Comprehensive Guide to Humerus & Elbow: Surgical Anatomy, Biomechanics, & Pathologies
Key Takeaway
The arm, surgically defined, includes the humerus and elbow joint. Key pathologies involve humerus fractures (proximal, shaft, distal) and elbow instability, particularly ulnar collateral ligament (UCL) injuries. Understanding the humerus's osteology, its articulation with the ulna and radius, and the arm's musculature, especially the radial nerve's path, is crucial for effective diagnosis and surgical management.
Introduction & Epidemiology
The "arm," as defined surgically and anatomically in this context, primarily refers to the segment between the shoulder and elbow joints, housing the humerus bone, its associated musculature, and critical neurovascular structures. The elbow joint, a complex hinge and pivot joint, represents a crucial functional articulation often implicated in arm pathologies. This reference guide will focus on the surgical anatomy, biomechanics, and management strategies pertinent to common pathologies of the humerus and elbow ligaments, specifically fractures of the humerus (proximal, shaft, distal) and elbow instability, particularly ulnar collateral ligament (UCL) injuries.
Humerus fractures account for approximately 5% of all fractures. Proximal humerus fractures are most common in elderly osteoporotic individuals, often resulting from low-energy falls, with bimodal peaks in young males (high-energy trauma) and elderly females. Humerus shaft fractures represent 1-3% of all fractures, frequently associated with radial nerve palsy. Distal humerus fractures are less common but often complex, particularly in the elderly, and require meticulous surgical reconstruction to restore articular congruity and function. Elbow ligamentous injuries, especially UCL ruptures, are prevalent in overhead throwing athletes, with an increasing incidence due to sports specialization and intensity. Lateral collateral ligament (LCL) complex injuries are typically associated with elbow dislocations. A thorough understanding of the intricate anatomy and biomechanics is paramount for successful surgical intervention and optimal functional outcomes.
Surgical Anatomy & Biomechanics
Osteology of the Arm
The humerus is the sole bone of the arm, articulating proximally with the scapula at the glenohumeral joint and distally with the ulna and radius at the elbow joint.
Humerus
The humerus is divided into three functional segments:
- Proximal Humerus: Comprises the head, anatomical neck, surgical neck, greater tuberosity, lesser tuberosity, and bicipital groove. The surgical neck is a common site for fractures due to its metaphyseal-diaphyseal junction. The greater tuberosity serves as the insertion site for the supraspinatus, infraspinatus, and teres minor, while the lesser tuberosity receives the subscapularis tendon.
-
Humerus Shaft:
The diaphysis extends from the surgical neck to the supracondylar ridges. Key anatomical landmarks include the deltoid tuberosity on the anterolateral aspect, where the deltoid muscle inserts.
- The posterior spiral groove (for the radial nerve) is a critical surgical consideration, located adjacent to the deltoid tuberosity, running obliquely from proximal medial to distal lateral across the posterior aspect of the shaft. The radial nerve travels in this groove, making it vulnerable during fixation of mid-shaft humerus fractures, particularly with posterior approaches or screw placement from anterior/lateral.
-
Distal Humerus:
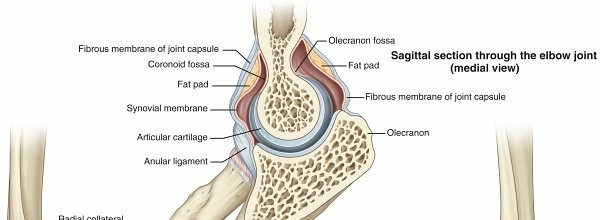
Comprises the medial and lateral epicondyles, the medial and lateral supracondylar ridges, the olecranon fossa, coronoid fossa, radial fossa, and the articular surface.
- Trochlea: The medial spool-shaped articular structure, articulating with the trochlear notch (olecranon and coronoid processes) of the ulna, providing primary sagittal plane stability to the elbow.
- Capitellum: The lateral globe-shaped articular structure, opposing the radial head. Its articulation allows for pronation and supination.
- The articular surface of the distal humerus has a 7-degree valgus tilt relative to the shaft , defining the carrying angle of the elbow. This carrying angle is crucial for normal forearm alignment and function, allowing the forearm to clear the hip during gait.

