The Growing Problem of Osteoporosis: Your Guide to Prevention & Treatment

Key Takeaway
This article provides essential research regarding The Growing Problem of Osteoporosis: Your Guide to Prevention & Treatment. Osteoporosis is a condition weakening bones and causing brittle fractures, impacting quality of life with pain, disability, and even death. The problem of osteoporosis is escalating, driven by an aging population, lifestyle changes, and improved diagnosis. Addressing this serious health concern is crucial for improving public health and well-being across all ages.
Introduction & Epidemiology
Osteoporosis, a systemic skeletal disorder characterized by compromised bone strength predisposing to an increased risk of fracture, represents a significant public health challenge with profound implications for orthopedic surgery. While primary osteoporosis is an age-related decline in bone mineral density (BMD) and microarchitectural integrity, secondary osteoporosis can stem from various underlying medical conditions, medications, or lifestyle factors. The orthopedic surgeon primarily encounters the devastating consequences of osteoporosis: fragility fractures. These fractures, defined as occurring from a fall from a standing height or less, are sentinel events signifying underlying skeletal fragility.
The epidemiological burden of osteoporosis and its associated fragility fractures is substantial and escalating. Globally, an estimated 200 million people are affected by osteoporosis. In the United States, over 10 million individuals are estimated to have osteoporosis, with an additional 43 million having low bone mass (osteopenia), placing them at elevated risk for future fractures. The incidence of fragility fractures, particularly hip, vertebral, and distal radius fractures, rises exponentially with age. Hip fractures, the most devastating of fragility fractures, are projected to increase by over 240% in men and 310% in women by 2050, largely driven by the aging global population. These fractures lead to significant morbidity, including chronic pain, functional impairment, loss of independence, increased rates of long-term care placement, and a substantial excess mortality risk, particularly in the year following a hip fracture. From an economic perspective, the healthcare costs associated with treating fragility fractures are staggering, exceeding $20 billion annually in the U.S. alone, underscoring the imperative for comprehensive orthopedic management strategies.
Surgical Anatomy & Biomechanics
The anatomical and biomechanical characteristics of osteoporotic bone present unique challenges for surgical intervention. Osteoporosis is fundamentally a disorder of bone
quality
and
quantity
.
From an anatomical perspective, osteoporotic bone exhibits:
*
Reduced Cortical Thickness:
The outer cortical shell, crucial for resisting bending and torsional forces, becomes thinner and more porous.
*
Decreased Trabecular Bone Density:
The internal trabecular network, essential for compressive strength and load distribution, undergoes significant architectural deterioration, with loss of horizontal struts and thinning of vertical struts. This results in increased trabecular spacing and reduced connectivity.
*
Increased Bone Turnover Markers:
While not directly anatomical, altered bone remodeling pathways contribute to microarchitectural damage.
Biomechanical implications for surgical fixation are profound:
*
Reduced Implant Anchorage:
The primary purchase of orthopedic implants relies on screws engaging competent bone. In osteoporotic bone, the pull-out strength of screws is significantly diminished due to decreased bone density and compromised bone-screw interface. This leads to an increased risk of screw loosening, backing out, or cutting through the bone (cut-out).
*
Increased Risk of Periprosthetic Fracture:
The reduced strength of the surrounding bone makes it more susceptible to fracture during implant insertion or due to stress risers created by the implant itself.
*
Compromised Load Transfer:
The ability of osteoporotic bone to effectively transfer loads across the fracture site and around implants is diminished, contributing to delayed union, non-union, or refracture adjacent to implants.
*
Fracture Patterns:
Fragility fractures often present with comminution, impaction, and an inability to maintain reduction due to the inherent weakness of the bone fragments. Specific fracture patterns, such as intracapsular femoral neck fractures or highly comminuted distal radius fractures, are particularly challenging due to the tenuous blood supply and inability of osteoporotic bone to provide robust purchase for fixation.
*
Sites of Predilection:
The metaphyseal regions of long bones (e.g., distal radius, proximal humerus, proximal femur) and vertebral bodies are particularly vulnerable due to their high content of trabecular bone, which is more metabolically active and thus more susceptible to osteoporotic changes compared to cortical bone.
