Unlock Perfect Reduction: Key Techniques in Fracture Management
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Unlock Perfect Reduction: Key Techniques in Fracture Management. Techniques in fracture reduction commonly involve closed methods, starting with traction along the limb's line to disimpact fragments and correct shortening. Any residual angulation is then addressed with localized hand pressure. In challenging cases, initial increased angulation may help unlock fragments. Post-reduction, stabilization is critical using methods like plaster fixation, various traction types, cast bracing, or external fixation to prevent redisplacement.
Unlock Perfect Reduction: Key Techniques in Fracture Management
Introduction & Epidemiology
Achieving anatomical reduction is a cornerstone of fracture management, directly correlating with favorable functional outcomes, minimized pain, and reduced incidence of post-traumatic complications. "Perfect reduction" in orthopedic trauma signifies the restoration of length, alignment, rotation, and joint congruity to as near anatomical as possible, within the limits of biological healing and patient physiology. This objective is particularly critical for intra-articular fractures where even minor incongruity can lead to accelerated degenerative changes and persistent dysfunction.
Fractures are a ubiquitous burden on global healthcare systems. Their epidemiology varies widely based on age, mechanism of injury, and geographic location. While distal radius fractures are common in osteoporotic populations, diaphyseal fractures are more prevalent in younger, high-energy trauma cohorts. Regardless of the specific fracture type or patient demographic, the principles of reduction remain paramount. The goal is to facilitate optimal biological healing and reconstruct the skeletal architecture to withstand physiological loads, thereby returning patients to their pre-injury functional status, or the best possible outcome given the injury severity. The decision between closed and open reduction, and the subsequent choice of fixation, is a complex process guided by fracture characteristics, patient factors, and surgical expertise, all centered around achieving and maintaining an optimal reduction.
Surgical Anatomy & Biomechanics
A thorough understanding of regional surgical anatomy and the biomechanical forces influencing fracture patterns is indispensable for effective reduction. The specific anatomical location (e.g., long bone diaphysis, metaphysis, epiphysis, articular surface) dictates the inherent stability of a fracture and its propensity for displacement.
- Muscle Forces: Muscular attachments exert significant deforming forces on fracture fragments, leading to characteristic displacements. For instance, in a subtrochanteric femoral fracture, the iliopsoas typically causes flexion and external rotation of the proximal fragment, while the abductors pull it into abduction. In contrast, distal radius fractures often displace dorsally and radially due to muscle and ligamentous pull. Understanding these forces is critical for applying counter-forces during reduction.
- Ligamentotaxis: This principle is particularly relevant for articular fractures, such as those of the calcaneus, distal radius, or pilon. Intact ligaments spanning a fracture can be tensioned through traction, thereby indirectly reducing articular fragments. This technique leverages the capsuloligamentous attachments to guide fragments back into position, often obviating the need for extensive soft tissue dissection.
- Periosteal Hinge: In many closed fractures, an intact periosteal sleeve on one side of the bone can act as a hinge, facilitating reduction by providing a stable pivot point. This hinge must be protected during reduction maneuvers, as its disruption can convert a relatively simple reduction into a more complex one with increased instability.
- Fracture Personality: Each fracture possesses a unique "personality" defined by its morphology (transverse, oblique, spiral, comminuted, segmental), location, and degree of displacement. Simple, stable fracture patterns may be amenable to closed reduction and cast immobilization, while complex, highly comminuted, or intra-articular fractures often necessitate open reduction and internal fixation to restore anatomy and achieve stability.
- Bone Quality: The biomechanical properties of the bone itself significantly influence reduction strategies. Osteoporotic bone is prone to comminution and may not hold fixation well, requiring specific implant designs and reduction techniques that minimize stress risers. Conversely, dense cortical bone in younger patients may present challenges in manipulating fragments without specialized tools.
Indications & Contraindications
The decision to pursue operative versus non-operative management, and subsequently the choice of reduction technique, hinges on a careful assessment of the fracture pattern, patient factors, and functional goals.
Indications for Reduction
-
Closed Reduction:
- Fractures with unacceptable alignment, length, or rotation that can be corrected manually without surgical exposure.
- Fractures amenable to immobilization after reduction (e.g., cast, splint, functional brace).
- Emergent stabilization of displaced fractures (e.g., prior to definitive fixation, temporary neurovascular decompression).
- Fractures where anatomical reduction is not strictly necessary for good function (e.g., certain clavicle fractures, some fibula fractures).
-
Open Reduction:
- Irreducible fractures: Fractures that cannot be adequately reduced by closed methods due to soft tissue interposition (e.g., muscle, tendon, periosteum), severe displacement, or bone-on-bone impingement.
- Intra-articular fractures: Displaced fractures involving articular surfaces where anatomical restoration of joint congruity is critical to prevent post-traumatic arthritis.