Proximal Ulna and Radius
While technically forearm bones, their proximal portions are integral to elbow joint function and stability.
*
Ulna:
The trochlear notch of the olecranon and coronoid process articulates with the humeral trochlea. The olecranon provides a strong lever arm for the triceps and is a common site for avulsion fractures. The coronoid process is a primary osseous stabilizer against posterior displacement. The sublime tubercle, located on the medial aspect of the coronoid, is the attachment site for the anterior bundle of the UCL.
*
Radius:
The radial head articulates with the capitellum and the radial notch of the ulna. It is a secondary stabilizer to valgus stress, particularly in flexion, and crucial for forearm rotation.
Musculature of the Arm
The muscles of the arm are divided into anterior (flexor) and posterior (extensor) compartments by the medial and lateral intermuscular septa.
Anterior Compartment (Flexors)
Innervated primarily by the musculocutaneous nerve (C5-C7). Blood supply from the brachial artery.
*
Biceps Brachii:
* Origin: Long head (supraglenoid tubercle), short head (coracoid process).
* Insertion: Radial tuberosity, bicipital aponeurosis.
* Action: Powerful forearm supinator, elbow flexor (especially with supination), weak shoulder flexor.
* Surgical relevance: The long head tendon is a common source of shoulder pathology; the muscle bellies are superficial, requiring careful retraction in anterior humeral approaches.
*
Brachialis:
* Origin: Distal half of the anterior humerus.
* Insertion: Coronoid process and ulnar tuberosity.
* Action: Primary elbow flexor (pure flexion, independent of forearm rotation).
* Surgical relevance: Lies deep to the biceps; important landmark for anterior approaches to the distal humerus and elbow. The musculocutaneous nerve lies on its anterior surface proximally, piercing it distally.
*
Coracobrachialis:
* Origin: Coracoid process.
* Insertion: Medial mid-shaft humerus.
* Action: Adducts and weakly flexes the arm.
* Surgical relevance: The musculocutaneous nerve pierces this muscle, a consistent landmark.
Posterior Compartment (Extensor)
Innervated by the radial nerve (C6-C8). Blood supply from the profunda brachii artery.
*
Triceps Brachii:
* Origin: Long head (infraglenoid tubercle), lateral head (posterior humerus superior to spiral groove), medial head (posterior humerus inferior to spiral groove).
* Insertion: Olecranon process of the ulna.
* Action: Powerful elbow extensor; long head also extends and adducts the shoulder.
* Surgical relevance: Forms the bulk of the posterior arm. The radial nerve runs between the lateral and medial heads in the spiral groove, then pierces the lateral intermuscular septum to become anterior. Posterior approaches to the humerus shaft often involve splitting the triceps or mobilizing it. Distal humerus posterior approaches require careful management (olecranon osteotomy vs. triceps-sparing approaches).
Ligaments of the Elbow Joint
The elbow joint's stability is provided by osseous congruity, particularly the ulnohumeral articulation, and robust collateral ligament complexes.

Medial (Ulnar) Collateral Ligament (UCL) Complex
The primary valgus stabilizer of the elbow. It consists of three distinct bundles, but the anterior bundle is the strongest and most critical.
-
Table: Elbow Ligaments - Medial (Ulnar) Collateral Ligament (UCL) Components
| Ligament Component | Origin | Insertion | Comment(s) |
| :----------------- | :------------------------------------------------ | :----------------------------------------------------------- | :------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- |
| Anterior Bundle | Anteroinferior portion of the medial humeral epicondyle | Sublime tubercle (18 mm distal to coronoid tip) | 1. Strongest elbow ligament and primary restraint to valgus stress.
2. Taut from 60 degrees of flexion to full extension.
3. Reconstructed in UCL reconstruction (Tommy John surgery).
4. Composed of an anterior band (primary restraint) and a posterior band (secondary restraint). |
| Posterior Bundle | Medial epicondyle | Medial aspect of olecranon | 1. Fan-shaped, thickening of the posterior capsule.
2. Secondary restraint to valgus stress.
3. Most taut in extreme flexion (>90 degrees).
4. Forms the floor of the cubital tunnel. |
| Transverse Bundle | Medial epicondyle | Medial aspect of coronoid process | 1. Variable presence.