Effective surgical strategies in osteoporotic bone must account for these biomechanical realities, emphasizing techniques that maximize implant purchase, distribute stress, and promote biological healing in a compromised environment.
Indications & Contraindications
The decision-making process for operative versus non-operative management of fragility fractures in osteoporotic patients is complex, balancing fracture characteristics, patient comorbidities, functional goals, and the inherent challenges of fixation in weakened bone. Generally, the aim is to restore function, alleviate pain, and prevent complications.
Operative Indications (General Principles for Fragility Fractures):
- Displaced or Unstable Fractures: Fractures that are significantly displaced or inherently unstable and unlikely to heal in an acceptable alignment with conservative measures.
- Intra-articular Fractures: Fractures involving joint surfaces, especially if displaced, to restore articular congruity and prevent post-traumatic arthritis.
- Non-union or Malunion: Failed conservative management or fractures that have healed in an unacceptable position causing significant functional deficit.
- Pathologic Fractures: Fractures through areas of neoplastic involvement, often requiring stabilization to prevent impending fracture or alleviate pain.
- Neurovascular Compromise: Fractures causing acute compromise of neurovascular structures.
- Early Mobilization Requirement: In elderly, often frail patients, surgical stabilization frequently allows earlier weight-bearing and mobilization, which is crucial for preventing deconditioning, pressure ulcers, pneumonia, and DVT/PE. This is a particularly strong indication for hip fractures.
Non-Operative Indications (General Principles for Fragility Fractures):
- Minimally Displaced or Stable Fractures: Fractures that are inherently stable or can be adequately reduced and maintained in an acceptable position with external immobilization (e.g., cast, brace) or protected weight-bearing.
- High Surgical Risk: Patients with significant medical comorbidities that contraindicate surgery or carry an unacceptably high anesthetic or surgical risk.
- Low Functional Demand: Patients with very limited pre-injury functional status or severe cognitive impairment where the potential benefits of surgery do not outweigh the risks.
- Patient Preference: When adequately informed, the patient (or their surrogate decision-maker) may opt for non-operative management despite surgical indications.
- Certain Vertebral Compression Fractures: Most osteoporotic vertebral compression fractures are treated non-operatively with pain management, bracing, and early mobilization, with percutaneous augmentation (kyphoplasty/vertebroplasty) reserved for intractable pain or progressive collapse.
Specific Fracture Indications (Operative vs. Non-Operative):
| Fracture Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Proximal Femur | - Femoral Neck: Displaced (Garden III/IV) in ambulatory patients (arthroplasty - hemi/total). Non-displaced (Garden I/II) in younger, higher functional demand patients (internal fixation, e.g., cannulated screws). | - Femoral Neck: Non-displaced (Garden I/II) in very low-demand, non-ambulatory patients or those with prohibitive surgical risk (controversial, often leads to failure). |
| - Intertrochanteric: Virtually all displaced/unstable fractures (cephalomedullary nailing preferred). | - Intertrochanteric: Extremely rare; only in non-ambulatory, comfort care patients with minimal pain, often leads to significant morbidity. | |
| - Subtrochanteric: All displaced/unstable fractures (long cephalomedullary nailing preferred). | - Rare due to high risk of non-union/malunion. | |
| Distal Radius | - Displaced Intra-articular: Articular step-off > 2mm. | - Minimally displaced, stable fractures without significant articular involvement. |
| - Unstable Extra-articular: Dorsal tilt > 10-15 degrees, radial shortening > 3-5mm, significant comminution, loss of initial reduction. | - Acceptable reduction maintained after closed reduction and casting. | |
| - Failure of closed reduction and casting to maintain acceptable alignment. | ||
| Proximal Humerus | - Displaced 2, 3, or 4-part fractures in active patients. | - Minimally displaced 1-part fractures (most common). |
| - Humeral head split fractures: Requiring arthroplasty. | - Non-displaced 2-part surgical neck or greater tuberosity fractures. | |
| - Glenohumeral dislocation with associated fracture. | - Low-demand, elderly patients with significantly displaced fractures who are not surgical candidates. | |
