PTH level (secondary hyperparathyroidism).
-
Physical Examination Findings:
- Enlargement of the costochondral junction (rachitic rosary) due to physeal hypertrophy.
- Bowing of the knees (genu varum) or genu valgum, most prominent in lower extremities due to weight-bearing.
- Muscle hypotonia, contributing to weakness and gait disturbances.
- Dental disease, including enamel hypoplasia and delayed eruption.
- Pathologic fractures (Looser zones or pseudofractures on compression sides of bones, Milkman’s fractures).
- Waddling gait, often secondary to proximal muscle weakness and lower limb deformities.
-
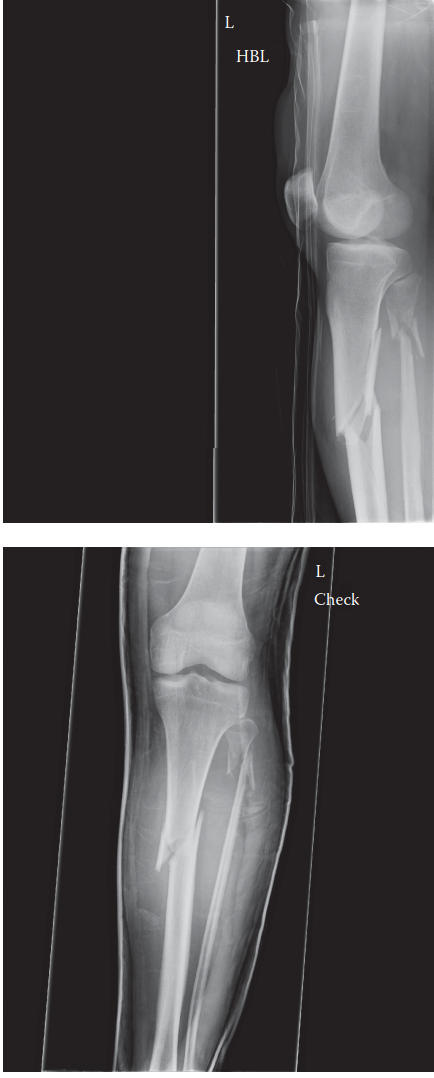
Radiographic Findings:
- Physeal widening and cupping at the metaphyses (e.g., distal femur, proximal tibia, distal radius/ulna).
- Coxa vara, with a decreased femoral neck-shaft angle.
- Codfish vertebrae (biconcave vertebral bodies) due to weakened bone and disc expansion.
- Retarded bone growth, reflecting the defect in the hypertrophic zone of the physis and widened osteoid seams.
- Looser zones, appearing as unmineralized osteoid bands perpendicular to the cortex, resembling stress fractures.
- In affected children, height is commonly below the fifth percentile for age.
-
Calcium-Deficiency Rickets:
- Less common than vitamin D deficiency but can occur with extremely low calcium intake.
- Presentation is similar to vitamin D deficiency, as severe calcium deficiency can also lead to secondary hyperparathyroidism and similar bone pathology.
While the primary treatment for active rickets is medical, involving vitamin D and/or calcium supplementation, severe or persistent skeletal deformities often necessitate orthopedic surgical intervention. Initial medical management (e.g., vitamin D 1000–6000 IU daily based on weight) resolves most metabolic derangements and may allow for some spontaneous correction of deformities in young, growing children. However, uncorrected or progressive deformities that impact function, cosmesis, or contribute to pain require surgical planning and intervention.
Surgical Anatomy & Biomechanics
Nutritional rickets profoundly alters skeletal anatomy and biomechanics, setting the stage for subsequent orthopedic deformities that may require surgical correction. Understanding these alterations is critical for surgical planning.
Growth Plate (Physis)
The most striking anatomical alteration occurs at the physis. Normally, the physis is a highly organized structure responsible for longitudinal bone growth through endochondral ossification. In rickets, there is a fundamental defect in the mineralization of the cartilage matrix in the zone of provisional calcification. This leads to:
*
Physeal Widening:
Accumulation of unmineralized osteoid and disorganized hypertrophic chondrocytes.
*
Cupping and Fraying:
Irregularity and splaying of the metaphysis, giving it a "cupped" appearance on radiographs.
*
Weakness:
The disorganization and lack of mineralization make the physis mechanically weak, prone to stress, and contributes to angular deformities.
