Optimal Straight Nailing for 2-Part Surgical Neck Fractures
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Optimal Straight Nailing for 2-Part Surgical Neck Fractures. Extraarticular 2-part surgical neck impaction fractures are intrinsically stable due to metaphyseal impaction. Nonoperative treatment with early mobilization often yields good results. Surgical intervention, like nailing, is considered for unacceptable deformity, risk of displacement, or a need for greater stability and earlier mobilization of the affected part surgical neck to achieve optimal union and alignment.
Introduction & Epidemiology
Two-part surgical neck fractures of the proximal humerus represent a common injury in orthopedic trauma, particularly affecting an aging population with diminished bone mineral density. While a significant proportion of these fractures are intrinsically stable due to impaction and can be managed non-operatively, a subset requires surgical intervention to restore acceptable alignment and facilitate early rehabilitation. Intramedullary nailing, specifically using a straight antegrade nail, has emerged as a valuable fixation option for these specific fracture patterns.
The proximal humerus is the third most common site for osteoporotic fractures, with surgical neck fractures comprising a substantial subgroup. Neer's classification, while primarily designed for 4-part fractures, identifies 2-part surgical neck fractures as those involving displacement at the surgical neck, without significant displacement or angulation of the tuberosities or articular segment. These fractures are distinct from metaphyseal head-splitting fractures or those involving the anatomical neck, which often carry a higher risk of avascular necrosis.
The rationale for utilizing a straight intramedullary nail in selected 2-part surgical neck fractures stems from several key biomechanical and surgical considerations. The intramedullary position of the implant provides robust internal fixation, particularly advantageous in osteoporotic bone where screw purchase with plate fixation can be tenuous. The load-sharing characteristics of an intramedullary device may contribute to earlier weight-bearing or mobilization, theoretically reducing the risk of implant failure or delayed union compared to load-bearing constructs. Furthermore, the antegrade approach typically involves a smaller incision and less soft tissue stripping compared to open reduction and internal fixation (ORIF) with plates, potentially preserving the local blood supply and minimizing perioperative morbidity.
However, patient selection is paramount. While these fractures are often intrinsically stable due to impaction, operative management is considered for unacceptable deformity, persistent instability, or high-demand patients for whom earlier, more predictable restoration of function is desired. This comprehensive review aims to delineate the current understanding, surgical principles, and evidence-based practices surrounding optimal straight nailing for 2-part surgical neck fractures, guiding orthopedic surgeons, residents, and medical students in their clinical decision-making.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the proximal humerus is fundamental to safe and effective intramedullary nailing. The surgical neck is defined as the region immediately distal to the humeral head and tuberosities, representing a common fracture site due to the change in cortical thickness.
Key anatomical structures relevant to straight nailing include:
*
Humeral Head and Tuberosities:
The articular segment, comprising the humeral head, greater tuberosity (insertion of supraspinatus, infraspinatus, teres minor), and lesser tuberosity (insertion of subscapularis), typically remains as a single unit in 2-part surgical neck fractures. The
supraspinatus footprint
is a critical landmark for nail entry.
*
Rotator Cuff:
The integrity and function of the rotator cuff tendons are crucial. The typical antegrade entry portal for straight nailing necessitates a trans-tendon approach through the supraspinatus. While minimized, this violation can have implications for postoperative shoulder function and pain.
*
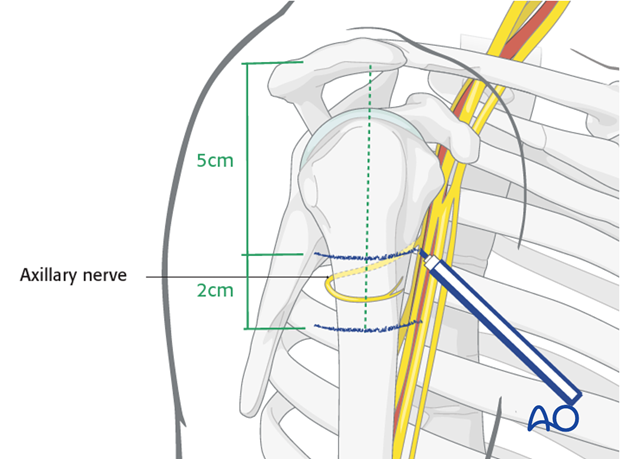
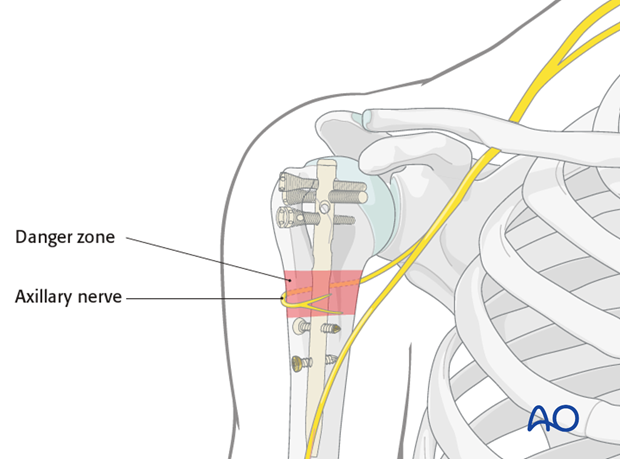
Deltoid Muscle:
The approach to the proximal humerus for nailing typically involves a deltoid-splitting incision. Understanding the innervation by the axillary nerve is critical to avoid iatrogenic injury. The axillary nerve wraps around the surgical neck, approximately 5-7 cm distal to the acromion, making it vulnerable during distal interlocking or if excessive soft tissue dissection is performed.
*
Vascular Supply:
The blood supply to the humeral head primarily originates from the anterior and posterior circumflex humeral arteries, which form an arcuate artery system. The ascending branch of the anterior circumflex humeral artery is particularly important. While 2-part surgical neck fractures generally have a lower risk of avascular necrosis (AVN) compared to anatomical neck or multi-part head fractures, excessive stripping or devitalization of soft tissues during reduction can compromise vascularity.
*
Bone Quality:
The proximal humerus is characterized by cancellous bone, particularly in the humeral head, which diminishes with age and osteoporosis. This highlights the importance of implants designed for strong purchase in poor bone quality and the load-sharing principles of intramedullary fixation.
Biomechanically, straight intramedullary nails provide excellent axial and rotational stability by engaging both the proximal humeral head and the distal diaphyseal segment.
*
Proximal Fixation:
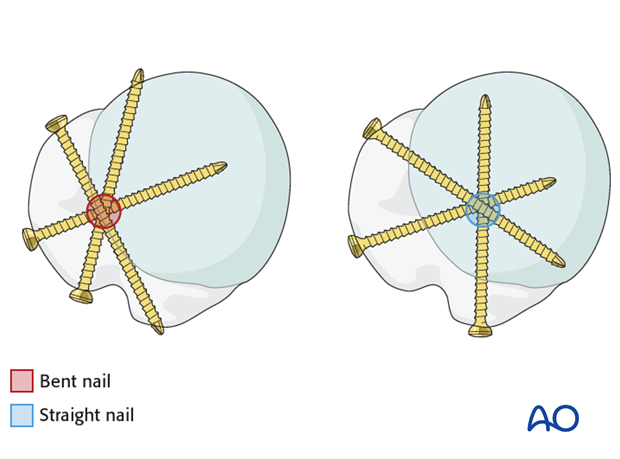
Multiple locking screws are directed into the humeral head, providing angular stability and resisting varus collapse and rotational forces. The design of modern nails often includes divergent or convergent screws to maximize purchase in the cancellous bone.