| Vertebral Body | - Neurologic deficit: Spinal cord compression or nerve root impingement. | - Majority of osteoporotic compression fractures without neurologic deficit (conservative management with pain control, bracing, activity modification). |
| - Progressive kyphosis/deformity: In certain cases. | - Percutaneous vertebral augmentation (vertebroplasty/kyphoplasty) for persistent, intractable pain after 6-8 weeks of conservative management, or progressive collapse. This is not open surgery. | |
| - Spinal instability: Evidence of ligamentous disruption or progressive vertebral collapse refractory to conservative measures. | ||
| Pelvis | - Unstable pelvic ring fractures: Associated with significant displacement, usually involving disruption of both anterior and posterior elements (e.g., APC II/III, LC II/III, vertical shear). | - Stable pelvic ring fractures (e.g., sacral insufficiency fractures, pubic rami fractures) managed with protected weight-bearing and pain control. |
| - Displaced acetabular fractures: Especially those leading to joint incongruity. | - Minimally displaced acetabular fractures or those in non-ambulatory patients where arthroplasty is considered for later. |
Contraindications:
Absolute contraindications for fragility fracture surgery are rare and typically relate to the patient's overall medical status rather than the fracture itself:
*
Unstable Medical Condition:
Severe uncompensated cardiac, pulmonary, or neurological disease that makes the risks of anesthesia and surgery prohibitive (e.g., active myocardial infarction, uncontrolled sepsis, severe acute stroke).
*
Terminal Illness:
Patients with a very limited life expectancy where surgery would not significantly improve comfort or quality of life.
*
Severe Sepsis:
Active systemic infection requiring control before elective or semi-elective orthopedic surgery.
*
Lack of Functional Goal:
Inability to achieve a functional gain from surgery, often seen in severely debilitated, non-ambulatory patients with certain fracture patterns (e.g., hip fracture in a patient with severe dementia and no prior ambulation).
Relative contraindications include significant dermatological issues over the surgical site, active local infection, or poorly controlled diabetes, all of which increase surgical risk. These are often managed pre-operatively to optimize the patient for surgery.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is paramount for fragility fracture management, particularly in the osteoporotic population, which often presents with significant comorbidities and compromised bone stock.
Pre-Operative Planning:
-
Medical Optimization:
- Comorbidity Assessment: Comprehensive medical evaluation by an internist, geriatrician, or hospitalist is essential. This includes cardiac risk stratification (ECG, echo, cardiology consult), pulmonary assessment (PFTs, chest X-ray), renal function, nutritional status, and glycemic control.
- Anemia Correction: Pre-operative anemia is common and should be corrected if possible to improve oxygen delivery and reduce the need for perioperative transfusions.
- Anticoagulation Management: Careful management of antiplatelet and anticoagulant medications according to institutional protocols, often requiring temporary cessation or bridging therapy.
- Bone Health Assessment: While the fracture itself indicates osteoporosis, screening for underlying bone health issues (vitamin D deficiency, secondary causes) and initiating medical treatment (e.g., bisphosphonates post-op) should be considered.
- Delirium Prevention: Implement strategies to minimize the risk of post-operative delirium, common in this population (e.g., avoiding deliriogenic medications, ensuring adequate hydration, early mobilization).
-
Imaging Review:
- Standard Radiographs: AP and lateral views are crucial for fracture classification, displacement assessment, and planning implant size/type. Obtain images of the entire bone if diaphyseal extension is suspected.
- CT Scans: Indicated for complex intra-articular fractures (e.g., acetabulum, distal radius, proximal humerus) or for detailed assessment of comminution and bone loss, especially in the proximal femur or vertebral column, to aid in implant selection and surgical approach. 3D reconstructions can be invaluable.
- MRI: Rarely indicated acutely for fracture diagnosis, but useful for assessing ligamentous injuries (e.g., pelvis), occult fractures, or ruling out tumor pathology.
-
Surgical Strategy & Implant Selection:
- Approach Selection: Based on fracture pattern, patient anatomy, and surgeon preference.
