Doctors: Proximal Humeral Fractures - Master Reverse Arthroplasty Technique

Key Takeaway
Learn more about Doctors: Proximal Humeral Fractures - Master Reverse Arthroplasty Technique and how to manage it. Doctors recommend reverse shoulder arthroplasty for complex proximal humeral fractures, particularly in elderly patients with displaced four-part fractures or comminuted tuberosities. This procedure, which doesn't rely on rotator cuff function, provides predictable pain relief and improved shoulder function where tuberosity healing is problematic. Key to success involves precise surgical landmarks, extensive soft tissue release, and stable tuberosity fixation.
Doctors: Proximal Humeral Fractures - Master Reverse Arthroplasty Technique
Introduction & Epidemiology
Proximal humeral fractures (PHF) represent a significant burden on healthcare systems, accounting for approximately 5-6% of all fractures, with a markedly increased incidence in the elderly population due to osteoporosis. The demographic shift towards an aging population suggests this incidence will continue to rise. While the majority of PHFs are minimally displaced and can be managed non-operatively, a substantial proportion, particularly complex, multi-fragmentary fracture patterns (Neer three- and four-part fractures), present considerable surgical challenges.
Traditional surgical management options for displaced PHFs have included open reduction and internal fixation (ORIF) with plates and screws, and hemiarthroplasty. However, ORIF in severely osteoporotic bone is frequently associated with complications such as screw cutout, loss of reduction, nonunion, and avascular necrosis (AVN) of the humeral head, particularly when tuberosity comminution compromises blood supply. Hemiarthroplasty, while addressing the humeral head, often yields unpredictable functional outcomes primarily due to the inconsistent healing and function of the tuberosities and their attached rotator cuff musculature. Poor tuberosity healing in hemiarthroplasty significantly impairs active elevation and external rotation, leading to limited function and persistent pain.
Reverse shoulder arthroplasty (RSA) has emerged as an increasingly attractive and effective surgical solution for complex PHFs in elderly patients, particularly those with compromised bone quality, rotator cuff deficiency, or significant tuberosity comminution. By medializing and distalizing the center of rotation and utilizing the deltoid muscle as the primary elevator of the arm, RSA bypasses the critical reliance on a functional rotator cuff and well-healed tuberosities, offering more predictable pain relief and functional restoration compared to hemiarthroplasty. The expanding indications for RSA in PHF underscore its growing role in the armamentarium of the orthopedic surgeon.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the shoulder joint is paramount for successful RSA in the setting of PHF.
Surgical Anatomy
- Proximal Humerus : The proximal humerus comprises the humeral head, anatomical neck, surgical neck, greater tuberosity (insertion of supraspinatus, infraspinatus, teres minor), lesser tuberosity (insertion of subscapularis), and the bicipital groove. Fracture patterns are typically described relative to these anatomical landmarks. The blood supply to the humeral head is predominantly via the anterior and posterior circumflex humeral arteries, with critical contributions from the ascending branch of the anterior circumflex artery. Comminution of the tuberosities often disrupts this vascularity, predisposing to AVN.
- Rotator Cuff : Consists of the supraspinatus, infraspinatus, teres minor, and subscapularis. These muscles stabilize the glenohumeral joint and contribute to rotation and abduction. In PHF, these tendons can be avulsed with the tuberosity fragments, making their repair critical for restoring a more anatomical function, even in RSA.
- Deltoid Muscle : The deltoid muscle is the primary abductor and flexor of the shoulder. In RSA, its integrity and tension are crucial as it becomes the main elevator of the arm, compensating for a deficient rotator cuff. The deltoid is innervated by the axillary nerve.
-
Neurovascular Structures
:
- Axillary Nerve : Courses inferior to the humeral head, winding around the surgical neck, supplying the deltoid and teres minor. It is highly susceptible to injury during the surgical approach, particularly with inferior humeral displacement or aggressive retraction.
- Musculocutaneous Nerve : Pierces the coracobrachialis, providing motor innervation to the biceps and coracobrachialis.
- Brachial Plexus : Superior to the axillary artery and vein, lies medially in the deltopectoral interval.
- Axillary Artery and Vein : Lie medial to the coracobrachialis and short head of the biceps.
- Anterior and Posterior Circumflex Humeral Arteries : Branches of the axillary artery, supplying the humeral head and deltoid.
- Careful dissection and meticulous hemostasis are critical to avoid iatrogenic injury.
Biomechanics of Reverse Shoulder Arthroplasty
RSA fundamentally alters the shoulder's biomechanics by converting the convex humeral head and concave glenoid relationship to a concave humerus and convex glenoid (glenosphere). This design principle, pioneered by Grammont, offers several key advantages in the setting of PHF with rotator cuff compromise:
- Medialization and Distalization of the Center of Rotation : The center of rotation is moved medially towards the glenoid and distalized, increasing the deltoid's lever arm. This allows the deltoid to effectively elevate the arm even in the absence of a functional rotator cuff.
- Increased Deltoid Tension : Distalization of the humeral component increases deltoid tension, improving its efficiency and contributing to joint stability. However, excessive tension can lead to scapular notching, axillary nerve stretch, or deltoid dysfunction.
- Enhanced Stability : The large glenosphere and deep humeral cup provide inherent stability, reducing the risk of dislocation often seen with hemiarthroplasty in fracture settings.
- Tuberosity Function : While RSA does not rely on rotator cuff function for elevation, successful healing of the tuberosities, particularly the greater tuberosity, significantly improves active external rotation, which can be profoundly limited otherwise. The subscapularis, if repaired, also contributes to internal rotation and anterior stability.