Long Bones
The long bones, particularly those undergoing rapid growth and subject to weight-bearing, are most affected:
*
Bowing Deformities:
The most common and clinically significant deformity. The softened bone, combined with muscular pull and weight-bearing forces, leads to progressive bowing.
*
Genu Varum (Bowlegs):
The most frequent deformity, affecting the lower limbs. It involves a varus angulation, often with the apex at the distal femur or proximal tibia, or both. This shifts the mechanical axis medially, increasing stress on the medial compartment of the knee.
*
Genu Valgum (Knock-knees):
Less common but can also occur. This shifts the mechanical axis laterally, increasing stress on the lateral compartment.
* Anatomically, the bowing typically occurs at the metaphysis, where the bone is most active and weakest.
*
Coxa Vara:
A decreased femoral neck-shaft angle (<120 degrees) resulting from defective mineralization and abnormal loading across the hip. This alters hip joint mechanics, leading to a Trendelenburg gait and potential for premature hip osteoarthritis.
*
Pathological Fractures and Pseudofractures (Looser Zones):
The osteomalacic bone, with its wide osteoid seams and poor mineralization, is mechanically weaker and more susceptible to fractures from minimal trauma. Looser zones are areas of unmineralized osteoid mimicking stress fractures, often found perpendicular to the cortex on the compression side of bowed long bones or pelvis. Milkman's fractures are a specific type of pseudofracture.
*
Metaphyseal Flaring:
The broadened and unmineralized metaphysis contributes to the characteristic "cupping" seen radiographically.
Vertebral Column
Rickets can also affect the axial skeleton, leading to:
*
Codfish Vertebrae:
The weakened vertebral bodies are susceptible to compression, leading to biconcave deformities as the intervertebral discs expand into the softened endplates.
*
Scoliosis/Kyphosis:
Deformities of the spine can occur, though less common than limb deformities, due to poor mineralization and muscle hypotonia.
Muscle-Bone Interaction & Gait
Muscle hypotonia, a common feature of rickets, exacerbates skeletal deformities. Weakness of hip abductors and quadriceps muscles, coupled with lower limb bowing and coxa vara, contributes to a characteristic waddling gait. This abnormal gait further stresses the weakened bones and growth plates, potentially worsening deformities.

Figure 1. Radiographic image illustrating physeal widening and metaphyseal cupping characteristic of nutritional rickets in the distal radius and ulna.
The understanding of these anatomical and biomechanical changes is paramount for the orthopedic surgeon. Surgical interventions aim to restore normal alignment, improve mechanical axis, stabilize weakened bones, and promote functional recovery. This requires meticulous preoperative planning to identify the apex of deformity and select the appropriate corrective osteotomy or growth modulation technique.

Figure 2. Clinical image depicting severe genu varum (bowlegs) in a child with nutritional rickets, highlighting the significant lower limb angular deformity that may necessitate surgical correction.
Indications & Contraindications
The management of nutritional rickets primarily involves correcting the underlying metabolic derangement. However, when metabolic correction alone is insufficient, or when severe deformities persist, orthopedic intervention becomes necessary.
Non-Operative Management
Non-operative management is the initial and often definitive treatment for most cases of nutritional rickets.
-
Indications:
- Active Rickets with Mild Deformities: Young children with mild angular deformities (e.g., genu varum <10-15 degrees) that are expected to spontaneously resolve with adequate metabolic correction (vitamin D and calcium supplementation).
- Skeletal Immaturity: In children with open physes, there is significant potential for remodeling and spontaneous correction once metabolic derangements are normalized. Regular clinical and radiographic monitoring is essential.
- Flexible Deformities: Deformities that correct with manual manipulation, indicating less severe structural changes.
- Bracing: Can be used for mild to moderate flexible deformities to guide growth and encourage correction, particularly in the lower limbs. Compliance is a significant factor.
- Pathological Fractures: Many low-energy pathological fractures in rickets, once metabolic control is achieved, can heal with standard conservative management (casting, bracing) due to the robust healing potential of rachitic bone once adequately mineralized.
Operative Management
Surgical intervention is reserved for specific circumstances where non-operative approaches have failed or are deemed insufficient. Crucially, all surgical procedures for rachitic deformities must be performed after achieving adequate metabolic control to ensure proper bone healing and prevent recurrence.
-
Indications:
- Failure of Medical Treatment: Deformities that persist or progress despite prolonged (typically 6-12 months) and adequate metabolic correction.