*
Distal Fixation:
Distal interlocking screws prevent shortening and rotational instability. Their placement requires careful attention to avoid neurovascular structures, particularly the radial nerve in the spiral groove.
*
Load Sharing:
Unlike plates, which are load-bearing constructs, intramedullary nails are load-sharing devices. This means that a significant portion of the axial load is transmitted through the nail itself, reducing stress shielding of the bone and potentially promoting callus formation and union. This is particularly advantageous in osteoporotic bone, where stress concentration at the plate-bone interface can lead to periprosthetic fractures.
*
Metaphyseal Impaction:
In the context of 2-part surgical neck fractures with impaction, the intrinsic stability contributes to the success of both operative and non-operative management. When surgically fixed, the nail reinforces this impaction, providing enhanced mechanical stability.
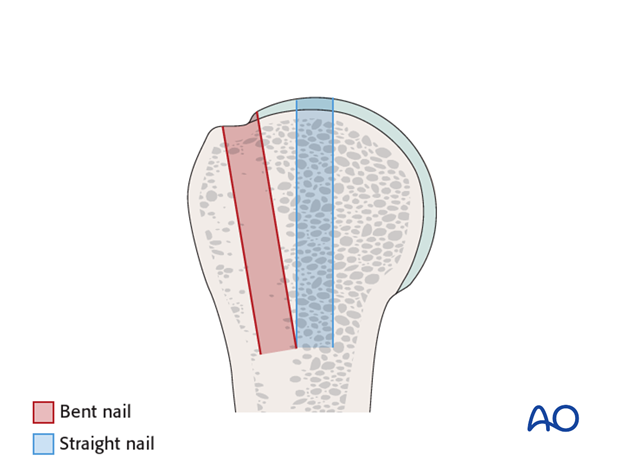
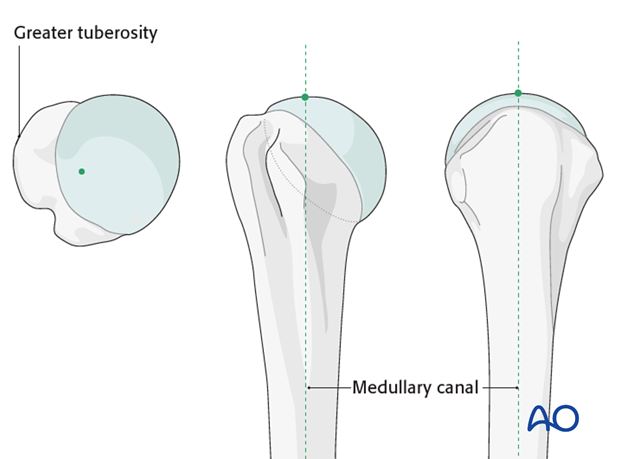
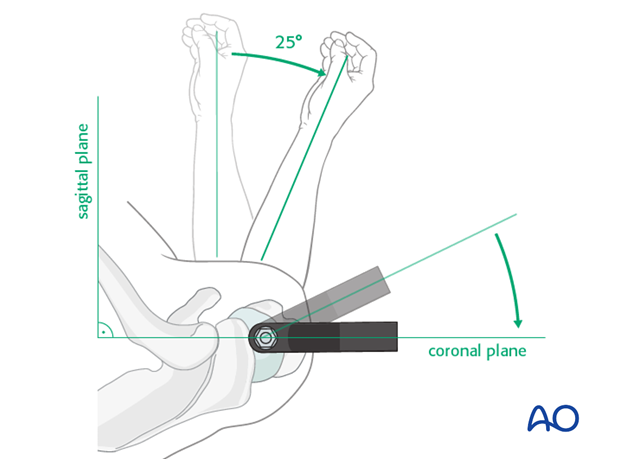
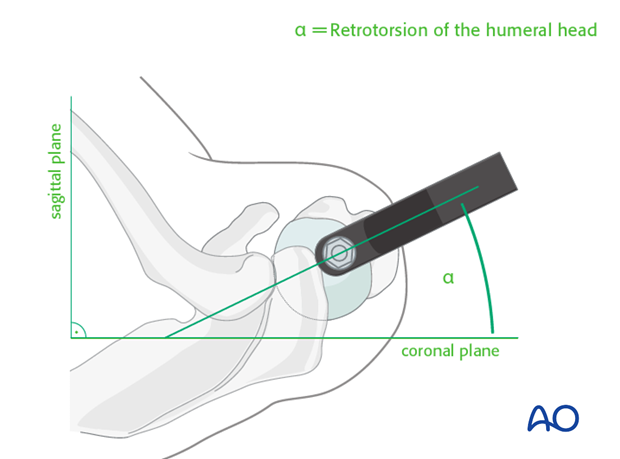
The entrance point of the nail is critical. A proper entry point, typically at the apex of the humeral head in line with the humeral shaft axis, minimizes malalignment and prevents interference with the articular surface. An improperly placed entry point (e.g., too medial) can lead to varus malreduction or impingement. An excessive lateral entry point can make nail insertion difficult and potentially compromise rotator cuff integrity further.
Indications & Contraindications
The decision to proceed with operative management for 2-part surgical neck fractures, particularly with intramedullary nailing, is based on a careful assessment of fracture characteristics, patient factors, and the surgeon's experience. While many such fractures are intrinsically stable, operative fixation is considered for those with unacceptable deformity or a high risk of displacement.
Main Indications:
*
Unacceptable Deformity:
*
Angulation:
Greater than 20-30 degrees of angulation in the coronal or sagittal plane, particularly varus angulation, which can lead to impingement and functional limitations.
*
Translation:
Greater than 1 cm translation.
*
Shortening:
Significant shortening (e.g., >1 cm).
*
Risk of Displacement:
Fractures deemed unstable despite initial impaction, especially in younger, active patients or those with poor bone quality where early motion is desired.
*
Need for More Stability and/or Earlier Mobilization:
For patients where early, controlled range of motion is crucial to prevent stiffness, such as active individuals or those with specific occupational demands.
Supporting Indications:
* Polytrauma patients where early mobilization is desired for global rehabilitation.
* Associated neurovascular injury requiring surgical exploration.
* Open fractures (though these are rare for 2-part surgical neck fractures and may require different management strategies).
Contraindications:
*
Absolute Contraindications:
* Active infection in the surgical field.
* Severe comminution of the humeral head or surgical neck making stable fixation impossible with a straight nail.
* Significant articular involvement (e.g., head-splitting fractures) that would be better addressed by arthroplasty or plating with articular reduction.
* Severe soft tissue compromise precluding safe surgical incision and wound closure.
* Patient medically unfit for surgery or anesthesia.
*
Relative Contraindications:
* Pre-existing shoulder arthritis or significant rotator cuff pathology that may complicate post-operative rehabilitation or mask surgical outcomes.
* Fractures with a very short proximal segment where adequate screw purchase for nailing is questionable.
* Morbid obesity, which can complicate surgical exposure, reduction maneuvers, and fluoroscopic imaging.
* Extremely osteoporotic bone where even intramedullary fixation may not provide sufficient stability; consider alternative fixation or augmentation.