-
Implant Choice:
Critical in osteoporotic bone. Preference for:
- Angle-Stable Fixation: Locking plates and screws, cephalomedullary nails with locking options, which provide a fixed-angle construct, resisting pull-out and collapse in weak bone.
- Augmentation Techniques: Consider bone cement augmentation (PMMA) for screws in metaphyseal bone (e.g., proximal humerus, vertebral body) or acetabular reconstruction. Allograft or autograft can be used for bone defects.
- Larger Diameter Implants: Where appropriate, to maximize surface area contact and bone purchase.
- Load Sharing vs. Load Bearing: Aim for load-sharing constructs where the implant helps bear some stress but allows the bone to participate in healing, which is challenging in osteoporotic bone.
- Contingency Planning: Always have backup implants and strategies available (e.g., different plate lengths, screw types, augmentation options).
Patient Positioning:
Correct and stable patient positioning is critical to provide optimal surgical exposure, facilitate reduction, and prevent iatrogenic injury. Specific considerations for osteoporotic patients include:
*
Padding:
Meticulous padding of all pressure points to prevent skin breakdown and nerve compression, given fragile skin and reduced subcutaneous tissue.
*
Stability:
Ensure the patient is securely positioned to prevent movement during reduction maneuvers or surgical instrumentation.
*
Traction Table:
Frequently used for hip and proximal femur fractures (e.g., intertrochanteric, subtrochanteric) to aid in reduction and maintain alignment during nailing. Careful attention to perineal pressure.
*
Beach Chair / Supine:
For proximal humerus fractures, depending on the chosen approach.
*
Supine with Hand Table:
For distal radius fractures, allowing for fluoroscopic visualization and instrumentation.
Detailed Surgical Approach / Technique
Surgical techniques for fragility fractures in osteoporotic bone are characterized by principles aimed at maximizing implant stability, promoting biological healing, and minimizing iatrogenic damage. While specific approaches vary by fracture type, common themes include meticulous soft tissue handling, indirect reduction, angle-stable fixation, and potential augmentation.
We will detail the approach for a common and impactful fragility fracture: Intertrochanteric Femur Fracture treated with a Cephalomedullary Nail, and general principles applicable to Distal Radius Fractures treated with Volar Locking Plate.
1. Intertrochanteric Femur Fracture (Cephalomedullary Nailing)
This fracture often involves the metaphyseal bone of the proximal femur, notorious for its compromised quality in osteoporotic patients. Cephalomedullary nailing has become the standard of care due to its biomechanical advantages (load sharing, shorter lever arm) over plate-and-screw constructs in this region.
Patient Positioning:
* Supine on a fracture table, with the injured limb in traction. Ensure adequate perineal padding. The contralateral limb is abducted to allow C-arm access. Careful fluoroscopic screening ensures adequate views (AP and lateral) of the proximal femur, hip joint, and desired nail length distally.
Surgical Approach (Minimally Invasive):
1.
Proximal Incision:
A 3-5 cm longitudinal incision is made over the tip of the greater trochanter, extending proximally. The fascia lata and gluteus maximus are split in line with their fibers.
2.
Entry Point:
The tip of the greater trochanter is identified. The entry point for the nail is crucial: typically, it is placed at or slightly medial to the tip of the greater trochanter, in line with the medullary canal on both AP and lateral views. This prevents varus malalignment or iatrogenic fracture.
*
Internervous Plane:
This approach generally avoids major neurovascular structures by splitting muscle fibers. The superior gluteal nerve innervates the gluteus medius and minimus, located more anteriorly.
3.
Reaming/Broaching:
Once the guide wire is accurately placed in the canal, the proximal femur is reamed (or broached, depending on nail system) to the appropriate diameter, allowing passage of the nail. Gentle technique is paramount to avoid iatrogenic fracture in osteoporotic bone.
Reduction:
*
Indirect Reduction:
Primarily achieved through traction and manipulation on the fracture table.
*
Length:
Traction is applied to restore limb length.
*
Rotation:
The limb is derotated until the patella points directly anterior.