-
Severe Angular Deformities:
- Genu varum or genu valgum exceeding 15-20 degrees, particularly if leading to significant mechanical axis deviation, functional impairment, or joint pain.
- Persistent bowing that affects gait, increases risk of falls, or causes significant cosmetic concern for the patient and family.
- Significant Limb Length Discrepancy (LLD): Resulting from asymmetrical growth disturbance or previous asymmetrical physeal injury.
- Symptomatic Coxa Vara: Leading to a Trendelenburg gait, hip pain, or significant functional limitations.
- Unstable or Malunited Pathological Fractures: Fractures that fail to heal, heal in unacceptable alignment, or are at high risk of displacement despite metabolic correction.
- Skeletal Maturity with Residual Deformity: In adolescents or young adults where no further spontaneous correction is expected, and the deformity causes pain, functional limitation, or cosmetic distress.
- Progressive Deformities: Despite stable metabolic control, indicating a fixed structural problem.
Contraindications for Operative Management
- Uncontrolled Active Rickets: This is an absolute contraindication. Surgery on unmineralized bone carries a high risk of poor healing, non-union, hardware failure, and recurrence of deformity. Metabolic stability (normalized vitamin D, calcium, phosphate, and PTH, along with decreasing ALP) must be achieved pre-operatively.
- Severe Medical Comorbidities: Patients with significant co-existing medical conditions that preclude safe anesthesia and surgical intervention.
- Poor Patient/Family Compliance: For post-operative care, including weight-bearing restrictions, bracing, and ongoing metabolic monitoring.
- Mild, Asymptomatic Deformities: Especially in young children with open physes, where conservative management and continued growth may lead to spontaneous correction.
Table: Operative vs. Non-Operative Indications for Rachitic Deformities
| Feature | Non-Operative Indications | Operative Indications |
|---|---|---|
| Metabolic Status | Active rickets (treatment in progress) | Metabolically controlled rickets (stable for >6 months) |
| Deformity Severity | Mild angular deformities (<10-15°) | Severe angular deformities (>15-20°) |
| Deformity Progression | Non-progressive or improving with metabolic treatment | Progressive despite metabolic control |
| Skeletal Maturity | Skeletally immature, significant growth potential | Skeletally mature with residual deformity; severe deformity in immature skeleton |
| Functional Impact | Asymptomatic, no significant gait disturbance | Significant gait abnormality, pain, functional limitation |
| Fractures | Stable, non-displaced pathological fractures | Unstable, displaced, or malunited pathological fractures |
| Compliance | Good for bracing and medical regimen | Good for post-operative rehabilitation and follow-up |
| Special Cases | Minor LLD, flexible foot deformities | Symptomatic coxa vara, severe LLD |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is paramount for successful surgical outcomes in patients with rachitic deformities. This phase involves a comprehensive assessment of the patient's metabolic status, thorough radiographic analysis, precise surgical strategy, and careful patient positioning.
Metabolic Control Optimization
-
Mandatory Requirement:
Surgical intervention must
never
be performed on active, uncontrolled rickets. The metabolic derangements (low vitamin D, low calcium, low phosphate, high PTH, high ALP) must be normalized or significantly improved. This ensures:
- Adequate bone quality for osteotomy healing.
- Reduced risk of non-union or delayed union.
- Minimization of hardware failure.
- Prevention of deformity recurrence.
- Timing: Typically, metabolic control should be maintained for at least 6-12 months before considering elective osteotomies. Regular monitoring of serum 25(OH)D, calcium, phosphate, PTH, and ALP levels is essential throughout this period.
Radiographic Assessment & Deformity Analysis
- Full-Length Standing Radiographs: Essential for evaluating lower limb alignment. Anteroposterior (AP) views encompassing the hip, knee, and ankle allow for accurate measurement of the mechanical axis deviation (MAD). Lateral views are also crucial for assessing sagittal plane deformities.
-
Identify Apex of Deformity:
The level of maximum angulation (apex) must be precisely identified. This can be at the physis, metaphysis, or even diaphysis. Digital templating software can aid in measuring angles such as:
- Mechanical Lateral Distal Femoral Angle (mLDFA)
- Medial Proximal Tibial Angle (MPTA)
- Joint Line Convergence Angle (JLCA)
- These measurements help localize the deformity to the femur, tibia, or both, and determine if it's articular or extra-articular.