2. Provides minimal elbow stability; does not cross the joint. |
Lateral Collateral Ligament (LCL) Complex
The primary varus and posterolateral rotatory stabilizer of the elbow. Consists of:
*
Radial Collateral Ligament (RCL):
Originates from the lateral epicondyle, blends with the annular ligament. Primary varus stabilizer.
*
Lateral Ulnar Collateral Ligament (LUCL):
Originates from the lateral epicondyle, inserts onto the supinator crest of the ulna. The most critical component of the LCL complex, preventing posterolateral rotatory instability (PLRI) of the elbow.
*
Accessory Lateral Collateral Ligament (ALCL):
Originates from the lateral epicondyle, inserts onto the annular ligament.
*
Annular Ligament:
Encircles the radial head, maintaining its articulation with the radial notch of the ulna.

Neurovascular Structures
Several critical neurovascular structures traverse the arm and are at risk during surgical approaches.
-
Radial Nerve:
- Course: Exits the axilla posterior to the brachial artery, spirals around the posterior humerus in the spiral groove, then pierces the lateral intermuscular septum to enter the anterior compartment near the elbow. Divides into superficial (sensory) and deep (posterior interosseous nerve, motor) branches.
- Surgical relevance: Extremely vulnerable during approaches to the mid-shaft humerus, particularly posterior and direct lateral approaches. Careful identification and protection are paramount.
-
Ulnar Nerve:
- Course: Travels medially in the arm, passes posterior to the medial epicondyle (cubital tunnel), then enters the forearm.
- Surgical relevance: Highly susceptible to injury or irritation during medial elbow approaches (UCL reconstruction), distal humerus fractures, or during extensive elbow dissection. Transposition may be required.
-
Median Nerve:
- Course: Travels alongside the brachial artery throughout the arm, crossing it usually anteriorly. Enters the forearm anterior to the elbow joint.
- Surgical relevance: At risk during extensive anterior dissection of the distal humerus or medial elbow.
-
Brachial Artery:
- Course: Main artery of the arm, courses with the median nerve. Divides into radial and ulnar arteries at the cubital fossa.
- Surgical relevance: At risk in anterior approaches, particularly in supracondylar humerus fractures in children, or in cases of severe trauma with neurovascular compromise.
- Profunda Brachii Artery: Large branch of the brachial artery, accompanies the radial nerve in the spiral groove. Supplies the posterior compartment.
Indications & Contraindications
Surgical intervention in the arm, particularly for humerus fractures and elbow ligamentous injuries, is guided by fracture morphology, patient factors, associated injuries, and functional demands.
Humerus Fractures
Proximal Humerus Fractures
-
Operative Indications:
- Neer 3- and 4-part fractures in physiologically active patients.
- Two-part surgical neck fractures with significant displacement (>1 cm) or angulation (>45 degrees).
- Displaced two-part greater tuberosity fractures (>5 mm displacement) preventing abduction.
- Fracture-dislocations.
- Head-splitting fractures (often require arthroplasty).
- Irreducible fractures.
- Pathologic fractures.
-
Non-Operative Indications:
- Non-displaced or minimally displaced one- and two-part fractures.
- Impacted valgus-type fractures.
- Patients with significant medical comorbidities precluding surgery.
- Low functional demands.
Humerus Shaft Fractures
-
Operative Indications:
- Open fractures.
- Vascular injury requiring repair.
- Associated nerve injury (especially open fracture with nerve injury, or nerve injury after closed reduction attempt), though isolated radial nerve palsy is not an absolute indication for immediate exploration in closed fractures.
- Pathologic fractures.
- Segmental fractures.
- Polytrauma patients requiring early mobilization.
- Floating elbow (ipsilateral forearm fracture).
- Obesity or non-compliance where cast management is impractical.
- Nonunion or symptomatic malunion.
- Fractures with significant comminution that are unstable in a brace.
-
Non-Operative Indications:
- Closed, isolated humerus shaft fractures with acceptable alignment (angulation <20 degrees anterior-posterior, <30 degrees varus-valgus, <3 cm shortening, minimal rotation).