*
Angulation:
Often addressed by judicious internal/external rotation and adduction/abduction of the limb, guided by fluoroscopy. For varus deformities, internal rotation and slight adduction may help.
*
Direct Reduction (Less Common):
If indirect methods fail, a percutaneous clamp or K-wire may be used, but this risks further soft tissue stripping and devitalization.
*
C-arm Confirmation:
AP and lateral views are critical at each step to confirm reduction adequacy. Ensure no malrotation, apex anterior/posterior angulation, or excessive varus/valgus.
Fixation (Cephalomedullary Nailing):
1.
Nail Insertion:
The chosen cephalomedullary nail is inserted into the medullary canal. Ensure the nail tip passes the fracture site without undue force.
2.
Lag Screw / Blade Insertion:
A guide wire for the cephalic screw (or blade) is inserted into the femoral head. Placement is critical: typically, central or slightly inferior on the AP view and central on the lateral view, aiming for the tip-apex distance (TAD) of <25mm. Optimal placement minimizes cut-out risk in osteoporotic bone.
*
Technique for Osteoporotic Bone:
Ensure the lag screw/blade has good purchase. Some systems allow for cement augmentation around the lag screw for enhanced stability in severely osteoporotic heads.
3.
Distal Locking:
Once the proximal fixation is complete, distal locking screws are inserted, typically using a targeting jig or freehand technique under fluoroscopy. One or two distal screws are usually sufficient.
Closure:
* Irrigation, hemostasis, closure of fascia, subcutaneous tissue, and skin in layers.
2. Distal Radius Fracture (Volar Locking Plate)
These are common fragility fractures, often intra-articular and comminuted, making stable fixation challenging in osteoporotic bone. Volar locking plates provide angular stability, which is highly advantageous.
Patient Positioning:
* Supine on the operating table with the arm extended on a radiolucent hand table. A tourniquet is applied to the upper arm. The C-arm is positioned for AP and lateral views of the wrist.
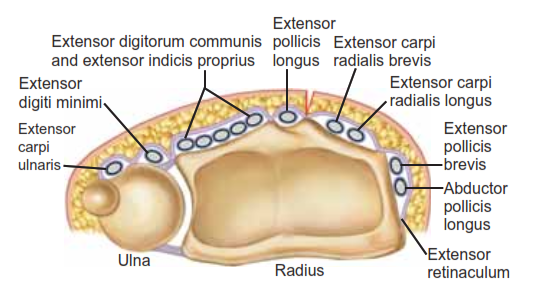
Surgical Approach (Volar Henry Approach):
1.
Incision:
A longitudinal incision is made along the volar aspect of the distal forearm, centered between the flexor carpi radialis (FCR) tendon and the radial artery.
2.
Dissection:
* The superficial fascia is incised.
* The FCR tendon sheath is opened and the FCR tendon retracted ulnarly.
* The radial artery is identified and retracted radially.
*
Internervous Plane:
The plane between the FCR (median nerve innervation) and the brachioradialis (radial nerve innervation) is utilized. The flexor pollicis longus (FPL) muscle and its median nerve branch (anterior interosseous nerve) are protected.
3.
Deep Dissection:
The pronator quadratus muscle is identified. Its ulnar insertion is released from the radius and the muscle is elevated radially, exposing the volar aspect of the distal radius. Careful release ensures protection of the anterior interosseous nerve, which runs on its dorsal surface.
Reduction:
*
Ligamentotaxis:
Traction is applied to the hand (manual or using finger traps) to help restore length and align fragments through tension on the intact ligaments.
*
Direct Reduction:
Use small pointed reduction clamps, K-wires, or small osteotomes/elevators to meticulously reduce articular fragments under direct visualization and fluoroscopic guidance.
*
Provisional K-wire Fixation:
Use temporary K-wires to stabilize reduced fragments.
*
C-arm Confirmation:
Confirm articular congruity and overall alignment on AP, lateral, and oblique fluoroscopic views.
Fixation (Volar Locking Plate):
1.
Plate Application:
The volar locking plate is positioned on the radial shaft, ensuring appropriate distal placement to support the articular fragments.