- Open fractures: Require débridement and irrigation, and often necessitate open reduction for stable fixation.
- Neurovascular compromise: Fractures causing or threatening neurovascular structures that require immediate surgical exploration and reduction.
- Polytrauma patients: Often benefit from early definitive stabilization to facilitate rehabilitation and prevent complications of prolonged immobilization.
- Pathologic fractures: May require open reduction for tumor resection and stabilization.
- Unstable fractures: Fractures that are inherently unstable and cannot be maintained in an acceptable position with closed methods alone.
Contraindications for Reduction
-
Non-operative Management:
- Fractures with acceptable alignment, length, and rotation that are inherently stable.
- Minimally displaced fractures in anatomical regions where small residual displacement is functionally inconsequential (e.g., some toe fractures, stable rib fractures).
- Medically unstable patients for whom anesthesia and surgery pose excessive risk.
- Patients with limited functional demands or significant comorbidities where aggressive intervention may outweigh potential benefits.
-
Relative Contraindications for Open Reduction:
- Severe soft tissue compromise, active infection (though open fractures require débridement), or profound medical instability.
- Extensive comminution making anatomical reduction impossible or detrimental due to excessive soft tissue stripping.
Operative vs. Non-Operative Indications
| Feature | Operative Reduction (ORIF/CRIF) | Non-Operative Reduction (Closed Reduction & Immobilization) |
|---|---|---|
| Fracture Displacement | Unacceptable displacement (angulation, shortening, rotation) | Acceptable displacement, or reducible to acceptable limits by closed means |
| Fracture Type | Intra-articular, unstable, open fractures, segmental, highly comminuted, irreducible fractures | Stable, minimally displaced, some extra-articular fractures (e.g., clavicle, stable olecranon) |
| Associated Injuries | Neurovascular compromise, compartment syndrome, significant soft tissue injury requiring exploration | No neurovascular compromise, intact soft tissue envelope (except open fractures requiring debridement) |
| Patient Factors | Polytrauma, active patient requiring early mobilization, inability to maintain reduction without fixation | Medically unstable, low functional demands, compliant patient, suitable for prolonged immobilization |
| Fracture Location | Articular surfaces, certain metadiaphyseal regions prone to instability (e.g., proximal tibia) | Diaphyseal fractures with inherent stability, periarticular fractures with minimal displacement |
| Failure of Closed Reduction | Yes | N/A |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is paramount for achieving and maintaining perfect reduction.
Pre-Operative Planning
- Clinical Assessment: Thorough history and physical examination, including neurovascular status.
-
Imaging:
- Plain Radiographs: At least two orthogonal views are essential. Consider views of joints above and below, and contralateral limb for templating.
- Computed Tomography (CT): Crucial for complex periarticular and intra-articular fractures to delineate comminution, fragment orientation, and articular step-off/gap. 3D reconstructions can be invaluable.
- Magnetic Resonance Imaging (MRI): Indicated for suspected ligamentous injury, meniscal tears, or occult soft tissue trauma influencing stability or reduction.
- Templating: Utilize radiographs or digital images to pre-select appropriate implants (plates, screws, nails, external fixators) and plan their placement. This allows for anticipation of reduction challenges and equipment needs.
- Anesthesia Considerations: Adequate anesthesia (regional, general, or a combination) is crucial for muscle relaxation, which is often the primary obstacle to closed reduction.
- Tourniquet Management: Plan for tourniquet use if appropriate to optimize visualization and minimize blood loss. Discuss duration and potential complications.
- Surgical Approach Selection: Based on fracture pattern and location, choose an approach that provides optimal visualization for reduction while minimizing soft tissue disruption (e.g., extensile approach for complex intra-articular fractures vs. limited approach for percutaneous plating).
Patient Positioning
Proper patient positioning is critical for both exposure and facilitation of reduction maneuvers.
*
Access:
Ensure unimpeded access to the surgical site and the ability to maneuver instruments and C-arm fluoroscopy.
*
Stability:
The patient must be stable on the operating table, often secured with bolsters, beanbags, or traction tables.
*
C-arm Fluoroscopy:
Position the C-arm for optimal orthogonal views without repositioning the patient. For long bone fractures, ensure adequate range of motion to visualize the entire bone and adjacent joints. For intra-articular fractures, multiple oblique views may be necessary.
*
Traction Tables:
Specialized traction tables (e.g., for femur fractures, ankle fractures) provide sustained axial traction, which is invaluable for reducing shortening and distracting fragments, facilitating ligamentotaxis. This is particularly relevant for proximal femur fractures and ankle fractures.
*
Upper Extremity Positioning:
For upper extremity fractures, supine positioning with the arm on a hand table, or prone/beach chair for shoulder/humerus, allows for various degrees of rotation and flexion/extension.
Detailed Surgical Approach / Technique
Principles of Closed Reduction
Closed reduction aims to restore anatomical alignment without direct surgical exposure of the fracture site. This relies heavily on understanding the deforming forces and applying inverse maneuvers.