- Radial nerve palsy with closed fracture (often observed for spontaneous recovery).
Distal Humerus Fractures
-
Operative Indications:
- Displaced intra-articular fractures (Type C) to restore articular congruity.
- Displaced supracondylar fractures (Type A) in adults.
- Open fractures.
- Fracture-dislocations.
- Associated neurovascular injury.
-
Non-Operative Indications:
- Non-displaced extra-articular fractures in elderly patients with low demands.
- Minimally displaced intra-articular fractures where risks of surgery outweigh benefits.
- Patients with severe medical comorbidities.
Elbow Ligamentous Injuries
UCL Injuries (Medial Elbow Instability)
-
Operative Indications (UCL Reconstruction/Repair):
- Complete tear of the anterior bundle in overhead throwing athletes or laborers requiring valgus stability.
- Chronic valgus instability unresponsive to conservative management.
- Ulnar nerve compression in conjunction with valgus instability.
-
Non-Operative Indications:
- Partial tears without significant functional instability.
- Non-throwing athletes or low-demand individuals without symptomatic instability.
- Acute injuries in non-athletes with mild laxity.
LCL Complex Injuries (Lateral Elbow Instability, PLRI)
-
Operative Indications (LCL Reconstruction/Repair):
- Recurrent posterolateral rotatory instability (PLRI) following elbow dislocation.
- Chronic LCL insufficiency causing symptomatic instability.
-
Non-Operative Indications:
- Often managed with closed reduction and brief immobilization for acute dislocations without evidence of recurrent instability.
Contraindications
General contraindications for any surgical procedure apply, including:
* Active infection (unless it is the indication for surgery, e.g., open fracture debridement).
* Severe uncontrolled medical comorbidities.
* Inadequate skin coverage or soft tissue envelope.
* Patient refusal or inability to comply with postoperative rehabilitation.
Table: Operative vs. Non-Operative Indications for Arm Pathologies
| Pathology | Operative Indications | Non-Operative Indications |
|---|---|---|
| Proximal Humerus Fractures | Neer 3/4 part, displaced 2-part surgical neck, displaced GT, head-split, fracture-dislocation, irreducible | Non-displaced/minimally displaced 1/2 part, impacted valgus, low demand, high comorbidity |
| Humerus Shaft Fractures | Open, vascular injury, pathological, segmental, polytrauma, floating elbow, nonunion/malunion, severe comminution | Closed, isolated, acceptable alignment, isolated radial nerve palsy |
| Distal Humerus Fractures | Displaced intra-articular (Type C), displaced supracondylar (Type A), open, fracture-dislocation | Non-displaced extra-articular, minimally displaced in elderly/low demand, high comorbidity |
| UCL Injuries | Complete anterior bundle tear in athletes, chronic valgus instability, ulnar nerve entrapment | Partial tears without instability, non-athletes without symptoms |
| LCL Complex Injuries (PLRI) | Recurrent PLRI, chronic LCL insufficiency | Acute dislocations with stable reduction, no recurrent instability |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for optimizing surgical outcomes and minimizing complications.
Pre-Operative Planning
- Detailed History & Physical Examination: Assess neurovascular status, associated injuries, skin condition, and patient's functional demands.
-
Imaging:
- X-rays: AP, lateral, and true scapular Y views for the shoulder; AP and lateral views for the elbow. Oblique views or stress views (for ligaments) as needed.
- CT Scan: Crucial for complex intra-articular fractures (distal humerus, proximal humerus with articular involvement) to delineate fracture pattern, comminution, and articular step-off. 3D reconstructions are highly beneficial.
- MRI: Essential for soft tissue injuries, especially UCL tears, to assess tear location, extent, and associated pathologies. May also be useful for occult fractures or rotator cuff tears with proximal humerus fractures.
- Templating: Pre-operative templating with contralateral radiographs (if uninjured) helps determine implant size and position for plates, screws, or arthroplasty components.
- Surgical Approach Selection: Based on fracture pattern, location, associated injuries, surgeon preference, and exposure required.
- Equipment & Instrumentation: Ensure all necessary implants (plates, screws, K-wires, sutures, anchors, arthroplasty components, graft harvest kits) and specialized instruments are available.