- Offset : Glenoid-sided and humeral-sided offsets influence range of motion, stability, and deltoid tension. Proper selection is critical to prevent impingement and ensure optimal function.
Indications & Contraindications
The indications for reverse shoulder arthroplasty in proximal humeral fractures are evolving, reflecting improved implant designs and surgical techniques.
Indications
- Displaced Four-Part Fractures : This remains the classic indication, especially in elderly patients with osteoporotic bone and significant comminution of the humeral head and tuberosities where anatomical reduction and stable fixation are unlikely.
- Displaced Three-Part Fractures : Increasingly considered, particularly when there is significant comminution of the tuberosities, poor bone quality, or suspicion of pre-existing rotator cuff pathology.
- Fracture-Dislocations : Complex cases involving both a fracture and dislocation, especially if the humeral head is significantly compromised or chronic dislocation makes reduction difficult.
- Fractures with Pre-existing Rotator Cuff Arthropathy : If the patient has documented cuff tear arthropathy prior to the fracture, RSA is a superior option.
- Failed Open Reduction and Internal Fixation (ORIF) : Cases of primary ORIF failure due to nonunion, malunion, implant cutout, or severe AVN of the humeral head.
- Failed Hemiarthroplasty : Persistent pain and poor function following hemiarthroplasty, often due to tuberosity nonunion or malunion.
- Elderly Patients (>70-75 years) : Patients with low functional demands and significant osteoporosis who would likely have poor outcomes with ORIF due to bone quality.
- Specific Fracture Patterns : Such as those with very small or highly comminuted tuberosity fragments that are unsuitable for stable fixation.
More recently, even certain two-part surgical neck fractures may be considered in the elderly, particularly those with poor bone stock or existing rotator cuff issues, to provide a more predictable outcome.
Contraindications
- Active Infection : Absolute contraindication. Infection must be eradicated prior to arthroplasty.
- Non-functional Deltoid Muscle : The deltoid is the primary motor for RSA. Axillary nerve palsy or severe deltoid muscle compromise (e.g., extensive scarring, avulsion) contraindicates RSA.
- Significant Glenoid Bone Loss : Insufficient glenoid bone stock to securely fix the glenoid baseplate, which could lead to early loosening.
- Unrealistic Patient Expectations : Patients must understand the goals of the surgery (pain relief, functional improvement, not necessarily return to high-impact activities).
- Young, Active Patients : Relative contraindication. In younger, more active individuals, attempts to preserve the native joint or perform complex ORIF are often preferred, reserving RSA for salvage or specific situations.
- Severe Medical Comorbidities : Patients with comorbidities that significantly increase surgical risk and outweigh the potential benefits of the procedure.
Operative vs. Non-Operative Indications
The decision-making process for managing proximal humeral fractures involves careful patient selection and fracture characterization.
| Indication Type | Non-Operative Management | Operative Management (RSA) |
|---|---|---|
| Fracture Pattern | Minimally displaced 1- and 2-part fractures | Displaced 3- and 4-part PHF (Neer classification) |
| Stable impacted fractures | Fracture-dislocations | |
| Bone Quality | Good bone stock, stable fragments | Severe osteoporosis, comminuted tuberosities |
| Patient Age | Any age, typically younger or very elderly with low demand | Generally elderly (>70-75 years) |
| Functional Demand | Low functional demand, sedentary lifestyle | Moderate to high functional demand for ADLs |
| Rotator Cuff Status | Intact rotator cuff | Pre-existing rotator cuff arthropathy, suspected tear |
| Associated Injuries | No significant neurovascular compromise | Failed ORIF or Hemiarthroplasty |
| Significant articular damage or humeral head AVN | ||
| Primary indication in certain complex 2-part fractures |
Pre-Operative Planning & Patient Positioning
Careful pre-operative planning and meticulous patient positioning are crucial for successful reverse shoulder arthroplasty in the setting of proximal humeral fractures.
Patient Preparation
- History and Physical Examination : Obtain a comprehensive medical history, focusing on comorbidities, medications, and previous shoulder pathologies. Assess skin integrity, neurological status (specifically axillary nerve function), and vascular supply. Document baseline range of motion and pain levels.
-
Imaging
:
- Standard Radiographs : AP (true glenoid view), scapular Y, and axillary views are essential to define the fracture pattern and glenohumeral relationship.
- Computed Tomography (CT) Scan : Crucial for evaluating fracture comminution, particularly tuberosity involvement, humeral head impaction, and glenoid bone stock. 3D reconstructions are invaluable for pre-operative visualization and surgical templating.
- Magnetic Resonance Imaging (MRI) : May be considered if there is suspicion of pre-existing rotator cuff pathology that would influence surgical decision-making, though often not necessary in acute fractures directly proceeding to RSA.
- Templating : Utilize digital templating software with the CT images to plan glenoid baseplate size, screw length, glenosphere size, humeral stem size and type (cemented vs. uncemented), and humeral tray offset. This aids in anticipating challenges and selecting appropriate implant components.
- Medical Optimization : Optimize all chronic medical conditions (e.g., diabetes, hypertension, cardiac disease) to minimize surgical risks. Pre-operative cardiac clearance and blood work are standard.
- Informed Consent : Thoroughly discuss the procedure, potential benefits (pain relief, improved function for activities of daily living), risks (infection, neurovascular injury, dislocation, tuberosity nonunion, glenoid loosening, scapular notching), and the prolonged rehabilitation process.