2.
Shaft Screw(s):
One or two non-locking cortical screws are typically inserted first into the diaphysis to provisional fix the plate to the bone, allowing for final plate positioning.
3.
Distal Locking Screws:
These are critical. They are inserted through the plate's locking holes into the osteoporotic epiphysis.
*
Technique for Osteoporotic Bone:
Ensure multiple, short, diverging locking screws are used to capture the articular fragments and provide maximum purchase in the weak bone. Screws are usually aimed at the subchondral bone to support the articular surface. Some plates allow for cement augmentation in extremely osteoporotic cases, though less common here than in the humerus.
4.
Proximal Locking Screws:
Once distal fixation is achieved, additional locking screws are placed proximally in the diaphysis.
5.
Final Checks:
Confirm reduction and fixation stability under fluoroscopy and direct visualization with full range of motion.
Closure:
* Reattach the pronator quadratus, irrigate, achieve hemostasis, and close the skin in layers.
Complications & Management
Management of fragility fractures in osteoporotic patients is associated with a unique set of complications, often exacerbated by advanced age, comorbidities, and the compromised nature of the bone. These complications can be broadly categorized into general surgical complications and those specific to fixation in osteoporotic bone.
General Surgical Complications (Exacerbated in Osteoporotic Population):
-
Systemic:
- Delirium: High incidence (up to 50% post-hip fracture). Management: early mobilization, pain control, hydration, avoidance of sedatives, reorientation, medical workup for underlying causes (infection, metabolic imbalance).
- Cardiopulmonary: Myocardial infarction, congestive heart failure, pneumonia, deep vein thrombosis (DVT), pulmonary embolism (PE). Management: pre-operative optimization, aggressive DVT prophylaxis (chemical and mechanical), early mobilization, chest physiotherapy.
- Urinary Tract Infection (UTI): Common. Management: early catheter removal, hydration, prompt antibiotic treatment.
- Pressure Ulcers: Due to immobility and fragile skin. Management: meticulous skin care, frequent repositioning, specialized mattresses.
-
Local:
- Infection (SSI): Higher risk due to comorbidities, prolonged surgery, and poor soft tissue envelope. Management: meticulous surgical technique, prophylactic antibiotics, debridement, targeted antibiotics, implant removal if necessary.
- Neurovascular Injury: Iatrogenic injury during dissection or reduction. Management: careful surgical technique, intra-operative monitoring, post-operative assessment, surgical repair if indicated.
Specific Complications of Fixation in Osteoporotic Bone:
| Complication | Incidence (Approximate) | Salvage Strategies |
|---|---|---|
| Implant Cut-Out / Pull-Out | 5-20% (Hip fractures) |
- Revision surgery with larger or different implant (e.g., conversion from dynamic hip screw to cephalomedullary nail or hemiarthroplasty for femoral neck fracture).
- Bone graft or cement augmentation. - If significant bone loss or severe osteoporosis, arthroplasty (hemi or total) is often the preferred salvage for hip/shoulder, or fusion for wrist/ankle. - Optimize patient's bone health with medical management. |
| Screw Loosening / Back-Out | Variable | - Similar to cut-out/pull-out. Often precursor to cut-out. May require revision with locking screws, augmentation, or conversion to arthroplasty. |
| Non-Union | 5-15% (Prox. Hum.) |
- Biological augmentation: bone grafting (autograft, allograft, DBM, BMPs).
- Mechanical stabilization: revision fixation with stronger, longer, or augmented implant (e.g., locked plate, IM nail). - Electrical or ultrasonic stimulation. - Consider systemic anabolic agents (e.g., teriparatide) if not already on medical management for osteoporosis. |
| Malunion | 10-30% (Distal Radius) |
- For symptomatic malunion causing functional deficit or pain: corrective osteotomy with internal fixation.