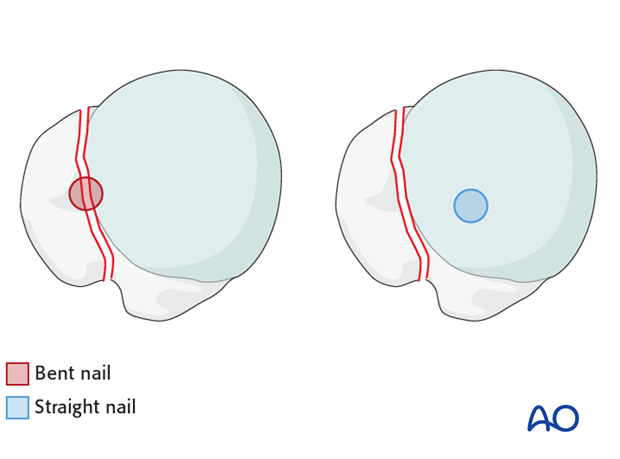
The choice of a "straight" nail implies a specific implant design intended to follow the natural bowing of the humerus without excessive reaming or stress on the cortex. This is in contrast to some older or more flexible nail designs.
Table: Operative vs. Non-Operative Indications for 2-Part Surgical Neck Fractures
| Feature | Non-Operative Management | Operative Management (Straight Nailing) |
|---|---|---|
| Fracture Angulation | Mild to moderate angulation (e.g., < 20-30 degrees varus/valgus) | Unacceptable angulation (> 20-30 degrees varus/valgus), particularly in younger, active patients. |
| Fracture Translation | Minimal translation (e.g., < 1 cm) | Significant translation (> 1 cm) |
| Fracture Shortening | Minimal shortening | Significant shortening (> 1 cm) |
| Impaction Stability | Stable impaction (varus impacted fractures often very stable) | Unstable impaction or high risk of secondary displacement after initial non-operative trial. |
| Bone Quality | Adequate bone quality for healing with external support | Poor bone quality (osteoporosis) where IM nail provides superior purchase and load sharing. |
| Patient Age/Activity | Elderly, low-demand, comorbid patients. | Active, higher-demand patients, younger individuals where optimal alignment and early function are paramount. |
| Comorbidities | Significant medical comorbidities precluding surgery. | Medically stable patient capable of tolerating surgery and anesthesia. |
| Rehabilitation Goals | Gradual, protected mobilization; acceptance of potential residual deformity. | Early, aggressive rehabilitation aiming for restoration of pre-injury range of motion and strength; minimizing stiffness. |
| Soft Tissue Injury | Intact skin and soft tissues. | Impending skin compromise due to severe angulation. |
| Associated Injuries | Isolated fracture. | Polytrauma, requiring early mobilization of the extremity; associated brachial plexus or axillary nerve lesion (if surgical exploration is also needed). |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for a successful outcome in straight nailing of 2-part surgical neck fractures.
Pre-Operative Assessment
- Clinical Evaluation: A thorough history and physical examination are paramount. Assess neurovascular status, associated injuries, and pre-existing shoulder conditions (e.g., rotator cuff tear, arthritis). Document baseline range of motion and pain.
-
Radiographic Evaluation:
-
Standard Views:
Obtain true AP, lateral (scapular Y), and axillary views of the shoulder. These are crucial for characterizing the fracture pattern, displacement, and angulation.
- CT Scan: A CT scan is highly recommended, especially for complex or highly displaced fractures, or when considering the specific morphology of the surgical neck. It provides detailed information on comminution, articular involvement (to rule out other fracture types), and aids in planning reduction maneuvers and nail trajectory. This can help visualize the impaction and plan for its reduction or retention.
- Contralateral Shoulder X-rays: In cases of severe comminution or uncertainty regarding the normal anatomy, contralateral shoulder imaging can assist in templating nail length and diameter.
-
Standard Views:
Obtain true AP, lateral (scapular Y), and axillary views of the shoulder. These are crucial for characterizing the fracture pattern, displacement, and angulation.
Templating and Implant Selection
-
Nail Length and Diameter:
Determine appropriate nail length and diameter based on pre-operative radiographs and/or CT. The nail should extend to the proximal diaphysis, ideally into the distal third of the humerus, to provide sufficient working length for distal locking. The diameter should be chosen to provide adequate cortical fit without excessive reaming, considering bone quality.
- Templating helps estimate the appropriate nail length to ensure adequate distal locking options while avoiding violation of the elbow joint.
- Estimate the head size to select appropriate proximal locking screw lengths.
- Consider different nail designs regarding curvature and proximal locking options. While "straight" nails are preferred for their ease of insertion and reduced risk of malalignment, variations exist.
- Proximal Locking Configuration: Review the implant system's available proximal locking screw patterns (e.g., number, divergence, angle) to ensure optimal fixation within the humeral head, especially with osteoporotic bone.
- Reduction Tools: Plan for potential reduction aids such as percutaneous K-wires (joysticks), reduction clamps, or blunt elevators, which may be necessary for achieving and maintaining reduction during nail insertion.
Patient Positioning
-
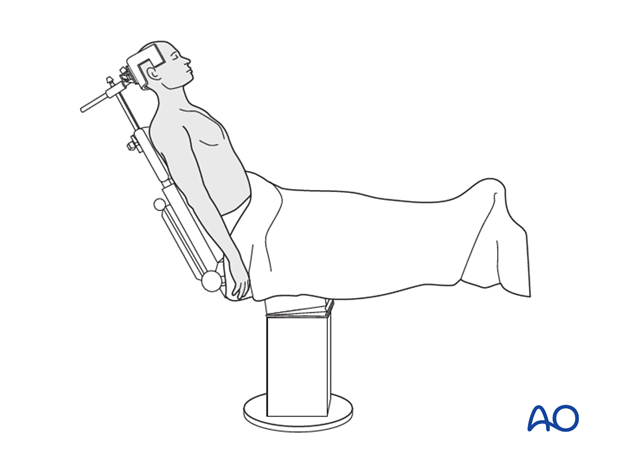
Beach Chair Position:
While some surgeons prefer a supine position on a radiolucent table, the
beach chair position
is commonly favored.
- Advantages: Facilitates ease of access to the shoulder, allows for good fluoroscopic views in multiple planes (AP, lateral, axillary), and provides a comfortable position for the patient and surgical team. It also allows the arm to be manipulated freely for reduction maneuvers.
- Setup: The patient is positioned with the torso elevated 30-70 degrees, supported by a headrest. The affected arm is prepped and draped free, allowing full manipulation.
-
Fluoroscopy:
Ensure optimal C-arm positioning to obtain true AP, lateral, and axillary views without repositioning the patient. Test these views prior to sterile draping.
-
Supine Position:
Can also be used, especially with a traction table to assist with reduction.
- Advantages: May be easier for anesthesia in certain patients, and provides excellent stability for long cases.
- Disadvantages: Can be more challenging for obtaining axillary views and may restrict arm manipulation.
Anesthesia and Prep
- General anesthesia is standard. Regional blocks (e.g., interscalene) can be used for post-operative pain control.
- The limb is prepped from the base of the neck to the hand, ensuring complete sterile field for potential distal locking. The ipsilateral chest and axilla are also included.
- Sterile Draping: The arm is draped free, allowing full range of motion.
Detailed Surgical Approach / Technique
The surgical technique for straight nailing of 2-part surgical neck fractures prioritizes anatomical reduction, appropriate implant placement, and minimal soft tissue disruption.