Patient Positioning
Appropriate patient positioning is critical for optimal exposure, fracture reduction, and surgeon comfort. Fluoroscopy setup is often required.
-
Proximal Humerus Fractures (ORIF/Arthroplasty):
- Beach Chair Position: Allows excellent access to the shoulder, ability to move the arm, and avoids potential issues with arm pads. Arm is draped free.
- Supine Position: Often used for trauma, on a radiolucent table with a bump under the ipsilateral scapula. Arm can be draped free or placed on a hand table. Traction may be applied.
-
Humerus Shaft Fractures:
- Supine Position: For anterolateral or deltopectoral approaches. Arm draped free, often with a sterile tourniquet.
- Lateral Decubitus Position: For posterior or posterolateral approaches, or when a patient's body habitus precludes supine positioning. Affected arm supported by an arm holder or draped over an overhead frame.
- Prone Position: Rarely used, but can offer excellent posterior exposure.
-
Distal Humerus Fractures / Elbow Ligamentous Reconstruction:
- Supine Position: Arm on a hand table, or suspended with a bolster under the shoulder to allow full elbow extension and flexion.
- Lateral Decubitus Position: With the arm draped over a chest roll or a dedicated arm holder, allowing good access to all aspects of the elbow. A sterile tourniquet is common.
Detailed Surgical Approach / Technique
Humerus Fracture Fixation
Proximal Humerus ORIF (e.g., PHF Plating via Deltopectoral Approach)
- Incision: Deltopectoral groove incision, extending from the coracoid process distally.
- Interval: Identify the cephalic vein; retract laterally with the deltoid or medially with the pectoralis major. Develop the interval between the deltoid (lateral) and pectoralis major (medial).
- Deep Dissection: Incise the clavipectoral fascia. The conjoint tendon (coracobrachialis and short head of biceps) is retracted medially. The musculocutaneous nerve lies on the deep surface of the coracobrachialis.
- Exposure: The subscapularis tendon is exposed. For most proximal humerus fractures, the upper border of the pectoralis major insertion is identified. The deltoid is elevated off the humerus from the greater tuberosity as needed.
- Reduction: Indirect reduction techniques (traction, ligamentotaxis) or direct manipulation with K-wires, bone hooks, or reduction clamps. Restore articular congruity and tuberosity reduction. Fluoroscopic guidance is essential.
- Fixation: Apply a pre-contoured locking plate (e.g., PHILOS plate) laterally, positioned approximately 5-8 mm distal to the superior aspect of the greater tuberosity to avoid impingement. Place multiple locking screws into the humeral head to achieve maximal pullout strength, aiming for subchondral bone. Secure shaft screws. Assess rotator cuff tendon integrity and repair if necessary.
Humerus Shaft ORIF (e.g., Anterolateral Approach)
- Incision: Longitudinal incision on the anterolateral aspect of the arm, centered over the fracture.
- Interval: Develop the interval between the deltoid and pectoralis major proximally. Distally, the interval is between the biceps brachii (medially) and the brachialis (deep/posterior) or the lateral head of the triceps (laterally).
- Deep Dissection: Carefully identify and protect the cephalic vein and musculocutaneous nerve (lying on the brachialis or piercing coracobrachialis).
- Radial Nerve: This is the critical structure. The anterolateral approach generally keeps the radial nerve posterior to the plane of dissection, as it exits the spiral groove through the lateral intermuscular septum typically distal to the deltoid tuberosity. Identify the lateral intermuscular septum. The radial nerve is posterior to this septum in the middle and distal third of the arm. For more proximal fractures, the nerve may be more posterior.
- Exposure & Reduction: Elevate the brachialis from the anterior surface of the humerus. Reduce the fracture under fluoroscopy.
- Fixation: Apply a locking compression plate (LCP) to the anterolateral surface. Consider minimally invasive plate osteosynthesis (MIPO) techniques to preserve soft tissue and blood supply, utilizing small incisions proximal and distal to the fracture site and tunneling the plate submuscularly.
Distal Humerus ORIF (e.g., Posterior Transolecranon Approach)
- Incision: Posterior longitudinal incision over the olecranon, extending proximally along the triceps and distally over the ulna.