- Anesthesia : A general anesthetic is typically combined with an interscalene brachial plexus block for post-operative pain management.
Patient Positioning
-
Beach Chair Position : This is the most common position for RSA.
- The patient is placed in a semi-recumbent position at approximately 30-45 degrees, similar to a deck chair.
- The head is secured in a well-padded headrest, ensuring the neck is neutral to prevent brachial plexus stretch.
- The surgical arm is draped free to allow full manipulation during the procedure.
- The back of the patient should be elevated off the operating table using a support system to facilitate access for the surgeon and allow for easy arm adduction.
- Ensure appropriate padding for all pressure points (sacrum, heels, elbows, contralateral arm).
- Image Intensifier : Positioned to allow intraoperative AP and axillary views of the glenoid and humerus without repositioning the patient.
- A rolled towel or small bump can be placed between the scapula and the operating table to protract the scapula slightly, improving access to the glenoid.
-
Lateral Decubitus Position : Less commonly used for primary RSA in PHF but may be considered in specific circumstances or for revision cases. Requires meticulous padding and stabilization.
-
Preparation and Draping :
- The entire shoulder, upper extremity (to the fingertips), and axilla are prepped with an antiseptic solution.
- Sterile stockinettes and drapes isolate the arm, allowing it to be manipulated independently.
- The draping should provide a wide sterile field for potential exposure extension if needed.
Detailed Surgical Approach / Technique
The goal of reverse shoulder arthroplasty in proximal humeral fractures is to restore stable glenohumeral articulation, maximize deltoid function, and facilitate tuberosity healing where possible, to optimize pain relief and functional outcomes.
1. Incision and Approach
-
Incision
: A standard deltopectoral incision is utilized. Begin at the junction of the acromion and clavicle, extending distally along the deltopectoral groove for approximately 10-15 cm.
-
Deltopectoral Interval
: Identify the deltopectoral groove. The cephalic vein, typically residing within this interval, should be identified and retracted laterally with the deltoid. In some cases, it may need to be ligated and divided if it impedes exposure or is damaged.
- Subdeltoid Space : Develop the subdeltoid space by releasing adhesions and hematoma. Careful dissection is paramount to protect the axillary nerve, which lies approximately 5-7 cm distal to the acromial edge.
- Clavipectoral Fascia : Incise the clavipectoral fascia medial to the deltoid, exposing the underlying conjoined tendon (coracobrachialis and short head of biceps).
- Subscapularis : For non-fracture cases, the subscapularis tendon is typically released. In PHF, the subscapularis is often avulsed with the lesser tuberosity and may be retracted medially. Its integrity and position need to be assessed.
2. Fracture Exposure and Initial Assessment
- Remove hematoma and clear loose bone fragments. Identify the humeral head fragment, greater tuberosity, lesser tuberosity, and humeral shaft.
- Due to the often chaotic nature of fracture anatomy, it can be challenging to reliably orient the humeral head fragment. Focus on identifying stable landmarks.
- The humeral head fragment is typically avascular. If it is large enough, it may be used as a template for glenoid preparation or removed.
- In cases of severe comminution, the humeral head may be piecemeal or entirely fragmented.
- Manage tuberosity fragments meticulously; they are crucial for post-operative external rotation and should be carefully débrided of soft tissue but preserved for potential repair.
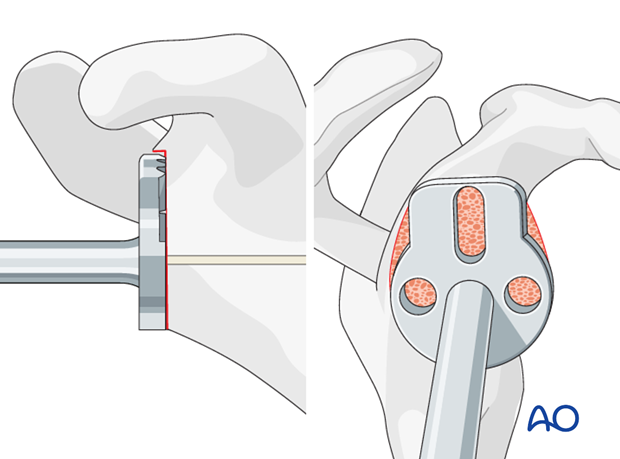
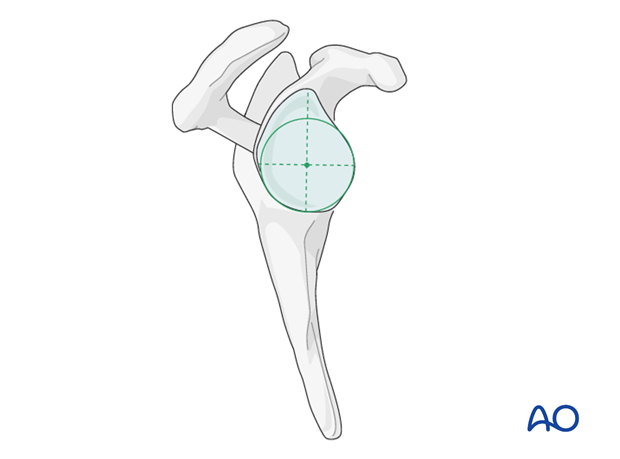
3. Glenoid Preparation
- Exposure : Retract the humeral shaft inferiorly and laterally. Release the anterior capsule and labrum from the glenoid rim as necessary. The assistant typically applies downward and external rotation traction to expose the glenoid.