- Limb Length Discrepancy (LLD): Measured from hip to ankle on full-length radiographs. This may require correction in conjunction with angular deformity.
- Hip Radiographs: AP pelvic view to assess coxa vara (femoral neck-shaft angle) and secondary hip dysplasia.
- Bone Quality: Assess cortical thickness, presence of Looser zones, and overall mineralization status.
Surgical Strategy
-
Type of Osteotomy:
- Closing Wedge Osteotomy: Most common for correcting genu varum/valgum, where a wedge of bone is removed. Advantages include inherent stability and shortening, which can be useful in specific cases.
- Opening Wedge Osteotomy: Involves cutting the bone and opening the gap, often requiring bone graft. Useful for lengthening simultaneously or when there is concern for iatrogenic shortening.
- Dome Osteotomy: Curved osteotomy, allows for multidirectional correction without creating a large void or wedge.
- Greenstick Osteoclasis: For milder, more flexible deformities in young children, a controlled fracture can be performed.
- Level of Osteotomy: Typically performed at the metaphysis, approximately 1-2 cm from the physis in children to avoid physeal injury, or at the apex of the deformity.
-
Fixation Method:
- Plates and Screws: Locking plates are commonly used in older children and adolescents, providing rigid fixation.
- Intramedullary Nailing: Less common for acute correction of severe angular deformities in younger children due to concerns about physeal damage, but can be considered in specific instances or for prophylactic stabilization of bones prone to fractures.
- External Fixators: Offer precise, gradual correction for complex deformities or for lengthening procedures.
- Growth Modulation (Guided Growth): For skeletally immature patients with mild-to-moderate progressive angular deformities, hemiepiphysiodesis (e.g., using a tension band plate) can be employed to slow growth on one side of the physis, allowing the deformity to correct gradually. This is a less invasive option but requires ongoing growth and careful monitoring.
Pre-operative Counseling
- Thorough discussion with the patient and family regarding the procedure, expected outcomes, potential complications, and the critical importance of post-operative compliance with weight-bearing restrictions and physical therapy.
- Reinforce the need for ongoing nutritional and metabolic management.
Patient Positioning
-
Lower Extremity Osteotomies (e.g., Proximal Tibial, Distal Femoral):
- Supine Position: Standard for most limb osteotomies.
- Padding: Ensure adequate padding for all bony prominences (heels, sacrum, ulnar nerves) to prevent pressure sores or nerve palsies.
- Tourniquet: Applied proximally on the thigh to achieve a bloodless field, typically inflated to 250-300 mmHg for adults, adjusted for pediatric patients.
- Fluoroscopy Access: Critical for intraoperative guidance. The C-arm must have full range of motion to obtain AP and lateral views, and ideally full-length views including the hip and ankle to confirm mechanical axis correction.
- Draping: Sterile draping to allow access to the entire limb, from hip to foot, and to accommodate C-arm placement.
Detailed Surgical Approach / Technique
The surgical correction of rachitic deformities primarily involves osteotomies to realign the affected bone segments. The choice of technique depends on the specific deformity, patient age, skeletal maturity, and surgeon preference. The general principles include achieving precise correction, providing stable fixation, and ensuring optimal conditions for bone healing.
General Principles for Rachitic Osteotomies
- Metabolic Control: Reiterate the absolute necessity of pre-operative metabolic normalization. Uncontrolled rickets leads to poor bone quality, increasing the risk of non-union, hardware failure, and recurrence.
- Precision: Meticulous planning with deformity analysis (mechanical axis deviation, angular measurements) is crucial for accurate correction.
- Stable Fixation: The fixation method must be robust enough to withstand early physiological loads, promote healing, and prevent loss of correction.
- Minimizing Physeal Injury: In skeletally immature patients, care must be taken to avoid damaging the growth plates during osteotomy and hardware placement.
- Multilevel Deformities: In severe cases, deformities may exist at multiple levels (e.g., distal femur and proximal tibia). These may require simultaneous or staged correction.
Angular Deformities (Genu Varum/Valgum)
The most common surgical interventions for rickets are corrective osteotomies of the distal femur and/or proximal tibia.
A. Proximal Tibial Osteotomy (for Genu Varum)
- Indications: Persistent or progressive genu varum with the apex of deformity primarily located in the proximal tibia, after metabolic correction.