The initial step involves assessing the
direction and magnitude of the causal force (1)
and the resulting
deformity (2)
. This can be deduced from the injury mechanism, clinical appearance, and radiographic assessment. To correct the displacement,
force is applied in the opposite direction (3)
to reverse the injury mechanism. This often involves a sequential approach: disimpaction, reduction of shortening, correction of angulation, and finally, rotation.

Basic techniques (b):
The application of
traction (1)
is usually the primary step in most closed reductions. Traction, typically applied in the long axis of the limb, overcomes muscle spasm and disimpacts fragments. This
disimpaction (2)
may occur almost immediately, especially in a relaxed patient under adequate anesthesia. Continuous traction also leads to the
reduction of shortening (3)
and, in many cases, will significantly correct the gross
deformity (4)
.

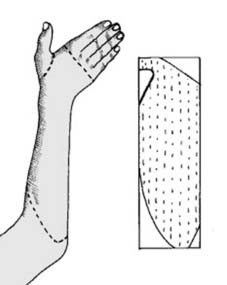
Basic techniques (c):
Following initial traction, any residual angulation can be corrected through direct manipulation. This often involves using the
heel of one hand as a fulcrum (1)
under the apex of the deformity, while applying
distal pressure with the other hand (2)
to complete the reduction. This maneuver leverages the intact periosteal hinge if present.
Additional critical principles for closed reduction:
*
Counter-traction:
Essential to effectively apply traction. This can be achieved through an assistant, specialized traction devices, or the operating table.
*
Circumduction/Rotation:
May be necessary to unlock fragments, especially in spiral or oblique fractures, before applying axial traction.
*
Direct Manual Pressure:
Once length and alignment are restored, direct pressure over the fracture fragments can correct minor remaining displacement.
*
Fluoroscopic Guidance:
Continuous or intermittent fluoroscopy is indispensable to monitor reduction progress and confirm final alignment in multiple planes.
Advanced Closed and Indirect Reduction Techniques
When direct manual pressure is insufficient or undesirable, advanced closed and indirect techniques can be employed.
-
Ligamentotaxis with External Fixation: For certain intra-articular fractures (e.g., distal radius, pilon), external fixators can be used to apply continuous traction, leveraging the intact ligamentous structures to pull articular fragments back into position. This is a powerful indirect reduction method.
-

-

-

-

-

These images likely illustrate different phases or applications of external fixation for reduction, perhaps showing pins inserted, the frame being applied, and the resulting distraction or compression to achieve fragment alignment. For instance, images gr22, gr18, gr25 might sequentially demonstrate external fixator application and initial reduction efforts for a distal radius or tibial pilon fracture, leveraging ligamentotaxis. Image gr13 could show a specific type of clamp or distractor used in conjunction with pins, while gr20 might show fluoroscopic confirmation of reduction.
-
-
Percutaneous K-wire Manipulation ("Joystick" Technique): K-wires can be inserted into fracture fragments and used as "joysticks" to manipulate them into desired positions under fluoroscopic guidance. This is a minimally invasive technique that minimizes soft tissue stripping.
-