- Coracoid Process : In some cases, a partial release of the coracoid process (from the subscapularis and conjoined tendon) or a coracoid osteotomy may be required for optimal glenoid exposure, though less commonly necessary for fracture cases if the humerus is disarticulated.
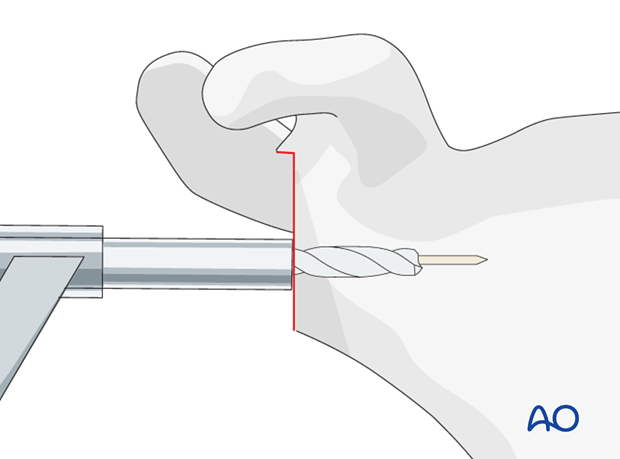
-
Glenoid Reaming
:
- Identify the anatomical glenoid surface.
- Place a central guide pin, ensuring appropriate version and inclination. Typically, neutral to slight retroversion (0-10 degrees) and neutral inclination are desired.
-
Ream the glenoid to a flat, raw cancellous bone surface using sequential reamers. Ensure adequate bone stock, particularly inferiorly, to prevent scapular notching.
- Ream to ensure the baseplate will sit flush and provide stable fixation.
-
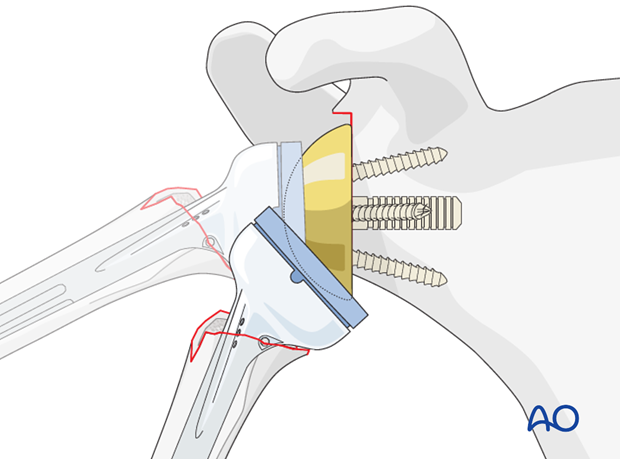
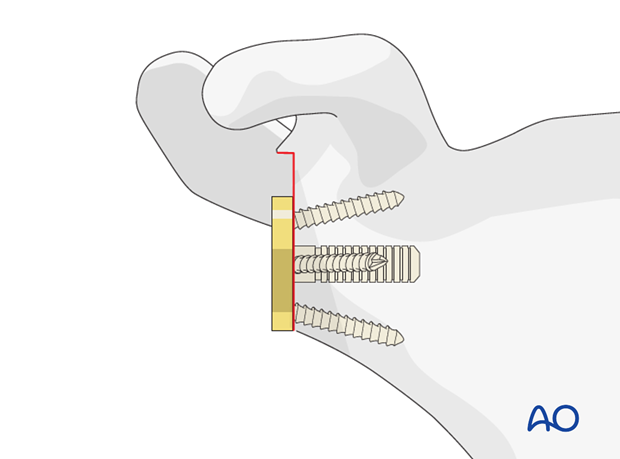
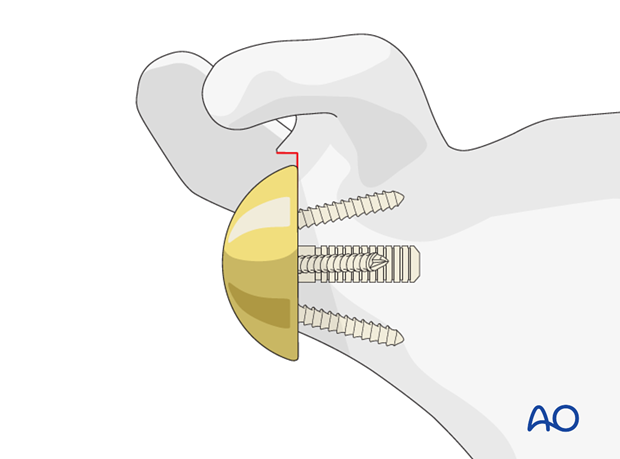
Baseplate Fixation
:
- Select the appropriate size of the glenoid baseplate.
- Position the baseplate on the reamed glenoid surface.
- Secure the baseplate with a central compression screw (locking or non-locking).
-
Insert peripheral locking screws to achieve rigid fixation. Ensure screws are bicortical where possible and do not violate the glenoid vault.
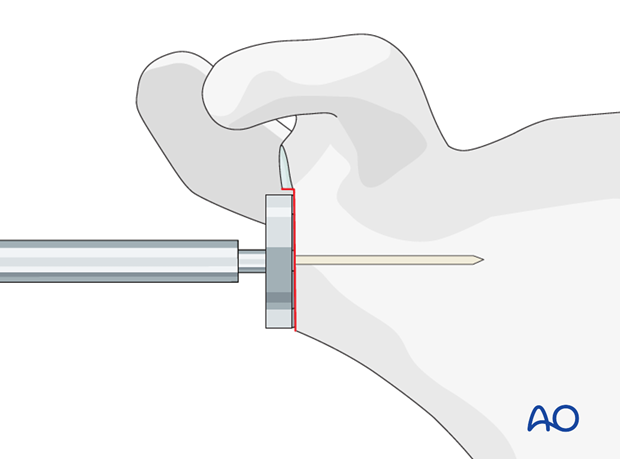
- Confirm stability with fluoroscopy and manual assessment.