1. Incision and Approach
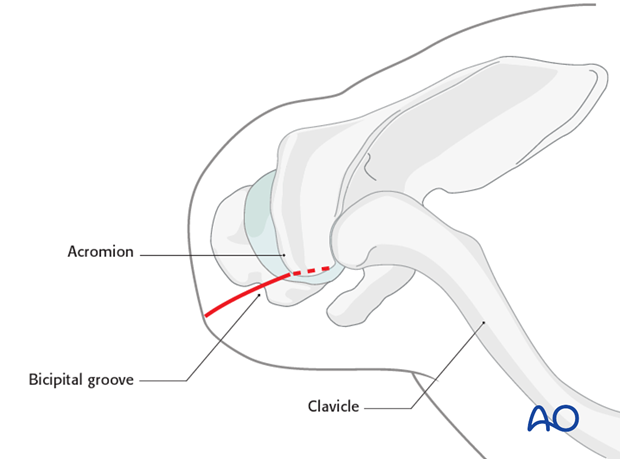
- Skin Incision: A longitudinal skin incision, typically 3-5 cm in length, is made over the anterolateral aspect of the acromion, centered slightly posterior to the acromioclavicular joint, extending distally along the line of the humerus. This allows for direct access to the rotator cuff.
-
Deltoid Split:
The deltoid muscle fibers are then split longitudinally in line with its fibers. The maximum safe length for a deltoid split is generally 5-6 cm distal to the acromion to avoid injury to the axillary nerve, which typically courses approximately 5-7 cm distal to the lateral acromion.
- Deepen the incision through the deltoid fascia, carefully spreading the deltoid fibers.
- Identify the underlying rotator cuff.
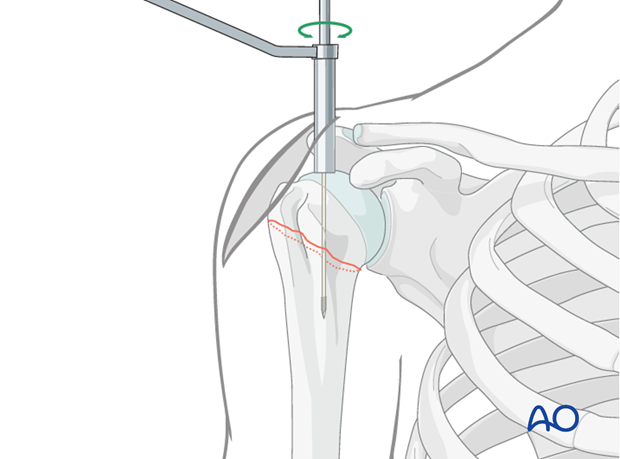
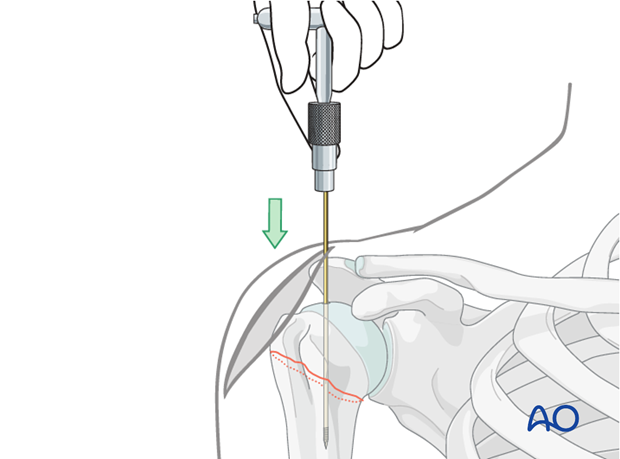
2. Rotator Cuff Entry Point
-
Visualization:
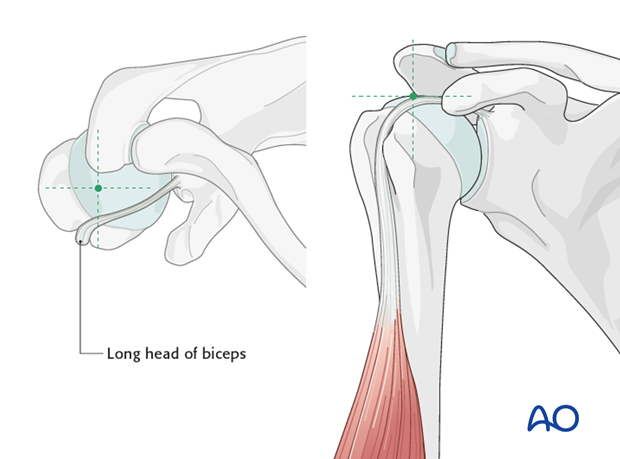
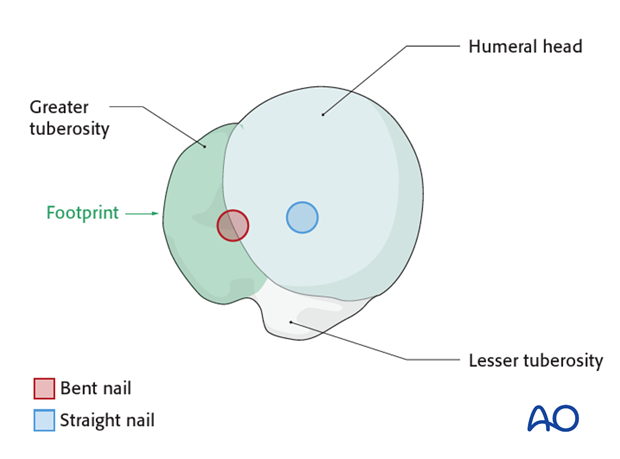
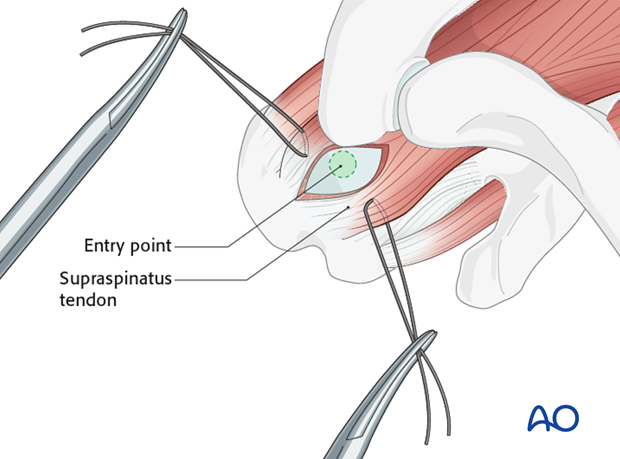
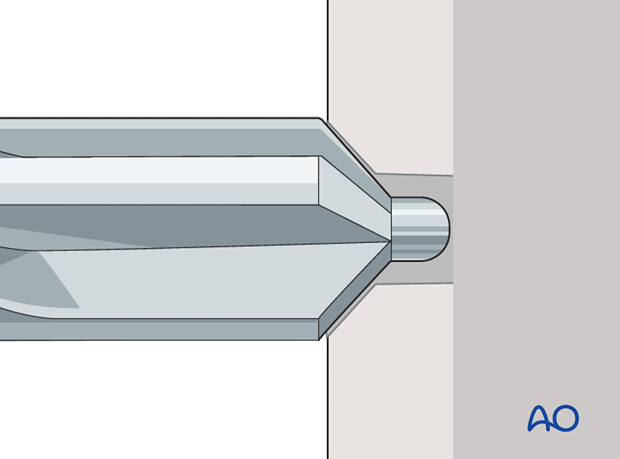
The supraspinatus tendon is identified. The optimal entry point for a straight antegrade humeral nail is typically located just medial to the greater tuberosity, through the supraspinatus tendon, at the apex of the humeral head. This aligns with the medullary canal of the humerus, minimizing varus/valgus malalignment and avoiding compromise of the articular surface.