-
These images probably depict the K-wire joystick technique. gr8 might show the insertion of a K-wire into a fragment, and gr15 could illustrate the manipulation of that K-wire to achieve reduction, often seen in metaphyseal or articular fragments.
-
-
Large Distractors: For complex long bone fractures, large external distractors can be applied across the fracture site to restore length and correct gross angulation before definitive fixation. This is particularly useful in comminuted diaphyseal fractures.
-

This image could show the application of a large distractor across a long bone fracture, illustrating how it creates tension to restore length, setting the stage for subsequent reduction and fixation.
-
-
Traction Tables: As mentioned, these are essential for sustained traction, especially in lower extremity fractures like femoral shaft or acetabular fractures, allowing the surgeon to free their hands for other maneuvers.
-

This image might show a patient positioned on a traction table, highlighting the boots or slings used to apply traction and counter-traction, aiding in initial reduction.
-
Open Reduction Techniques
Open reduction involves direct visualization of the fracture fragments, allowing for precise anatomical restoration. While it offers superior control, it carries the inherent risk of increased soft tissue dissection and potential devascularization.
General Principles of Open Reduction:
- Surgical Approach: Select an approach that provides adequate exposure with minimal damage to critical neurovascular structures and muscle attachments. Respect internervous planes whenever possible.
- Hematoma Evacuation: Remove hematoma and small, non-viable bone fragments to improve visualization and prevent interposition.
- Soft Tissue Protection: Minimize stripping of periosteum and attached muscle, especially around comminuted fragments, to preserve vascularity. The concept of "biological fixation" emphasizes this.
-
Sequential Reduction:
- Restore Length: Often the first step. This may involve traction (manual or mechanical) or the use of reduction clamps.
- Reduce Key Fragments: Identify and reduce the most stable fragments first, often using a "puzzle piece" approach for comminuted fractures. Intra-articular fragments are typically reduced first to establish joint congruity.
- Restore Rotational and Angulatory Alignment: Use anatomical landmarks (e.g., epicondyles, malleoli, cortical step-offs) and fluoroscopy to ensure correct rotation and angulation.
- Lag Screw Principle: For oblique or spiral fractures, a lag screw across the fracture line can compress fragments, enhancing stability and reduction.
Specific Reduction Tools & Maneuvers:
-
Reduction Clamps:
-
Pointed Reduction Forceps:
Used to grasp and manipulate individual fragments, compressing them across the fracture line.
-

-

These images likely demonstrate pointed reduction forceps in action. gr23 might show initial placement and grasping of fragments, while gr10 could illustrate the application of compression to achieve reduction.
-
- Periosteal Elevators/Hohmann Retractors: Can be used as levers or fulcrums to manipulate larger fragments.
-
Bone Hooks:
Useful for pulling or pushing fragments into position, especially in areas with limited access.
-

This image could show a bone hook engaging a fragment, illustrating its use in direct manipulation.
-
-
Pointed Reduction Forceps:
Used to grasp and manipulate individual fragments, compressing them across the fracture line.
-
Temporary K-wire Fixation: After achieving reduction of key fragments, K-wires are invaluable for temporary stabilization to hold the reduction while definitive fixation is applied.
-

-

Images gr26 and gr19 might illustrate the use of K-wires for temporary fixation, securing a reduced fragment or holding a reduction while a plate is contoured and applied.
-
-
Plate as a Reduction Tool: Pre-contoured anatomical plates can sometimes be used as a "template" or "reduction aid," applying pressure or tension to fragments as screws are inserted, thereby reducing them to the plate's contour. This is particularly useful for metaphyseal or periarticular fractures.
-

-

These images could show a plate being used as a reduction guide. gr21 might show the initial placement of a plate over displaced fragments, and gr14 could illustrate how tightening screws draws the bone fragments towards the pre-contoured plate, achieving reduction.
-
-
Intramedullary Nailing: For long bone diaphyseal fractures, intramedullary nailing relies on reaming and nail insertion to achieve and maintain reduction. While primarily a fixation technique, the nail itself acts as an internal splint to align fragments. Reduction maneuvers (e.g., traction, piriformis entry point, blocking screws) are often required prior to or during nail insertion.
-