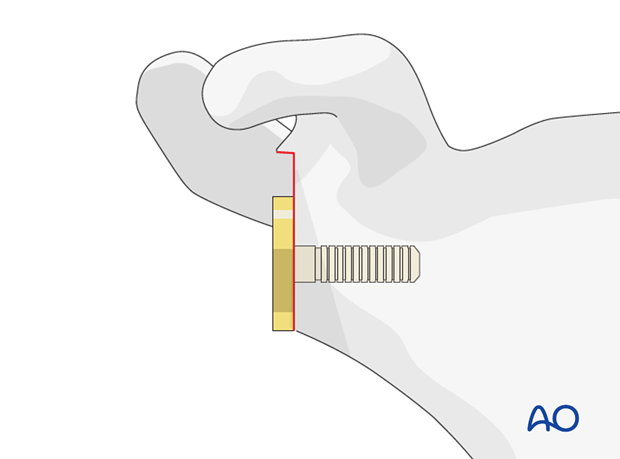
-
Glenosphere Placement
:
-
Attach the trial glenosphere to the baseplate. The size of the glenosphere (e.g., 36mm, 40mm, 42mm) influences stability, range of motion, and scapular notching risk. A larger glenosphere typically provides greater stability and may allow for more distalization of the humerus.
-
Attach the trial glenosphere to the baseplate. The size of the glenosphere (e.g., 36mm, 40mm, 42mm) influences stability, range of motion, and scapular notching risk. A larger glenosphere typically provides greater stability and may allow for more distalization of the humerus.
4. Humeral Preparation
- Humeral Head Resection : If a large, displaced humeral head fragment is present, it is often removed. In many comminuted fractures, the head is already fragmented or absent.
-
Medullary Canal Preparation
:
- Identify the humeral shaft.
- Use an intramedullary guide wire to establish the axis of the humeral shaft.
- Progressively ream the humeral canal to the desired depth and diameter, matching the chosen humeral stem.
-
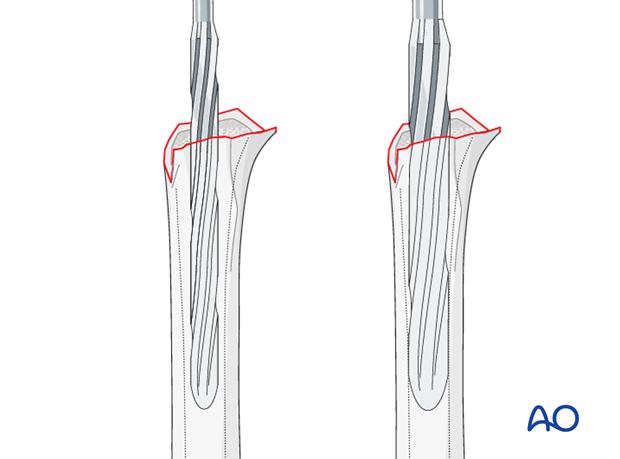
Protect the greater tuberosity during reaming and broaching, as it should be preserved for reattachment.
-
Humeral Broaching/Trial Stem
:
- Broach the canal to create the appropriate metaphyseal fit for the stem.
- Insert a trial humeral stem.
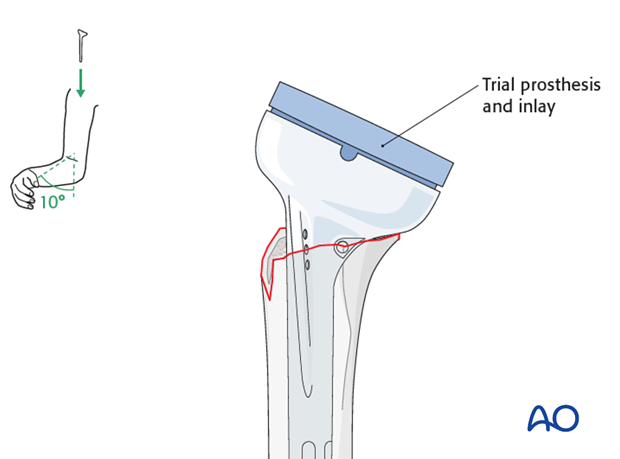
-
Attach the appropriate trial humeral tray/liner. The height and offset of the humeral component are critical for soft tissue tension and deltoid efficiency. Aim for approximately 2-3 cm distalization relative to the native joint line.
-
Keys to successful reverse shoulder arthroplasties (reiterated from seed content):
- Correct determination of the surgical landmarks
- Extensive soft tissue release
- Proper determination of prosthesis size and version
- Proper height of the prosthesis with correct soft-tissue tensions
- Stable fixation of the tuberosities to promote their union to the proximal humerus
5. Trial Reduction and Final Implantation
-
Perform a trial reduction with the trial glenosphere and humeral components.
- Assess stability through a full range of motion. Check for impingement, dislocation, and appropriate deltoid tension. The arm should reduce without excessive force and remain stable.
- Make adjustments to component size (glenosphere, humeral tray height, offset) as needed to optimize stability and soft tissue tension.
- Once satisfactory trial reduction is achieved, remove trial components.