- For severe articular malunion: fusion or arthroplasty (e.g., wrist fusion). - Non-symptomatic malunion may be observed. |
| Periprosthetic Fracture | 1-5% (Hip arthroplasty) |
- Depends on location and stability:
Stable, non-displaced: Non-operative with protected weight-bearing. Unstable/displaced: Internal fixation (plates, cerclage wires, cables, revision stems). - Often requires augmentation due to pre-existing osteoporotic bone. |
| Avascular Necrosis (AVN) | 10-30% (Femoral Neck) | - For significant AVN with collapse of femoral head: Arthroplasty (hemi- or total hip replacement) is the standard salvage. Core decompression is not effective in established AVN with collapse. |
| Hardware Impingement / Prominence | Variable | - Surgical removal of symptomatic hardware after fracture union. If necessary for stability, plate replacement or adjustment. |
| Refracture | 5-10% (after union) | - Re-operation with repeat fixation or arthroplasty. Crucially, emphasize comprehensive medical management of osteoporosis post-fracture to reduce future fracture risk (secondary fracture prevention). Fall prevention strategies are also paramount. |
| Loss of Reduction | 5-15% | - Usually indicates inadequate initial fixation or severe bone comminution. May require revision surgery to achieve better fixation, often with augmentation, or conversion to an alternative implant (e.g., from plate to nail, or internal fixation to arthroplasty). Reinforce post-operative rehabilitation adherence and weight-bearing restrictions if non-operative component. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation in osteoporotic fragility fracture patients is a critical determinant of functional outcome and overall recovery. Protocols must be carefully tailored, considering the inherent bone fragility, patient comorbidities, and the specific fixation achieved. The overarching goals are to restore function, prevent complications, and integrate secondary fracture prevention strategies.
Immediate Post-Operative Phase (Days 0-7):
- Pain Management: Aggressive, multimodal pain management (opioids, NSAIDs, acetaminophen, nerve blocks) is crucial to facilitate early mobilization and prevent delirium.
-
Early Mobilization:
As soon as medically stable and fixation allows. This is paramount to prevent DVT/PE, pneumonia, pressure ulcers, and deconditioning.
- Hip Fractures: For stable internal fixation or arthroplasty, typically weight-bearing as tolerated (WBAT) immediately, unless specific contraindications (e.g., unstable fixation, certain reverse total shoulder arthroplasties). Early transfer to a chair, ambulation with assistance (walker, crutches).
- Distal Radius: Early active and passive range of motion of the elbow, shoulder, and digits. Wrist immobilization (splint or cast) is maintained, with protected wrist motion potentially starting at 2-4 weeks.
- Proximal Humerus: Shoulder immobilization in a sling for 4-6 weeks, with pendulum exercises and gentle passive external rotation permitted early to prevent stiffness. Active range of motion and strengthening deferred until radiographic evidence of healing.
- Physical and Occupational Therapy: Initiate daily sessions focusing on transfers, gait training, activities of daily living (ADLs), and functional mobility.
- DVT Prophylaxis: Continue chemical (anticoagulants) and mechanical (SCDs) prophylaxis according to institutional guidelines.
- Nutritional Support: Optimize protein and caloric intake to support wound healing and recovery.
- Delirium Monitoring: Continuous monitoring and proactive management of risk factors.
Intermediate Phase (Weeks 2-12):
-
Progressive Weight-Bearing / Motion:
- Hip Fractures: Continue WBAT with progressive reduction in assistive devices as strength and balance improve.
- Distal Radius: Transition from immobilization to protected range of motion exercises for the wrist, gradually increasing intensity. Strengthening initiated as pain allows and radiographic healing progresses (typically 6-8 weeks).
- Proximal Humerus: Gradually progress from passive to active-assisted range of motion, then to gentle active range of motion, strictly adhering to surgeon-specified limitations based on fracture pattern and fixation stability. Strengthening typically begins at 8-12 weeks.
- Balance & Proprioception Training: Essential to reduce future fall risk.
- Strengthening: Focused exercises for hip abductors, quadriceps, gluteal muscles (for lower extremity fractures); rotator cuff, deltoid, grip strength (for upper extremity fractures).
- Functional Training: Reintegrate ADLs, return to leisure activities.
- Radiographic Follow-up: Regular radiographs (e.g., at 2, 6, 12 weeks) to monitor fracture healing and implant integrity.