-

-

-

These images likely pertain to intramedullary nailing for long bone fractures. gr4 might depict a guide wire being inserted, gr24 showing reaming, gr7 illustrating the nail insertion, and gr27 possibly demonstrating locking screw placement to stabilize the achieved reduction. The reduction component here is often indirect, achieved through traction and the centering effect of the reamers and nail.
-
-
Minimally Invasive Plate Osteosynthesis (MIPO): This technique involves limited surgical exposure for plate insertion, with reduction primarily achieved indirectly using external traction, manipulators, or percutaneous clamps. The plate acts as a "biological splint," preserving soft tissue envelope.
-

This image could show the use of a specialized percutaneous clamp or reduction tool employed during MIPO to manipulate fragments into alignment before plate fixation.
-
Final Reduction Assessment:
After presumed reduction, thoroughly assess alignment (length, rotation, angulation) using:
*
Fluoroscopy:
Multiple views (AP, lateral, obliques) are mandatory. Compare to contralateral side if needed.
*
Clinical Assessment:
Palpate anatomical landmarks, check limb lengths, and assess rotational alignment (e.g., patella-to-toe alignment, forearm pronation/supination).
*
Arthroscopy:
For certain intra-articular fractures (e.g., tibial plateau, pilon), arthroscopy can provide direct visualization of articular reduction and guide fragment fixation.
Complications & Management
Despite meticulous technique, complications can arise during or after fracture reduction and fixation. Awareness and prompt management are crucial.
| Complication | Incidence (General) | Salvage Strategies / Management |
|---|---|---|
| Malunion | Varies by fracture type (5-20%) | Mild: No intervention if asymptomatic. Moderate-Severe: Corrective osteotomy and refixation once healed. Revision surgery to restore anatomy. |
| Nonunion | Varies by fracture type (1-10%) | Revision surgery with débridement of nonunion site, biological augmentation (bone graft, bone graft substitutes), and rigid internal fixation. May require different implant or technique. |
| Infection | <1% (closed); 2-15% (open) | Surgical débridement, irrigation, antibiotics (IV then oral), negative pressure wound therapy. May require staged procedures, implant removal, or bone transport. |
| Neurovascular Injury | <1% (iatrogenic during reduction) | Immediate exploration. Primary repair if possible. Grafting if significant defect. Referral to vascular/neurosurgery as appropriate. Prevention: careful dissection, identification of structures, gentle manipulation. |
| Compartment Syndrome | Rare (iatrogenic); 2-9% (post-trauma) | Immediate fasciotomy. If caused by tight cast/dressing post-reduction, remove immediately. Prevention: vigilant monitoring, avoiding overly tight dressings. |
| Post-traumatic Arthritis | Varies (common in intra-articular fractures) | Early: Physiotherapy, NSAIDs, intra-articular injections. Late: Joint replacement (arthroplasty), arthrodesis, osteotomy, or revision surgery to correct residual incongruity. |
| Implant Failure | <5% | Revision fixation (stronger implant, different construct), often with bone grafting if nonunion is present. Address underlying cause (e.g., poor reduction, infection, premature weight-bearing). |
| Stiffness / Loss of Motion | Common, varies by joint | Intensive physiotherapy, static/dynamic splinting. Surgical release (arthrolysis) for severe cases after fracture healing. Prevention: early, controlled mobilization. |
| Pain (Chronic) | Common | Multimodal pain management, physiotherapy, psychological support. May require hardware removal if symptomatic, or specific nerve blocks/denervation for neuropathic pain. |
| Skin / Soft Tissue Necrosis | Varies by approach | Local wound care, débridement, negative pressure wound therapy. May require plastic surgery consultation for flaps or grafts. Prevention: careful handling of soft tissues, minimizing tension. |
-