- Ulnar Nerve: Identify and protect or transpose the ulnar nerve from the cubital tunnel.
- Olecranon Osteotomy: Perform a chevron or transverse osteotomy of the olecranon using an oscillating saw. This provides excellent exposure to the distal humerus articular surface. Reflect the triceps proximally with the osteotomized olecranon.
- Exposure: The entire distal humerus articular surface and columns are exposed.
- Reduction: Meticulously reduce the articular fragments first, often using K-wires for temporary fixation. Restore the capitellotrochlear anatomy. Then reduce the humeral columns to the shaft.
- Fixation: Dual-plate fixation is the standard for complex intra-articular fractures. Typically, a posterolateral plate (for the lateral column) and a posterior or medial plate (for the medial column). Plates should be orthogonal or parallel, providing strong fixation. The medial plate is positioned on the medial supracondylar ridge. The lateral plate may be posterior or posterolateral. Reconstruct the olecranon osteotomy with a tension band wiring technique or plate/screws.
Elbow Ligament Reconstruction
Ulnar Collateral Ligament (UCL) Reconstruction (Tommy John Surgery)
- Incision: Medial longitudinal incision, centered over the medial epicondyle.
- Ulnar Nerve: Carefully identify and protect the ulnar nerve. It is often transposed submuscularly or subcutaneously to prevent postoperative irritation or compression.
- Ligament Exposure: Incise the flexor-pronator mass carefully along its fibers or elevate it off the medial epicondyle to expose the UCL. Confirm the tear site (often at the humeral origin).
- Graft Harvest: Commonly palmaris longus or gracilis autograft.
-
Drill Tunnels:
- Humeral Tunnel: A single drill hole or "figure-of-8" configuration originating at the isometric point on the medial epicondyle (between the coronoid fossa and the epicondyle).
- Ulnar Tunnels: Two divergent drill holes in the sublime tubercle of the ulna, approximately 18 mm distal to the coronoid tip.
- Graft Passage & Fixation: Pass the graft through the tunnels. The most common techniques are the docking technique (graft passed through humeral tunnel, ends docked into ulnar tunnels) or figure-of-8 technique (graft woven through tunnels). Tension the graft with the elbow in 30-70 degrees of flexion (often 30 degrees for docking technique) and forearm pronation. Fix with interference screws, cortical buttons, or suture anchors.
- Closure: Repair the flexor-pronator mass. Close skin.
Lateral Ulnar Collateral Ligament (LUCL) Reconstruction/Repair
- Incision: Posterolateral longitudinal incision, centered over the lateral epicondyle.
- Exposure: Elevate the anconeus and common extensor origin to expose the lateral epicondyle and supinator crest of the ulna. Identify the annular ligament.
-
Drill Tunnels:
- Humeral Tunnel: Isometric point on the lateral epicondyle.
- Ulnar Tunnel: Supinator crest of the ulna.
- Graft Passage & Fixation: Pass a graft (e.g., palmaris longus) through the tunnels in an anatomical fashion, replicating the LUCL's course. Tension with the elbow in 30-40 degrees of flexion and forearm pronation. Fix with screws or anchors.
- Repair of Capsule/Extensors: Repair any capsular or extensor defects.
Complications & Management
Complications associated with arm surgeries can be significant and impact long-term function. Vigilance and appropriate management are crucial.