- Patient Positioning: Supine with the knee flexed to 30-45 degrees, allowing access to the medial proximal tibia. A sandbag or bolster under the contralateral hip can help internally rotate the affected limb for better exposure.
-
Approach:
Medial longitudinal incision.
- Incision: A curvilinear or straight longitudinal incision is made over the anteromedial aspect of the proximal tibia, typically 5-8 cm in length, centered at the planned osteotomy site (usually 1-2 cm distal to the tibial tubercle or physis).
- Dissection: Subcutaneous dissection to expose the deep fascia. Incise the fascia along the planned incision line. Identify and protect the saphenous nerve and vein, which typically run anterior to the medial gastrocnemius. The sartorius muscle may be encountered and can be retracted anteriorly or posteriorly.
- Periosteal Elevation: Subperiosteal dissection is performed to expose the proximal tibial metaphysis, carefully elevating the periosteum anteriorly and posteriorly. Care should be taken to avoid excessive stripping, which can compromise bone vascularity.
- Osteotomy Planning: Confirm the osteotomy level and angle with intraoperative fluoroscopy. K-wires or a custom jig can be used to delineate the osteotomy lines. For a closing wedge osteotomy, the apex of the wedge is typically lateral, with the base medial, corresponding to the varus deformity. The anterior tibial cortex is usually preserved initially as a hinge, though it may be cut later for complete correction.
- Osteotomy Execution: Using an oscillating saw, the osteotomy cuts are made meticulously. The distal cut is made first, followed by the proximal cut, meeting at the planned apex (lateral cortex). The medial wedge of bone is removed. The lateral cortex is carefully greenstick fractured or completely cut, allowing for correction of the varus.
- Correction: The deformity is gently corrected by manually bringing the distal fragment into the desired alignment. Intraoperative fluoroscopy (AP and lateral views) and a full-length image intensifier view (if available) are crucial to confirm the mechanical axis alignment from hip to ankle. The goal is to achieve a neutral mechanical axis or slight valgus.
- Fixation: A pre-contoured locking plate (e.g., pediatric proximal tibia locking plate or a suitable adult locking plate in adolescents) is applied to the medial or anteromedial aspect of the tibia. Ensure stable fixation with at least two or three screws proximal and distal to the osteotomy site. Screws should achieve bicortical purchase without violating the physis (if open).
- Wound Closure: The wound is irrigated thoroughly. The periosteum is reapproximated if possible, followed by layered closure of fascia, subcutaneous tissue, and skin.
B. Distal Femoral Osteotomy (for Genu Valgum)
- Indications: Persistent or progressive genu valgum with the apex of deformity primarily located in the distal femur, after metabolic correction.
- Patient Positioning: Supine with the knee slightly flexed.
-
Approach:
Lateral longitudinal incision.
- Incision: A longitudinal incision over the lateral aspect of the distal femur, centered at the osteotomy site (1-2 cm proximal to the distal femoral physis).
- Dissection: Incise subcutaneous tissue. Identify and protect the lateral femoral cutaneous nerve. The vastus lateralis muscle is split longitudinally or reflected anteriorly. Subperiosteal dissection exposes the lateral aspect of the distal femur.
- Osteotomy Planning: Fluoroscopy is used to confirm the level and angle. For a closing wedge osteotomy, the apex is medial, with the base lateral, to correct valgus.
- Osteotomy Execution: Similar to the tibia, oscillating saw cuts are made. The medial cortex can be preserved as a hinge. The lateral wedge of bone is removed.
- Correction: Varus correction is achieved by closing the lateral wedge. Mechanical axis is confirmed with fluoroscopy.
- Fixation: A pre-contoured locking plate (e.g., pediatric distal femur locking plate) is applied laterally, providing rigid fixation.
- Wound Closure: Layered closure.
C. Growth Modulation (Guided Growth)
- Indications: Skeletally immature patients with mild-to-moderate progressive angular deformities (e.g., 5-15 degrees of varus/valgus) and significant remaining growth potential.
-
Technique:
Hemiepiphysiodesis involves surgically slowing growth on one side of the physis.
- Approach: Small incision (1-2 cm) directly over the medial (for varus) or lateral (for valgus) aspect of the physis of the distal femur or proximal tibia.
- Procedure: A small tension band plate (e.g., 8-plate) with two screws is applied, bridging the physis. The screws are placed bicortically, one proximal and one distal to the physis, compressing the physis and slowing growth on that side.