-
Incision:
A small longitudinal incision (approximately 1-2 cm) is made through the supraspinatus tendon. This tenotomy should be just large enough to allow passage of the guide wire and reamers/nail, minimizing rotator cuff disruption.
- Carefully avoid excessive tendon resection, which can lead to postoperative rotator cuff dysfunction or pain.
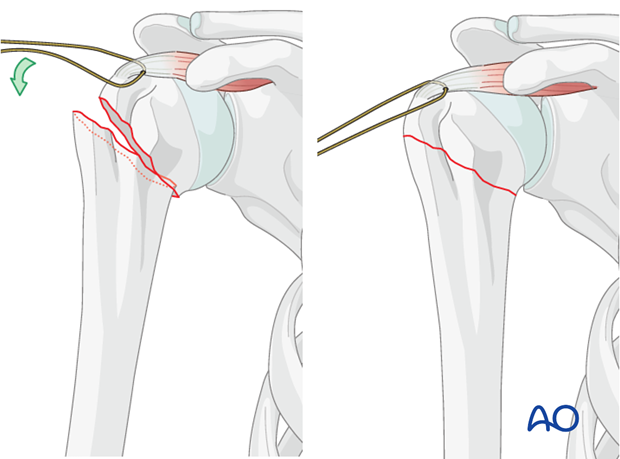
3. Fracture Reduction
-
Assessment:
Once the entry point is exposed, the fracture site is typically not directly visualized but assessed fluoroscopically.
-
Indirect Reduction:
For 2-part surgical neck fractures, indirect reduction techniques are often sufficient.
- Traction and Rotation: Gentle traction, external rotation, and abduction of the arm can help align the humeral head with the shaft.
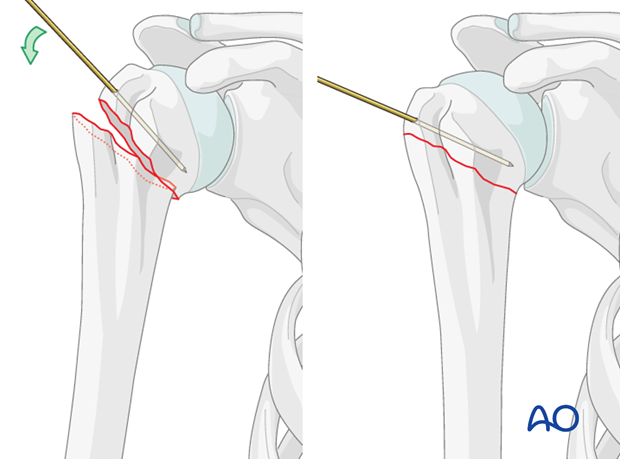
-
Percutaneous Joysticks:
K-wires can be inserted percutaneously into the humeral head and/or the humeral shaft to manipulate fragments under fluoroscopic guidance. This allows for fine adjustments in angulation and rotation.
-
Impaction:
The intrinsically stable impaction often present in these fractures may assist in reduction. If the fracture is significantly impacted in an undesirable alignment, careful disimpaction and reduction may be required.
-
Reduction Clamps/Instruments:
In some cases, a percutaneous reduction clamp may be necessary to stabilize the reduction temporarily.
-
Confirm Reduction:
Obtain true AP and lateral (axillary) fluoroscopic views to confirm anatomical or acceptable alignment before proceeding.
4. Guide Wire Insertion and Medullary Preparation
-
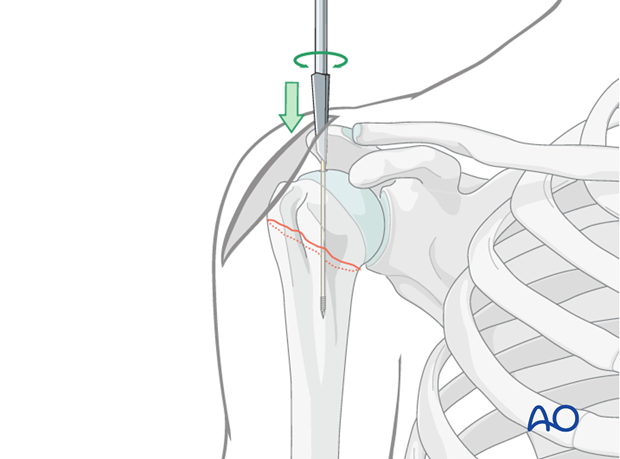
Guide Wire:
A specialized guide wire is advanced through the supraspinatus incision, targeting the medullary canal. Ensure the guide wire is centralized in the humeral head and shaft on both AP and lateral views.
- The guide wire should cross the fracture site and extend distally into the humeral shaft, preferably past the anticipated nail tip position.
-
Correct entry point and guide wire trajectory are crucial for achieving optimal nail placement and avoiding iatrogenic fracture or malreduction.
-
Reaming (Optional):
Many contemporary humeral nails are designed for unreamed insertion. However, if cortical fit is too tight or a larger diameter nail is desired for increased stability in larger canals, reaming may be performed over the guide wire. If reaming, do so incrementally to avoid thermal necrosis and minimize cortical bone loss.
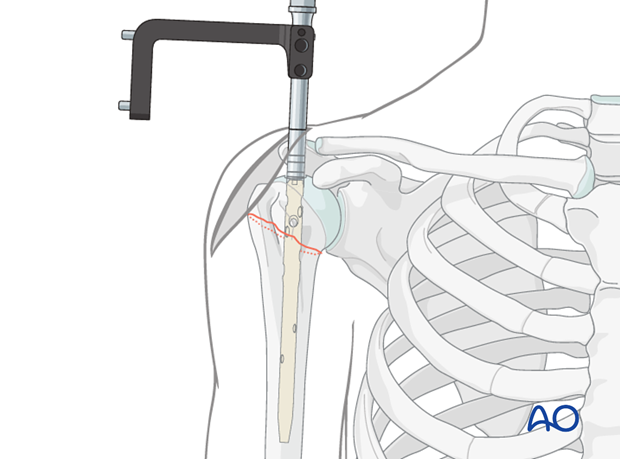
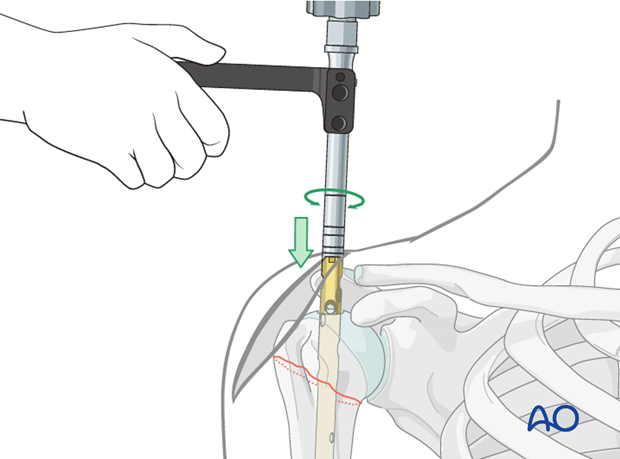
5. Nail Insertion
-
Nail Selection:
Choose the pre-templated straight intramedullary nail.