-

These images might represent illustrative examples of complications or their management. Gr16 could show a radiograph depicting a malunion, while gr12 might show an implant failure or a case requiring revision fixation, emphasizing the importance of accurate reduction and stable fixation to prevent these outcomes.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is an integral component of fracture management, directly impacting functional recovery following reduction and fixation. The protocol is individualized based on fracture stability, fixation strength, patient comorbidities, and functional goals.
General Principles:
- Pain and Swelling Management: Aggressive use of analgesia, elevation, ice, and compression to control pain and edema, which can hinder early rehabilitation.
-
Early Mobilization (as appropriate):
- Joints not immobilized: Commence immediate, active range of motion (ROM) to prevent stiffness.
- Fracture site: Depending on stability, controlled, protected ROM can begin early. This is critical for preventing stiffness, promoting cartilage health (in intra-articular fractures), and preventing muscle atrophy.
- Weight-Bearing Status: Strictly follow the surgeon's prescription (non-weight bearing, touch-down weight bearing, partial weight bearing, weight bearing as tolerated). This depends on the fracture pattern, fixation stability, and bone healing progression.
- Strengthening: Gradually introduce strengthening exercises as pain subsides and healing progresses. Focus on muscles proximal and distal to the fracture, and eventually the entire limb.
- Proprioception and Balance: Essential, especially for lower extremity and intra-articular fractures, to restore neuromuscular control and prevent re-injury.
- Functional Activities: Progress from basic movements to activities of daily living, and ultimately to sport- or work-specific activities.
- Monitoring: Regular clinical and radiographic follow-up to assess healing, monitor for complications (e.g., malunion, nonunion), and adjust rehabilitation protocols.
Specific Considerations:
- Upper Extremity: Early ROM for shoulder, elbow, wrist, and hand often commences as soon as fixation allows, to prevent contractures, particularly in the elbow and wrist.
- Lower Extremity: Emphasis on protected weight-bearing, gait training, and restoring balance and proprioception.
- Intra-articular Fractures: Critical to achieve early, controlled, pain-free ROM to promote cartilage healing and prevent arthrofibrosis and post-traumatic arthritis. Continuous passive motion (CPM) may be used for specific joints.
Summary of Key Literature / Guidelines
The principles guiding fracture reduction and fixation have evolved significantly, largely influenced by the contributions of the AO Foundation (Arbeitsgemeinschaft für Osteosynthesefragen) and other international bodies.
-
AO Principles of Fracture Management:
- Anatomical Reduction: Essential, especially for intra-articular fractures. For diaphyseal fractures, anatomical alignment of length, axis, and rotation is prioritized, with less emphasis on perfect anatomical reduction of every fragment if stability can be achieved otherwise.
- Stable Fixation: To provide absolute stability (e.g., lag screws for articular fragments) or relative stability (e.g., intramedullary nails, bridging plates for comminuted fractures) appropriate for the fracture pattern and biological environment.
- Preservation of Blood Supply: Meticulous surgical technique to minimize soft tissue stripping, protecting the periosteum and surrounding musculature to preserve the biological environment for healing. This underpins approaches like MIPO.
- Early, Safe Mobilization: Allows functional recovery and prevents complications associated with prolonged immobilization.
-
Timing of Intervention:
- Emergent: Open fractures, neurovascular compromise, compartment syndrome.
- Urgent (within 24 hours): Unstable pelvic ring injuries, grossly displaced fractures requiring pain control/skin protection.
- Early Definitive (within 3-5 days): Most other fractures after initial workup and optimization, especially in polytrauma settings to shorten ICU stay and reduce complications.
-
Role of Imaging: High-resolution CT scans with 3D reconstructions have become indispensable for pre-operative planning of complex articular and periarticular fractures, significantly improving the ability to anticipate and execute precise reduction maneuvers.
-
Biological Fixation vs. Absolute Fixation:
- Absolute stability: Achieved with interfragmentary compression (lag screws, tension band wiring) suitable for simple fracture patterns (transverse, short oblique, spiral) to allow primary bone healing. Requires anatomical reduction.
- Relative stability: Achieved with bridging plates, intramedullary nails, or external fixators, allowing for controlled motion at the fracture site leading to secondary bone healing (callus formation). Used for comminuted fractures where anatomical reduction of every fragment is impossible or biologically detrimental. Acceptable malalignment is sometimes tolerated to preserve soft tissue.
-
Evidence-Based Guidelines: Various national and international societies publish guidelines for specific fracture types (e.g., distal radius, hip fractures, ankle fractures), often incorporating recommendations on reduction techniques, implant choices, and post-operative care derived from systematic reviews and randomized controlled trials. These guidelines continually evolve with advances in surgical techniques and understanding of fracture biology.
Clinical & Radiographic Imaging

You Might Also Like