- Monitoring: Patients require regular clinical and radiographic follow-up (every 3-6 months) to monitor correction. The plate is removed once the desired alignment is achieved, to prevent overcorrection.
Coxa Vara
- Indications: Symptomatic coxa vara (Trendelenburg gait, pain, limping) that has not improved with metabolic treatment.
-
Technique:
Subtrochanteric valgus osteotomy.
- Approach: Lateral incision over the proximal femur.
- Procedure: A laterally based closing wedge osteotomy is performed in the subtrochanteric region. This increases the femoral neck-shaft angle, improving abductor mechanics.
- Fixation: A pediatric hip plate (e.g., dynamic hip screw with pediatric side plate) or blade plate is used for stable internal fixation.
- Considerations: Pre-operative templating is essential to determine the wedge size and optimal correction angle.
Pathological Fractures
-
Management:
While most rachitic pathological fractures heal with conservative measures and metabolic correction, surgical intervention may be required for:
- Displaced or Unstable Fractures: Requiring reduction and internal fixation.
- Non-unions or Malunions: After initial conservative treatment.
- Techniques: Internal fixation using plates and screws, intramedullary nails (careful with physes in children), or external fixators, depending on the fracture pattern and location. Bone quality, even post-metabolic correction, can still be suboptimal, necessitating robust fixation.
Bone Grafting
- Generally, bone grafting is not routinely required for simple corrective osteotomies in metabolically controlled rachitic bone, as its healing potential is excellent.
- It may be considered for large opening wedge osteotomies or for recalcitrant non-unions. Autogenous cancellous bone graft is typically preferred.
Complications & Management
Despite meticulous planning and execution, surgical intervention for rachitic deformities carries potential risks. Early recognition and appropriate management are crucial for optimal outcomes.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence | Management / Salvage Strategy |
|---|---|---|
| Recurrence of Deformity | Up to 10-30% in some series, especially if metabolic control lapses or in very young children with significant growth remaining. | Re-osteotomy for severe recurrence. Growth modulation (hemiepiphysiodesis) for progressive mild-moderate recurrence in skeletally immature patients. Reinforce metabolic control. |
| Non-union / Delayed Union | Relatively low if metabolic control is achieved pre-operatively (<5%), but higher in uncontrolled rickets. | Optimize metabolic status. Revision surgery with stronger fixation, possibly with bone grafting. Electrical stimulation. |
| Hardware Failure | 5-15%, often associated with non-union, inadequate fixation, or premature weight-bearing on poor quality bone. | Revision surgery with plate exchange or stronger fixation construct. Address underlying non-union. Prolonged immobilization if bone quality is poor. |
| Growth Arrest/Disturbance | <5%, primarily from iatrogenic physeal injury during osteotomy or screw placement. | If partial, may lead to angular deformity or LLD requiring contralateral epiphysiodesis or future limb lengthening. Total arrest may require lengthening. |
| Infection | Superficial: 5-10%; Deep: 1-3%. | Superficial: Oral antibiotics. Deep: Surgical debridement, intravenous antibiotics, possible hardware removal (after union). |
| Nerve/Vascular Injury | <1% (e.g., common peroneal nerve in proximal tibia osteotomy). | Intraoperative identification and repair. Post-operative neurological monitoring. Depending on severity, may require further surgical exploration. |
| Overcorrection / Undercorrection | 5-10%, often due to imprecise planning, intraoperative assessment, or post-operative settling. | Mild: May be observed. Significant: Revision osteotomy for precise realignment. Growth modulation in immature patients. |
| Compartment Syndrome | Rare (<1%), but a surgical emergency. | Immediate fasciotomy. |
| Pressure Sores/Skin Breakdown | Variable, higher with prolonged casting or tight dressings. | Prophylactic padding. Regular cast checks. Wound care for established sores. |
Detailed Management Strategies
-
Recurrence of Deformity:
The most common complication, particularly in younger children with open physes. Close post-operative monitoring of alignment is crucial. If recurrence is noted:
- First, re-evaluate and optimize metabolic control.
- For mild, progressive recurrence in skeletally immature patients, growth modulation (hemiepiphysiodesis) can be considered.
- For severe or rapidly progressing recurrence, a repeat osteotomy may be necessary.
-
Non-union/Delayed Union:
This is rare if rickets is metabolically controlled. However, if it occurs:
- Confirm optimal metabolic status (vitamin D, calcium, phosphate, PTH).