-
Insert the definitive humeral stem (cemented or uncemented).
-
Impact the definitive humeral polyethylene liner onto the stem or the definitive humeral component.
-
Connect the definitive glenosphere to the baseplate.
-
Reduce the final components.
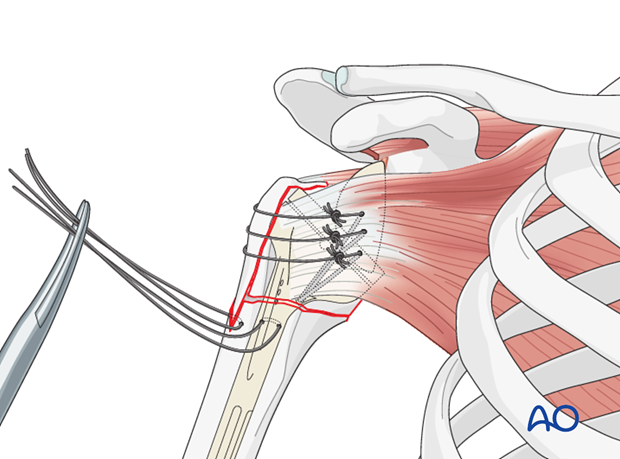
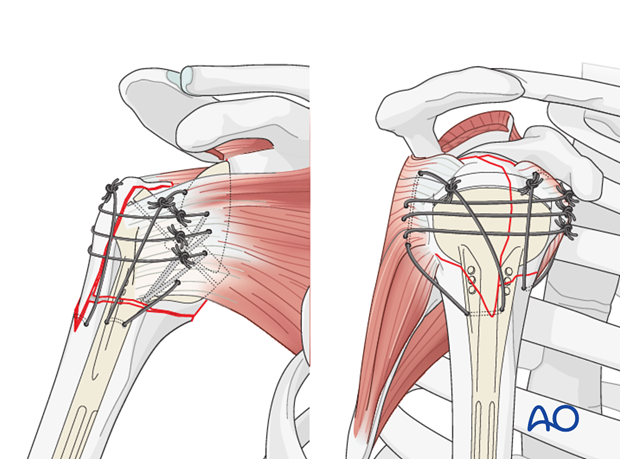
6. Tuberosity Repair
- This is a critical step for maximizing functional outcomes, particularly external rotation.
- Gather the greater and lesser tuberosity fragments. Débride any necrotic soft tissue or cartilage.
- Use heavy non-absorbable sutures (e.g., #5 Ethibond or FiberWire) to repair the tuberosities around the humeral stem.
-
Employ cerclage wires or suture anchors through the tuberosities and into the metaphyseal bone of the humeral shaft, securing them anatomically around the stem. This provides a soft tissue envelope and improves external rotation.
- Confirm stable fixation. While achieving perfect anatomical reduction can be challenging in comminuted fractures, stable biological fixation is the goal.
7. Closure
- Perform meticulous hemostasis.
- Irrigate the wound thoroughly.
- Consider drain placement (e.g., suction drain) if significant oozing is present, removing it within 24-48 hours.
- Close the deltopectoral interval.
- Close the subcutaneous layers and skin.
- Apply a sterile dressing and place the arm in an abduction sling or sling with an abduction pillow.
Complications & Management
While RSA offers predictable outcomes for pain relief and functional improvement in PHF, it is not without potential complications. A comprehensive understanding of these complications and their management strategies is essential.
Common Complications
- Infection : Periprosthetic joint infection (PJI) is a devastating complication, with incidence rates varying but generally ranging from 1% to 5%. Risk factors include advanced age, comorbidities (e.g., diabetes), prolonged operative time, and previous surgeries.
-
Neurovascular Injury
:
- Axillary Nerve Injury : The most common nerve injury, occurring in 1-10% of cases. Typically a neuropraxia due to stretch or retraction, but direct injury is possible. Manifests as deltoid weakness/palsy and numbness over the lateral shoulder.
- Brachial Plexus Injury : Less common but more severe, usually related to traction or malpositioning.
- Vascular Injury : Rare, but direct damage to the axillary artery or vein can lead to significant hemorrhage.
- Glenoid Component Loosening/Failure : Aseptic loosening of the glenoid baseplate can occur due to poor initial fixation, stress shielding, or osteolysis. Incidence varies from 2-10%.
- Humeral Component Loosening/Periprosthetic Fracture : Less common than glenoid loosening. Fractures can occur intraoperatively during stem insertion or post-operatively, often at the tip of the stem.
- Scapular Notching : Impingement of the humeral polyethylene liner on the inferior scapular neck, leading to bone erosion. More prevalent with earlier Grammont-style designs. Incidence has decreased with modified designs and eccentric glenospheres but remains a concern.
- Dislocation/Instability : Occurs in 2-5% of cases. Risk factors include component malposition, inadequate soft tissue tension, and poor patient compliance with post-operative restrictions.
- Tuberosity Nonunion/Malunion : Despite attempts at repair, tuberosity healing remains challenging in fracture RSA, with nonunion rates often reported between 20-50%. While RSA does not rely on tuberosity healing for basic function, successful union significantly improves active external rotation and cosmetic contour.
- Heterotopic Ossification (HO) : Abnormal bone formation in soft tissues around the joint, particularly in the deltoid. Can restrict range of motion.
- Hematoma Formation : Post-operative bleeding leading to hematoma, potentially requiring drainage.