-
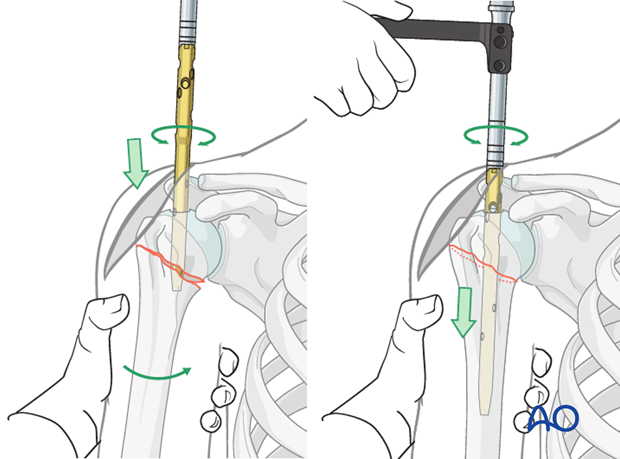
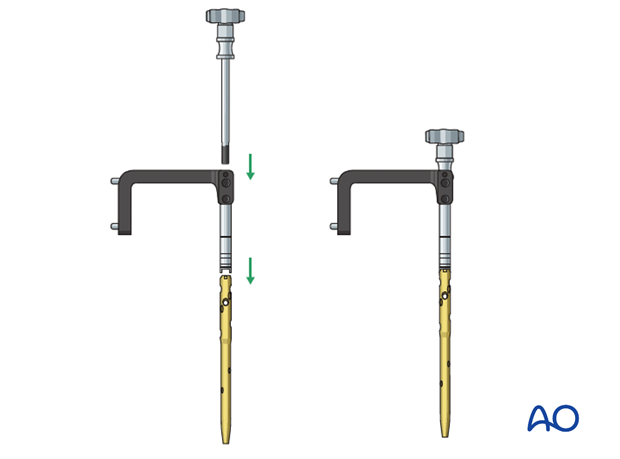
Insertion:
Mount the nail onto its insertion handle. Carefully advance the nail over the guide wire, across the fracture site, and into the distal humeral shaft.
-
Use gentle rotational and impaction forces. Avoid excessive force, which could lead to iatrogenic fracture or loss of reduction.
-
Use gentle rotational and impaction forces. Avoid excessive force, which could lead to iatrogenic fracture or loss of reduction.
-
Positioning:
Advance the nail until its proximal end is flush with, or slightly proud of, the superior aspect of the humeral head, ensuring that the proximal locking holes are optimally positioned for screw placement into the humeral head. Confirm correct length and position fluoroscopically.
6. Proximal Locking
-
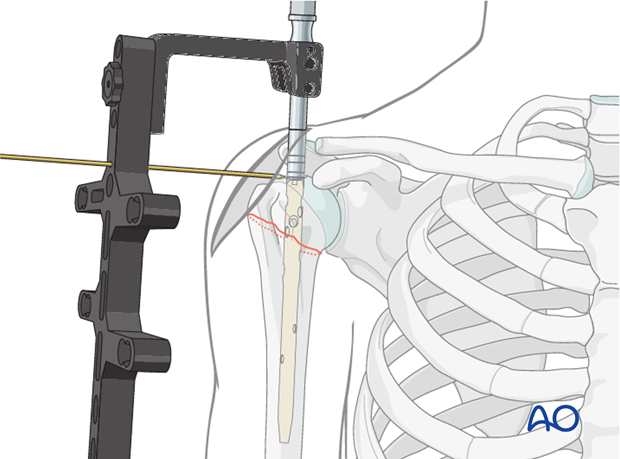
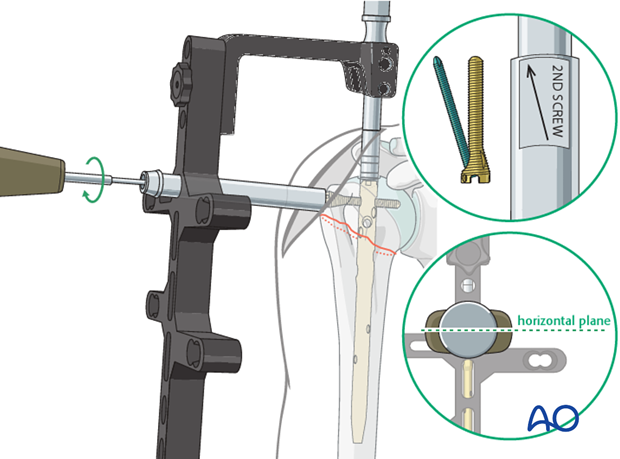
Targeting Jig:
Utilize the specialized targeting jig attached to the insertion handle to guide the placement of proximal locking screws.
-
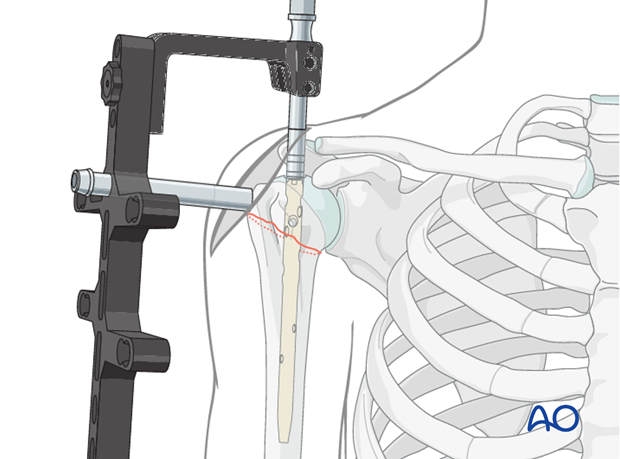
Screw Placement:
Insert guide sleeves and trocars through the skin and deltoid to the bone. Drill holes for the locking screws.
-
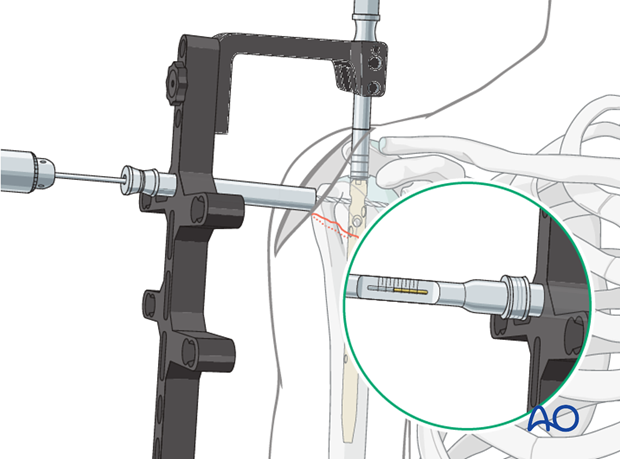
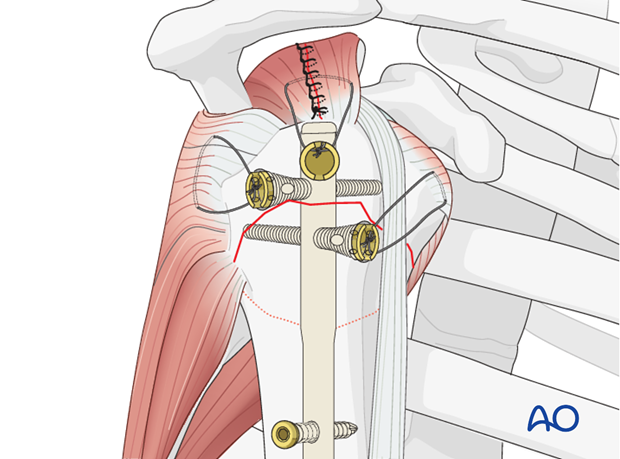
Select appropriate length screws based on fluoroscopic images to ensure bicortical purchase in the humeral head without violating the articular cartilage.