- Evaluate stability of fixation. If hardware is loose or broken, revision surgery with a more robust construct is indicated.
- Bone grafting (autogenous cancellous graft) may be considered, especially for large osteotomy gaps or revision cases.
- Pulsed electromagnetic field (PEMF) stimulation or low-intensity pulsed ultrasound (LIPUS) may be adjuncts.
- Hardware Failure: Often a consequence of non-union or poor bone quality. Requires revision surgery, removal of failed hardware, and re-fixation, typically with a stronger construct or consideration of alternative fixation methods (e.g., external fixator).
- Growth Arrest/Disturbance: Careful technique, including appropriate distance from the physis during osteotomy and precise screw placement, minimizes this risk. If partial physeal arrest occurs, it may lead to progressive angular deformity or limb length discrepancy. Salvage may involve contralateral epiphysiodesis, guided growth, or future limb lengthening.
- Infection: Standard surgical prophylaxis (pre-operative antibiotics, sterile technique) is essential. For superficial infections, oral antibiotics are often sufficient. Deep infections require surgical debridement, intravenous antibiotics, and potentially hardware removal once the osteotomy has healed.
- Nerve/Vascular Injury: Meticulous anatomical dissection and identification of neurovascular structures are paramount. Immediate intraoperative repair for identified injuries. Post-operative vigilance for signs of nerve palsy or vascular compromise.
- Overcorrection/Undercorrection: Accurate pre-operative templating and intraoperative fluoroscopic checks are critical. Mild cases may be observed. Significant malalignment may require revision osteotomy once the initial site has healed.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a critical component of successful management following surgical correction of rachitic deformities. The protocol aims to protect the osteotomy site, promote bone healing, restore function, and prevent recurrence.
Initial Post-Operative Period (0-6 Weeks)
-
Immobilization:
- Immediately post-surgery, the limb is typically immobilized in a cast (long leg or short leg, depending on the osteotomy location and stability of fixation) or a rigid brace. This protects the osteotomy from excessive forces during the early healing phase.
- Duration of immobilization varies, usually 4-8 weeks, depending on the patient's age, bone healing characteristics, and stability of internal fixation.
-
Weight-Bearing:
- Non-Weight-Bearing (NWB): Generally initiated for the first 4-6 weeks to allow for initial osteotomy consolidation. Patients use crutches or a walker.
- Partial Weight-Bearing (PWB): Gradual progression to PWB may begin after 4-6 weeks, guided by radiographic evidence of early healing (e.g., callus formation) and clinical stability. This involves touching down the foot with minimal weight (toe-touch weight-bearing), progressively increasing with therapist guidance.
- Pain Management: Opioids and NSAIDs are used as needed.
-
Physical Therapy:
- Early Phase: Focus on maintaining range of motion (ROM) in non-involved joints (e.g., ankle and hip ROM exercises for knee osteotomies), isometric muscle contractions (e.g., quadriceps sets, gluteal sets) to prevent atrophy without stressing the osteotomy, and transfer training.
- Edema Control: Elevation and gentle compression to manage swelling.
Intermediate Phase (6-12 Weeks)
- Radiographic Assessment: Regular radiographs (every 4-6 weeks) to monitor osteotomy healing. Look for progressive callus formation and bridging across the osteotomy site.
-
Weight-Bearing Progression:
- Once sufficient radiographic healing is observed and pain allows, weight-bearing progresses from PWB to full weight-bearing (FWB) over several weeks, under the guidance of a physical therapist.
- Crutches or a walker are gradually weaned as strength and balance improve.
-
Physical Therapy:
- Range of Motion: Aggressive but controlled ROM exercises for the affected joint (e.g., knee flexion/extension after tibial or femoral osteotomy) to prevent stiffness.
- Strengthening: Progressive strengthening exercises for all major muscle groups of the operated limb, focusing on quadriceps, hamstrings, hip abductors, and calf muscles. Begin with closed-chain exercises (e.g., mini-squats, leg presses) as tolerated.
- Proprioception and Balance: Exercises such as single-leg stance, balance board training, and gait re-education to improve stability and normalize walking patterns.
- Bracing: In some cases, a functional brace may be prescribed for several months during weight-bearing activities to provide additional support and prevent recurrence, especially in younger children or those with persistent bone quality concerns.