Management Strategies
| Complication | Incidence (%) (approx.) | Salvage Strategy |
|---|---|---|
| Periprosthetic Infection | 1-5 | Acute (<3 weeks): Debridement, antibiotics, implant retention (DAIR) if stable. Chronic (>3 weeks): Two-stage revision (implant removal, spacer, antibiotics, then reimplantation), or single-stage revision in highly selected cases. Girdlestone shoulder (excision arthroplasty) as last resort. |
| Axillary Nerve Injury | 1-10 | Neuropraxia: Observation, electrodiagnostic studies (EMG/NCS) at 3-6 weeks. Neurotmesis/Axonotmesis: Surgical exploration, neurolysis, nerve graft, or tendon transfer (e.g., latissimus dorsi) for persistent deficits. |
| Glenoid Loosening | 2-10 | Revision to a larger baseplate, augmented baseplate, bone grafting for defects, custom glenoid implant, or conversion to hemiarthroplasty/excision arthroplasty if severe bone loss. |
| Humeral Loosening | <2 | Revision to a longer or larger stem (cemented or uncemented), often with bone grafting. |
| Periprosthetic Fracture | 1-3 | Intraoperative: Revision to a longer stem, cerclage wiring, or plate fixation. Postoperative: ORIF with plate/screws and cerclage, or revision arthroplasty depending on stability and location. |
| Scapular Notching | 10-20 (variable) | Asymptomatic: Observation. Symptomatic: Conservative management, activity modification. Severe/Progressive: Glenoid revision with larger glenosphere, more eccentric glenosphere, or bone grafting (rare). |
| Dislocation | 2-5 | Acute: Closed reduction. Recurrent: Surgical exploration, assessment of component position, soft tissue tension, glenosphere size/offset, liner constraint. Revision of components or soft tissue repair. |
| Tuberosity Nonunion | 20-50 | Asymptomatic: Observation. Symptomatic (poor external rotation): Conservative management. Surgical options include latissimus dorsi or pectoralis major transfer (for external rotation), or revision to a different stem design allowing better tuberosity coverage. |
| Heterotopic Ossification | 5-10 | Prophylaxis: NSAIDs (e.g., Indomethacin) or radiation therapy in high-risk patients. Symptomatic: Excision of HO if mature and significantly limiting range of motion after 6-12 months. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following reverse shoulder arthroplasty for proximal humeral fractures is a critical determinant of functional outcome. The protocol must balance protecting the healing tuberosities and soft tissues with initiating early, controlled motion to prevent stiffness and optimize deltoid function. The specific protocol will vary based on surgeon preference, implant stability, and the quality of tuberosity repair.
General Principles
- Protection : Primary focus initially is protecting the surgical repair, especially the tuberosities.
- Early Motion : Gradual, controlled range of motion to prevent stiffness and promote articular cartilage health.
- Deltoid Engagement : Early activation of the deltoid, as it is the primary motor.
- Progressive Strengthening : Gradual increase in strength and functional demands.
- Individualization : Protocols should be tailored to individual patient factors, fracture severity, and surgical findings (e.g., quality of tuberosity repair).
Phased Rehabilitation Protocol
Phase 1: Immobilization and Passive Motion (Weeks 0-6)
- Goals : Protect surgical repair, minimize pain, initiate early passive range of motion.
- Immobilization : Arm maintained in an abduction sling or sling with an abduction pillow (10-30 degrees of abduction) for comfort and to minimize stress on tuberosity repairs. Remove sling for exercises and hygiene only.
-
Motion
:
- Pendulum Exercises : Begin gentle pendulum exercises within pain limits (day 1-3 post-op).
-
Passive Range of Motion (PROM)
: Initiated by a therapist or family member, avoiding active muscle contraction.
- Forward Elevation (Scaption) : To 90-120 degrees, respecting pain and soft tissue tension.
- External Rotation : Restricted initially (0-10 degrees, often sling-dependent) to protect greater tuberosity repair. If no tuberosity repair, may allow more, but generally limited to 20-30 degrees.
- Internal Rotation : To chest/abdomen.
- Elbow, Wrist, Hand : Active range of motion and strengthening exercises for the elbow, wrist, and hand.
- Activities : No active lifting, pushing, pulling, or sudden movements. No weight-bearing through the operated arm. Avoid hyperextension or forceful external rotation.
- Patient Education : Emphasize proper body mechanics and activity restrictions.
Phase 2: Active-Assisted & Gentle Active Motion (Weeks 6-12)
- Goals : Gradual increase in range of motion, initiate deltoid activation, improve scapular control.
- Immobilization : Discontinue sling use as comfort allows, typically by 6 weeks, except for sleeping or in crowded environments.
-
Motion
:
- Active-Assisted Range of Motion (AAROM) : Progress from PROM to AAROM for forward elevation, external rotation (gradual increase, still cautious with tuberosity repair), and internal rotation.
- Gentle Active Range of Motion (AROM) : Begin unassisted active motion as tolerated, focusing on controlled movements.
- Scapular Stabilization Exercises : Initiate isometric scapular retraction and depression exercises.
-
Strengthening
:
- Isometric Exercises : Gentle isometric contractions of the deltoid, biceps, and triceps with the arm in neutral positions.
- Rotator Cuff (if tuberosities healed) : If tuberosity healing is confirmed (clinically and/or radiographically), gentle isometric and very light resistance exercises for external and internal rotators can begin.
- Activities : Continue to avoid heavy lifting (>5 lbs), sudden movements, or activities that place undue stress on the shoulder. May begin light functional activities with the arm below shoulder height.