Advanced Phase (Months 3+):
- Return to Full Activities: Gradual return to pre-injury activity levels, avoiding high-impact activities if bone density remains compromised.
- Ongoing Strengthening & Conditioning: Maintenance exercise program focusing on strength, endurance, balance, and flexibility.
-
Secondary Fracture Prevention:
- Bone Mineral Density (BMD) Assessment: If not already performed, DEXA scan should be obtained to quantify osteoporosis severity.
- Medical Management: Initiate or optimize anti-osteoporosis medications (bisphosphonates, denosumab, teriparatide, romosozumab) as indicated, in consultation with an endocrinologist or primary care physician. Ensure adequate calcium and vitamin D intake.
- Fall Risk Assessment & Prevention: Comprehensive assessment of intrinsic (gait, balance, vision, polypharmacy) and extrinsic (environmental hazards) fall risks. Referrals to physical therapy for specialized balance programs, ophthalmology, medication review, home safety modifications.
- Lifestyle Modification: Encourage weight-bearing exercise, smoking cessation, and moderation of alcohol intake.
Summary of Key Literature / Guidelines
The management of osteoporosis and its related fragility fractures is guided by a robust body of literature and numerous clinical guidelines from prominent orthopedic and medical societies. These emphasize a multidisciplinary approach encompassing surgical stabilization, medical optimization, and long-term osteoporosis management.
-
American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines:
- Management of Hip Fractures in Older Adults: Strongly recommends early surgical intervention (within 48 hours) for most hip fractures, often with weight-bearing as tolerated post-operatively. Advocates for multimodal pain management and DVT prophylaxis. Emphasizes the importance of multidisciplinary care.
- Management of Distal Radius Fractures: Provides guidance on acceptable radiographic parameters for non-operative treatment and indications for surgical intervention (articular incongruity, significant displacement, instability).
- Management of Proximal Humerus Fractures: Outlines indications for non-operative vs. operative management based on fracture displacement, comminution, and patient factors, with increasing recognition of reverse total shoulder arthroplasty for complex fractures in older, osteoporotic patients.
-
National Osteoporosis Foundation (NOF) Clinician's Guide to Prevention and Treatment of Osteoporosis:
- This guideline provides comprehensive recommendations on diagnosing osteoporosis (DEXA scanning), assessing fracture risk (FRAX tool), and initiating pharmacologic treatment. It stresses the importance of adequate calcium and vitamin D intake and lifestyle modifications. Crucially, it highlights that any fragility fracture is an indication for osteoporosis evaluation and treatment.
-
International Osteoporosis Foundation (IOF) / European Federation of National Associations of Orthopaedics and Traumatology (EFORT) Position Papers:
- These international bodies consistently advocate for secondary fracture prevention strategies, including systematic identification of patients with fragility fractures (Fracture Liaison Services - FLS) to ensure they receive appropriate bone health evaluation and treatment. They emphasize that orthopedic surgeons are uniquely positioned to initiate this process.
-
Geriatric Orthopaedic Surgery & Rehabilitation Journal / JBJS / JOT:
- Recent literature in these journals continues to refine surgical techniques, implant designs (e.g., cement augmentation of screws, newer locking plate designs), and rehabilitation protocols specifically for osteoporotic bone. There's a growing focus on cost-effectiveness, quality of life metrics, and the prevention of subsequent fractures. Studies often compare different fixation methods, outcomes of arthroplasty vs. internal fixation, and the impact of pre- and post-operative medical management.
-
Cochrane Reviews:
- Provide evidence-based syntheses of interventions for fragility fractures, such as comparisons of different types of internal fixation, arthroplasty, and non-operative management, often highlighting areas requiring further research and informing guideline development.
In summary, the key takeaways from current literature and guidelines underscore that the orthopedic surgeon's role extends beyond acute fracture fixation to include a proactive approach to identifying and managing the underlying osteoporosis, collaborating with medical colleagues, and ensuring comprehensive rehabilitation and secondary fracture prevention. This integrated approach is essential to mitigate the significant individual and societal burden of fragility fractures.
You Might Also Like