- Typically, 2-3 proximal locking screws are used for optimal stability, especially in osteoporotic bone.
-
Select appropriate length screws based on fluoroscopic images to ensure bicortical purchase in the humeral head without violating the articular cartilage.
- Fluoroscopic Confirmation: Confirm the position and length of all proximal screws in AP and axillary views to ensure they are within the humeral head and not intra-articular.
7. Distal Locking
-
Technique:
Distal locking is usually performed using freehand technique with fluoroscopic guidance or with a distal targeting jig if available for the specific nail system.
-
Fluoroscopy:
Position the C-arm to obtain a perfectly round view of the distal locking holes.
- Make small skin incisions. Drill through the cortex, nail, and opposite cortex.
- Caution: Carefully identify and avoid the radial nerve, which lies in the spiral groove posteriorly, and the brachial artery/median nerve anteriorly. Maintain cortical contact with the drill bit and avoid plunging.
-
Screw Insertion:
Insert appropriate length distal locking screws to achieve bicortical purchase. Typically, 1-2 distal locking screws are sufficient.
-
Final Confirmation:
Obtain final AP and lateral fluoroscopic images of the entire humerus to confirm satisfactory fracture reduction, nail position, and all locking screw placements.
8. Wound Closure
- Remove the insertion handle and guide wire.
- Carefully repair the supraspinatus tenotomy if possible, using absorbable sutures. This minimizes rotator cuff irritation.
- Close the deltoid fascia and subcutaneous tissues in layers.
- Close the skin with appropriate sutures or staples.
- Apply a sterile dressing.
- A sling is typically applied for comfort and protection, though early motion is generally encouraged.
Complications & Management
While straight intramedullary nailing for 2-part surgical neck fractures is generally safe and effective, several complications can arise. Recognition and appropriate management are crucial for optimizing patient outcomes.
Common Complications:
-
Shoulder Pain / Rotator Cuff Impingement (Incidence: 10-30%):
- Cause: Often related to the nail entry point being too proud, rotator cuff tendon damage during insertion, or suture irritation.
-
Management:
- Initial: NSAIDs, physical therapy, subacromial corticosteroid injection.
- Persistent: Consider implant removal (nail and screws) after fracture union. If a specific nail protrusion is identified, surgical revision to re-seat the nail or burr down the nail tip may be necessary. Repair of the rotator cuff defect if symptomatic.
-
Reduction Difficulty / Malunion (Incidence: 5-15%):
- Cause: Failure to achieve or maintain adequate reduction during nail insertion, especially rotational or varus malalignment.
-
Management:
- Intra-operatively: Use additional reduction maneuvers (joysticks, percutaneous clamps), consider temporary K-wire fixation, or resort to a limited open reduction if indirect methods fail.
- Post-operatively: If symptomatic malunion (e.g., impingement, limited ROM) and functional impairment, consider corrective osteotomy or arthroplasty, depending on severity and patient age.
-
Nerve Injury (Axillary or Radial) (Incidence: 1-5%):
-
Cause:
- Axillary nerve: Excessive deltoid splitting (>5-6 cm distal to acromion) or inadvertent damage during proximal dissection.
- Radial nerve: During distal locking, particularly with freehand technique if the drill or screw violates the posterior cortex where the radial nerve lies in the spiral groove.
-
Management:
- Initial: Observation for neuropraxia (most common), nerve conduction studies/EMG if no improvement.
- Persistent deficit: Surgical exploration and neurolysis or repair, depending on the severity of injury.
-
Cause:
-
Nonunion / Delayed Union (Incidence: 2-10%):
- Cause: Inadequate reduction or stability, poor bone quality, excessive soft tissue stripping leading to devascularization, infection, smoking, NSAID use.
-
Management:
- Initial: Protected weight-bearing, bone stimulators.
-
Persistent nonunion (>6-9 months): Revision surgery with exchange nailing, bone grafting (autologous or allograft), or conversion to plate fixation if suitable.
-
Infection (Incidence: <1-2%):
- Cause: Operative contamination.
-
Management:
- Superficial: Oral antibiotics, local wound care.
- Deep: Surgical debridement, intravenous antibiotics, irrigation and débridement, potential hardware removal (after union, or with placement of an antibiotic spacer if non-union).
-
Hardware Failure (Screw back-out, nail protrusion) (Incidence: 2-8%):
- Cause: Poor bone quality, inadequate purchase, premature weight-bearing/mobilization, aggressive rehabilitation.
-
Management:
- Symptomatic hardware: Remove hardware after union.
- Hardware failure leading to loss of reduction or nonunion: Revision surgery with more robust fixation (e.g., larger nail, longer screws, exchange nailing, or conversion to plate/arthroplasty).
-
Avascular Necrosis (AVN) of Humeral Head (Incidence: <1% for 2-part surgical neck):
- Cause: Less common in isolated 2-part surgical neck fractures compared to anatomical neck or 3/4-part fractures, but can result from severe initial displacement or extensive surgical devascularization.
-
Management:
- Initial: Symptomatic management, protected weight-bearing.
- Late stage/collapse: Hemiarthroplasty or total shoulder arthroplasty.
-
Iatrogenic Fracture (Incidence: <1%):
- Cause: Forceful guide wire insertion, over-reaming, forceful nail insertion.
- Management: Intra-operative modification of technique, possible conversion to plate fixation if the iatrogenic fracture compromises nail stability.
Table: Common Complications, Incidence, and Salvage Strategies
| Complication | Estimated Incidence | Salvage Strategies |
|---|---|---|
| Shoulder Pain / Impingement | 10-30% | Conservative (NSAIDs, PT, injections); Hardware removal (after union); Revision to re-seat nail; Rotator cuff repair. |
| Malunion | 5-15% | Conservative for asymptomatic; Corrective osteotomy; Arthroplasty (hemi or total shoulder) for severe symptomatic cases with functional impairment. |
| Axillary Nerve Injury | 1-3% | Observation for neuropraxia; EMG/NCS; Surgical exploration/neurolysis/repair for persistent deficits. |
| Radial Nerve Injury | <1-2% | Observation for neuropraxia; EMG/NCS; Surgical exploration/neurolysis/repair for persistent deficits; Static/dynamic splinting. |
| Nonunion / Delayed Union | 2-10% | Protected weight-bearing, bone stimulators; Revision with exchange nailing; Bone grafting; Conversion to plate fixation or arthroplasty for failed cases. |
| Infection | <1-2% | Superficial: Oral antibiotics. Deep: Surgical debridement, IV antibiotics, irrigation & debridement; Hardware removal (acute: staged with antibiotic spacer; chronic: after union). |
| Hardware Failure | 2-8% | Revision with stronger/longer hardware; Exchange nailing; Bone grafting; Conversion to plate or arthroplasty (depending on fracture union status and bone quality). |
| Avascular Necrosis (AVN) | <1% | Conservative for early stages; Hemiarthroplasty or total shoulder arthroplasty for late-stage collapse and pain. |
| Iatrogenic Fracture | <1% | Intra-operative adjustment of technique; Addition of supplementary fixation (e.g., cerclage wires); Conversion to plate fixation if stability compromised. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is crucial for achieving optimal functional outcomes following straight nailing for 2-part surgical neck fractures. The primary goals are to protect the fracture fixation, restore range of motion, regain strength, and facilitate return to activity. The protocol should be tailored to individual patient factors, bone quality, and intra-operative stability.