Phase 3: Strengthening and Functional Return (Weeks 12-24)
- Goals : Improve strength, endurance, and full functional range of motion (within RSA limits).
- Motion : Progress to full AROM for all planes. Stretching to improve motion where limited.
-
Strengthening
:
- Progressive Resistance Exercises : Increase resistance for deltoid strengthening (e.g., resistance bands, light weights).
- Rotator Cuff : Continue strengthening for internal and external rotators, if tuberosities have healed well.
- Scapular Muscles : Continue strengthening exercises for periscapular stabilizers.
- Activities : Gradually increase the weight of objects lifted. Begin activities that require the arm at shoulder height. Return to light recreational activities (e.g., swimming, golf, depending on patient goals).
- Important Note : Active external rotation will be limited if the greater tuberosity fails to unite, requiring patient education regarding compensatory strategies.
Phase 4: Advanced Strengthening & Return to Activity (Months 4-6 onwards)
- Goals : Maximize strength, power, and endurance. Return to higher-level functional and recreational activities.
- Strengthening : Continue with progressive resistance training, incorporating exercises specific to the patient's desired activities.
- Functional Training : Sport-specific or work-specific training as appropriate.
- Lifetime Restrictions : Patients should generally avoid overhead heavy lifting, repetitive forceful activities, and contact sports to minimize stress on the prosthesis and reduce the risk of late complications.
Clinical Pearls
:
* Radiographic assessment of tuberosity healing should be performed regularly. If nonunion occurs, especially of the greater tuberosity, expect permanent limitations in active external rotation.
* Neurological status, particularly axillary nerve function, must be monitored throughout rehabilitation.
* Communication between the surgeon, patient, and physical therapist is vital for a successful outcome.
Summary of Key Literature / Guidelines
The role of reverse shoulder arthroplasty in the management of proximal humeral fractures has been solidified through an accumulating body of literature demonstrating its efficacy, particularly in specific patient populations and fracture patterns.
- Superiority over Hemiarthroplasty : Multiple systematic reviews and meta-analyses have consistently shown RSA to provide superior functional outcomes and pain relief compared to hemiarthroplasty for displaced 3- and 4-part PHFs in elderly patients. Studies by Galli et al. (2018) and others highlight lower reoperation rates and better patient-reported outcome measures (PROMs) with RSA. The unpredictable nature of tuberosity healing, which is critical for hemiarthroplasty success, is largely mitigated by RSA's design.
- Comparison with ORIF : For complex PHFs in osteoporotic elderly patients, RSA often outperforms ORIF. Literature suggests that while ORIF can provide good outcomes in younger patients with good bone quality, it is fraught with high complication and failure rates (up to 30-40%) in the elderly, leading to revision surgeries. RSA offers a more predictable "single-stage" solution for this challenging cohort, especially when tuberosity comminution or pre-existing rotator cuff deficiency is present.
- Expanding Indications : Initially reserved for the most complex 4-part fractures, the indications for RSA in PHF have expanded. Current trends suggest RSA is increasingly considered for certain displaced 3-part fractures, and even select 2-part surgical neck fractures in the elderly with poor bone stock or high risk of ORIF failure. This shift is driven by the desire for more reliable outcomes in an aging, often osteoporotic, population.
- Importance of Tuberosity Repair : While RSA inherently compensates for rotator cuff deficiency, numerous studies (e.g., Cuff et al., 2008; Schnetzke et al., 2017) emphasize that stable fixation and union of the tuberosities in RSA-PHF cases significantly improve active external rotation, enhance overall function, and may contribute to a more aesthetically pleasing contour. Nonunion rates remain high, necessitating improved fixation techniques and potentially biological augmentation.
- Complication Profile : While effective, RSA is associated with a distinct set of complications. Scapular notching, though reduced with newer implant designs (e.g., lateralized glenospheres, eccentric glenospheres), remains a consideration. Axillary nerve palsy, periprosthetic infection, and glenoid loosening are critical concerns, and their incidence rates are well-documented. Long-term follow-up studies (e.g., Simovitch et al., 2017) are crucial for understanding implant survivorship and potential late failures.
- Patient Selection : Guidelines from organizations such as the American Academy of Orthopaedic Surgeons (AAOS) and various international trauma groups emphasize that careful patient selection is paramount. Factors such as patient age, functional demands, bone quality, presence of rotator cuff pathology, and fracture pattern should all be weighed when deciding on RSA. Patients with high functional demands or those who are very young are generally not primary candidates for RSA for PHF.
- Emerging Trends : Current research focuses on improving tuberosity healing rates (e.g., biological augmentation with bone grafts, growth factors), optimizing glenoid and humeral component designs to reduce complications like notching and improve range of motion, and refining surgical techniques for fracture reduction and fixation. Personalized surgical planning using 3D printing and navigation is also gaining traction.
- Outcomes : The consensus is that RSA provides reliable pain relief and improvement in activities of daily living for complex PHFs in the elderly. While a "normal" shoulder function is not typically achieved, the functional gains are significant, particularly in overhead activities where the deltoid is the primary driver. Patient-reported outcome measures (PROMs) like the Constant score, ASES score, and DASH score consistently show favorable results for RSA in this context.
In summary, the academic literature strongly supports RSA as a first-line treatment for complex, displaced proximal humeral fractures in elderly patients with compromised bone quality or pre-existing rotator cuff deficiency, offering predictable outcomes superior to hemiarthroplasty and often to ORIF in this specific cohort. Continued research and refinement of techniques aim to further improve outcomes and mitigate complications.
Clinical & Radiographic Imaging
You Might Also Like