Advanced Phase (>12 Weeks)
-
Full Weight-Bearing & Activity Progression:
- Once radiographic union is confirmed and full strength is regained, patients transition to full, unrestricted weight-bearing and gradually return to age-appropriate activities.
- High-impact activities or contact sports may be restricted until robust bone healing is confirmed and significant functional improvement is achieved (often 6-12 months post-op).
- Continued Strengthening & Conditioning: Ongoing home exercise program to maintain strength, flexibility, and endurance.
- Gait Training: Address any residual gait abnormalities.
- Nutritional Follow-up: Crucial for long-term success. Regular monitoring by an endocrinologist or pediatrician to ensure continued metabolic control (vitamin D, calcium, phosphate, PTH levels) and prevent recurrence of rickets, which could compromise surgical outcomes.
- Hardware Removal: If a growth modulation plate (e.g., 8-plate) was used, it is removed once the desired correction is achieved. For corrective osteotomy plates, hardware removal is typically considered 12-24 months post-operatively, after complete bone healing and skeletal maturity, or if symptomatic.
Summary of Key Literature / Guidelines
The existing literature on nutritional rickets emphasizes a multi-disciplinary approach, with primary emphasis on medical management and surgical intervention reserved for persistent or severe deformities.
1. Medical Management Guidelines:
*
American Academy of Pediatrics (AAP) and Endocrine Society Guidelines:
Strongly recommend universal vitamin D supplementation for all infants, children, and adolescents.
* Infants (0-12 months): 400 IU/day.
* Children/Adolescents: 600 IU/day.
* Higher doses are needed for treatment of established vitamin D deficiency (e.g., 2000-5000 IU/day for 6-12 weeks, followed by maintenance).
*
Monitoring:
Regular monitoring of 25(OH)D, calcium, phosphate, PTH, and alkaline phosphatase is crucial during treatment. Resolution of elevated PTH and ALP, normalization of calcium/phosphate, and healing on radiographs indicate metabolic control.
*
Dietary Sources:
Emphasis on fortified foods (milk, cereals), fatty fish, and consideration of calcium intake.
2. Surgical Outcomes & Efficacy:
*
Osteotomies for Deformity Correction:
Numerous studies affirm the efficacy of corrective osteotomies (e.g., proximal tibial, distal femoral) in correcting severe angular deformities caused by rickets, leading to improved gait, function, and cosmesis.
*
Outcome Studies:
Report high rates of successful correction (often >90%) with significant improvement in mechanical axis alignment. Recurrence rates vary but are generally higher in very young children with significant growth remaining and if metabolic control is not rigorously maintained.
*
Fixation:
Modern locking plates have demonstrated excellent stability and success rates, minimizing complications such as loss of correction and hardware failure compared to older fixation methods.
*
Growth Modulation (Hemiepiphysiodesis):
Increasingly recognized as a viable option for skeletally immature patients with mild-to-moderate
progressive
deformities.
*
Advantages:
Less invasive than osteotomy, allows for gradual correction, and avoids the need for acute bone cuts and rigid fixation.
*
Limitations:
Requires significant remaining growth, careful monitoring to prevent overcorrection, and is not suitable for severe or fixed deformities.
*
Pathological Fractures:
Literature confirms that most rachitic fractures heal well with conservative management once metabolic derangements are corrected. Surgical fixation is reserved for unstable, displaced, or non-united fractures.
3. Importance of Multidisciplinary Care:
*
Team Approach:
Consensus highlights the critical role of a multidisciplinary team, including pediatric endocrinologists/nephrologists, orthopedic surgeons, nutritionists, and physical therapists.
*
Sequenced Management:
Metabolic stabilization
precedes
surgical intervention. Orthopedic surgeons must ensure the patient's metabolic status is optimized to facilitate bone healing and prevent post-operative complications.
*
Long-Term Follow-up:
Essential for monitoring nutritional status, detecting recurrence of rickets, assessing long-term outcomes of surgical correction, and addressing any residual growth disturbances.
In summary, nutritional rickets is fundamentally a medical condition requiring prompt nutritional and metabolic intervention. However, its significant orthopedic sequelae often necessitate surgical correction, for which meticulous pre-operative planning, precise surgical technique, stable fixation, and dedicated post-operative rehabilitation, all underpinned by sustained metabolic control, are critical for achieving optimal functional and anatomical outcomes.
Clinical & Radiographic Imaging

You Might Also Like