Humerus Fracture Fixation Complications
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Nonunion | Proximal: 5-10%; Shaft: 5-10%; Distal: 10-20% | Revision ORIF with debridement, bone grafting (autograft/allograft), stronger fixation (e.g., dual plating, intramedullary nail), adjunctive modalities (e.g., bone stimulators). |
| Malunion | Variable, depends on fracture type and fixation | Corrective osteotomy with ORIF if symptomatic (pain, impingement, reduced ROM). Arthroplasty for severe articular malunion (e.g., distal humerus). |
| Nerve Injury | Radial nerve (shaft): 10-18% (often transient) | For iatrogenic injury or lack of recovery: Nerve exploration, neurolysis, direct repair or graft, tendon transfers (e.g., for radial nerve palsy). Close observation for initial closed radial nerve palsy. |
| Infection | 1-5% | Debridement, irrigation, antibiotics (IV/oral), hardware retention vs. removal (depending on stability and severity), soft tissue coverage. May require staged reconstruction. |
| Stiffness/AROM Loss | High, especially with distal humerus and proximal humerus fractures | Early controlled motion, intensive physical therapy, serial manipulation under anesthesia (MUA), arthroscopic or open arthrolysis. Heterotopic ossification prophylaxis (NSAIDs/radiation). |
| Hardware Failure/Implant Impingement | Variable | Removal of hardware if asymptomatic after healing. Revision fixation if fracture nonunion or malunion. For impingement (proximal humerus plates), consider implant removal after fracture union. |
| Avascular Necrosis (AVN) | Proximal humerus (3-4 part): 10-30% | Hemiarthroplasty or reverse total shoulder arthroplasty (rTSA) in symptomatic cases. |
Elbow Ligamentous Reconstruction Complications
| Complication | Incidence | Salvage Strategies |
|---|---|---|
| Elbow Stiffness/AROM Loss | 5-15% | Early controlled motion protocol, intensive physical therapy, dynamic splinting, MUA, arthroscopic or open arthrolysis, removal of hardware if it is causing mechanical block. Heterotopic ossification prophylaxis. |
| Ulnar Nerve Neuropathy | 5-20% (UCL reconstruction) | Observation for transient symptoms. Neurolysis, revision transposition if persistent symptoms or nerve entrapment. |
| Recurrent Instability/Graft Failure | 5-10% | Revision reconstruction with stronger graft, different technique, or adjunctive procedures (e.g., osteophyte removal, capsular plication). |
| Infection | <1% | Debridement, irrigation, antibiotics. Hardware removal. May require staged reconstruction or external fixation if severe. |
| Heterotopic Ossification (HO) | 1-5%, higher after trauma or multiple surgeries | Prophylaxis (NSAIDs, low-dose radiation post-op). Excision of HO if symptomatic and mature (typically >6 months post-onset) and causing significant motion restriction. |
| Donor Site Morbidity | Variable (e.g., palmaris longus, gracilis) | Usually minor (pain, numbness, weakness). Managed symptomatically. Rare cases of chronic pain or functional deficit that may require local nerve block or surgical exploration. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is critical for restoring function, preventing stiffness, and ensuring successful integration of repaired/reconstructed structures. Protocols are highly specific to the procedure, fracture stability, and patient factors.
Humerus Fracture Rehabilitation (General Principles)
-
Proximal Humerus (ORIF):
- Phase I (0-6 weeks, Protection & Early Motion): Sling immobilization (often for 2-4 weeks), passive range of motion (PROM) for glenohumeral and elbow/wrist/hand joints. Pendulum exercises. Goal: prevent stiffness, protect healing.
- Phase II (6-12 weeks, Active Motion & Strengthening): Progress to active assistive range of motion (AAROM) and active range of motion (AROM). Isometric strengthening, light resistive exercises. Discontinue sling. Goal: restore full ROM, begin strength.
- Phase III (12+ weeks, Advanced Strengthening & Return to Activity): Progressive strengthening, endurance training, proprioception. Sport-specific or work-specific activities. Goal: achieve maximal functional recovery.
-
Humerus Shaft (ORIF):
- Phase I (0-2 weeks, Protection & Early Motion): Sling for comfort. Early elbow, wrist, and hand ROM exercises. Avoid active shoulder abduction/external rotation depending on plate position.
- Phase II (2-6 weeks, Progressive Motion): Initiate gentle PROM/AAROM of the shoulder and elbow. Gradual progression to AROM.
- Phase III (6-12 weeks, Strengthening): Once radiographic evidence of healing is present, begin progressive isometric and isotonic strengthening.
- Phase IV (12+ weeks, Return to Activity): Advanced strengthening, functional drills.
-
Distal Humerus (ORIF):
- Phase I (0-3 weeks, Protection & Gentle Motion): Often immobilized in a posterior splint or brace for 1-2 weeks. Initiate early PROM/AAROM of the elbow (gravity-assisted flexion, supine extension) within a pain-free arc as tolerated. Avoid active lifting.