Phase 1: Immobilization and Passive Range of Motion (Weeks 0-4/6)
- Protection: The arm is typically immobilized in a sling for comfort and protection for the initial 4-6 weeks. However, the sling should be removed for exercises.
- Goals: Minimize pain and swelling, prevent shoulder stiffness, protect healing soft tissues.
-
Exercises:
- Pendulum Exercises: Gentle, gravity-assisted oscillations of the arm.
-
Passive Range of Motion (PROM):
Initiated early, typically within the first week, by a physical therapist or with assistance.
- Forward flexion: Up to 90 degrees.
- External rotation: Up to 30-45 degrees (neutral position).
- Internal rotation: To chest.
- Scapular Mobilization: Gentle scapular retraction and protraction exercises.
- Elbow, Wrist, Hand Exercises: Full active range of motion to prevent stiffness in these joints.
- Weight-Bearing Restrictions: No active lifting, pushing, or pulling with the affected arm. No weight-bearing through the hand/arm.
- Activities of Daily Living (ADLs): Encourage use of the unaffected arm for personal care. Educate on proper sling use and hygiene.
Phase 2: Assisted and Active Range of Motion (Weeks 4/6 - 12)
- Progression: As pain subsides and radiographic signs of early healing appear (typically around 6 weeks), progression to active-assisted and then active range of motion is initiated.
- Goals: Gradually increase shoulder range of motion, initiate light strengthening.
-
Exercises:
- Active-Assisted Range of Motion (AAROM): Using the contralateral hand or a stick to assist the affected arm in flexion, abduction, and rotation.
- Active Range of Motion (AROM): Gradually progressing to full unassisted range of motion.
- Isometrics: Gentle isometric strengthening of the rotator cuff (subscapularis, infraspinatus, supraspinatus) and deltoid, with the arm in neutral positions.
- Scapular Stabilization: Exercises to strengthen scapular retractors and protractors.
- Weight-Bearing Restrictions: Continue to avoid heavy lifting. Light resistance (e.g., 1-2 lbs) may be introduced for specific exercises, under therapist guidance.
- Functional Activities: Begin incorporating light, pain-free ADLs using the affected arm.
Phase 3: Strengthening and Advanced Functional Training (Weeks 12 - 24+)
- Progression: Commences once full pain-free active range of motion is achieved and radiographic union is evident.
- Goals: Restore full strength, endurance, and proprioception; prepare for return to desired activities.
-
Exercises:
- Progressive Resistance Exercises (PREs): Using elastic bands, light dumbbells, and machines for rotator cuff, deltoid, and periscapular muscles.
- Proprioceptive Exercises: Wall push-ups, ball throws against a wall, progressing to dynamic activities.
-
Sport-Specific or Activity-Specific Training:
Tailored exercises to meet the patient's occupational or recreational demands.
 `
`
- Return to Activity: Gradual return to light activities (e.g., swimming) typically between 4-6 months, with full unrestricted activity (e.g., contact sports, heavy lifting) often requiring 6-12 months, depending on fracture consolidation and individual progress.
- Hardware Removal: If hardware-related pain or impingement persists after union (typically 12-18 months post-op), hardware removal may be considered.
Throughout all phases, pain management and patient education are integral. Close communication between the surgeon, physical therapist, and patient is essential to ensure appropriate progression and address any concerns or complications.
Summary of Key Literature / Guidelines
The existing literature regarding the optimal management of 2-part surgical neck fractures, particularly with intramedullary nailing, highlights a nuanced approach based on fracture stability, patient factors, and evolving implant technology.
-
Non-Operative vs. Operative Management:
- For stable, minimally displaced or well-impacted 2-part surgical neck fractures, non-operative management with early gentle mobilization often yields good functional outcomes, especially in elderly, low-demand patients. Studies by Court-Brown et al. and others emphasize that acceptable alignment can vary with age and activity level. The original seed content notes "Mild-moderate angulation is well tolerated. Significant deformity may require reduction and fixation." This aligns with the evidence supporting non-operative treatment for many of these inherently stable fractures.
- Operative intervention, including intramedullary nailing, is typically reserved for cases with unacceptable deformity (e.g., >30 degrees angulation, >1 cm translation or shortening), instability, or in active patients where superior anatomical alignment and earlier rehabilitation are desired.
-
Intramedullary Nailing vs. Plate Fixation:
- Biomechanical Advantages of Nailing: Intramedullary nails offer central load-sharing, which theoretically reduces stress risers at the bone-implant interface, a particular advantage in osteoporotic bone. Studies by several groups have shown that IM nails can provide comparable or superior torsional and bending stiffness compared to plates in biomechanical models, especially for metaphyseal fractures.
-
Clinical Outcomes:
Clinical outcomes between nailing and plating for proximal humerus fractures are often debated. For 2-part surgical neck fractures, nailing offers several advantages:
- Minimally Invasive: Smaller incision, less soft tissue stripping, potentially preserving periosteal blood supply to the fracture fragments. This reduces surgical trauma and may lead to faster healing and lower infection rates compared to extensive open plating approaches.
- Rotator Cuff Entry: The trans-tendon entry (supraspinatus) is a known concern for postoperative pain and rotator cuff disturbance, as noted in the original seed content's disadvantages. However, modern nail designs and careful surgical technique aim to minimize this. Some studies report a higher incidence of shoulder pain post-nailing compared to plating, but functional outcomes are often comparable.
- Disadvantages: Reduction can be technically more challenging with closed nailing compared to open plating. The risk of axillary nerve damage, while low, must be considered.
- Specific Evidence for 2-Part Surgical Neck: While much of the literature on proximal humerus nailing encompasses a broader range of fracture types (including 3- and 4-part), studies focusing on 2-part surgical neck fractures generally report favorable union rates (85-95%) and acceptable functional outcomes with intramedullary nailing, particularly when strict indications are followed.
-
Technical Considerations:
- Entry Point: The importance of a proper entry point (just medial to the greater tuberosity, in line with the humeral shaft) is consistently emphasized in the literature to prevent impingement, varus malalignment, and iatrogenic articular damage.
- Reduction: The effectiveness of indirect reduction techniques, often utilizing percutaneous K-wires or joysticks, is highlighted. Avoiding extensive open reduction helps preserve vascularity and soft tissue integrity.
- Nail Design: The development of "straight" nails with multiple, divergent proximal locking screws has improved stability in the cancellous humeral head, addressing concerns about pull-out in osteoporotic bone.
- Rehabilitation: Early, controlled passive and active-assisted range of motion is advocated in most rehabilitation protocols for surgically treated proximal humerus fractures, aiming to prevent stiffness while protecting fixation. Progression is guided by pain, radiographic healing, and stability of fixation.
In summary, current guidelines support intramedullary nailing as a viable and often preferred option for appropriately selected 2-part surgical neck fractures, particularly those that are displaced or unstable, in patients amenable to surgical intervention. The technique offers biomechanical advantages and a less invasive approach compared to plating, though careful attention to surgical detail and patient selection is paramount to mitigate potential complications. The evolving understanding of fracture biology, biomechanics, and refined surgical techniques continues to shape the optimal approach for these common injuries.
Clinical & Radiographic Imaging
You Might Also Like