- Phase II (3-6 weeks, Progressive Motion): Advance to AROM. Gentle forearm pronation/supination. Initiate light grip strengthening.
- Phase III (6-12 weeks, Strengthening): Once fracture healing is confirmed, begin progressive strengthening with resistance bands, light weights. Address any stiffness (dynamic splinting if needed).
- Phase IV (12+ weeks, Advanced Function): Progressive return to full activity.
Elbow Ligament Reconstruction Rehabilitation
-
UCL Reconstruction (Tommy John Surgery):
- Phase I (0-6 weeks, Immobilization & Protection): Long arm splint at 90 degrees flexion, then hinged elbow brace with restricted ROM (e.g., 30-100 degrees flexion) for initial weeks. Gentle wrist/hand ROM. Isometric shoulder exercises. Avoid valgus stress.
- Phase II (6-10 weeks, Progressive ROM & Strengthening): Gradual increase in elbow ROM (e.g., 10-degree increments per week). Light isotonic exercises for shoulder and elbow. Avoid overhead activities.
- Phase III (10-16 weeks, Interval Throwing Program Preparation): Full, pain-free ROM. Progressive strengthening, endurance, and core stability. Light plyometrics. Initiate low-velocity, short-distance throwing in a controlled manner (Phase I of throwing program).
- Phase IV (4-6 months+, Interval Throwing Program Progression): Gradual increase in throwing velocity, distance, and intensity. Return to competitive play typically 9-18 months post-op, depending on sport and position.
-
LCL Reconstruction/Repair:
- Phase I (0-4 weeks, Immobilization & Protection): Hinged elbow brace locked at 30-90 degrees flexion with forearm pronation to minimize stress on the repair. Gentle wrist/hand ROM.
- Phase II (4-8 weeks, Progressive ROM): Gradual increase in elbow ROM, keeping forearm pronated for initial weeks. Avoid varus stress and supination with extension.
- Phase III (8-12 weeks, Strengthening): Initiate light strengthening. Progress to full ROM.
- Phase IV (12+ weeks, Return to Activity): Progressive return to functional activities.
Summary of Key Literature / Guidelines
Evidence-based guidelines inform optimal management of arm pathologies:
- Proximal Humerus Fractures: The literature continues to debate the optimal treatment for displaced 3- and 4-part fractures in the elderly. While ORIF with locking plates remains a common choice, hemiarthroplasty and reverse total shoulder arthroplasty (rTSA) are increasingly utilized, particularly for comminuted fractures, severe osteopenia, or rotator cuff deficiency. The DELPHI study group has provided consensus recommendations for treatment algorithms.
- Humerus Shaft Fractures: Functional bracing remains the gold standard for most closed, isolated humerus shaft fractures, demonstrating high union rates. Operative management is reserved for specific indications as outlined, with intramedullary nailing and plate osteosynthesis being the predominant surgical techniques. The choice depends on fracture pattern, soft tissue status, and surgeon preference, with plating generally offering better rotational control.
- Distal Humerus Fractures: Restoration of articular congruity and stable internal fixation with dual-plate osteosynthesis (orthogonal or parallel) is critical for functional outcomes. Good long-term results are contingent on meticulous surgical technique and aggressive, early range of motion. Total elbow arthroplasty (TEA) is a viable option for highly comminuted fractures in elderly, low-demand patients.
- UCL Reconstruction: The success of UCL reconstruction (Tommy John surgery), pioneered by Dr. Frank Jobe, has been well-documented. Modern techniques emphasize anatomic reconstruction, ulnar nerve protection, and careful graft tensioning. Return-to-play rates for professional athletes are high, but the recovery period is protracted. Literature highlights the importance of specific throwing programs and strength conditioning.
- LCL Complex Injuries: Management of acute elbow dislocations focuses on stable reduction. For recurrent PLRI, anatomical reconstruction of the LUCL is the treatment of choice, aiming to restore stability and prevent recurrent dislocations.
- General Principles: Across all areas, early, controlled mobilization is a recurring theme to prevent stiffness. Prophylaxis against heterotopic ossification (e.g., NSAIDs) is commonly considered for high-risk elbow trauma. Awareness of specific nerve anatomy is paramount in all surgical exposures of the arm.
You Might Also Like

