Patellofemoral Pain Syndrome (Runner's Knee): Epidemiology, Anatomy & Biomechanics

Key Takeaway
Patellofemoral Pain Syndrome (PFPS), or runner's knee, is anterior knee pain exacerbated by knee flexion activities, often without clear pathology. Its multifactorial etiology involves abnormal patellar tracking due to biomechanical factors like malalignment (e.g., increased Q-angle, trochlear dysplasia), muscle imbalances (VMO insufficiency, hip weakness), soft tissue tightness, and overuse/training errors.
Introduction & Epidemiology
Patellofemoral pain syndrome (PFPS), colloquially known as "runner's knee," represents a prevalent musculoskeletal disorder characterized by retropatellar or peripatellar pain exacerbated by activities involving knee flexion and extension, such as running, stair climbing, squatting, and prolonged sitting. It is a diagnosis of exclusion, typically without identifiable intra-articular pathology on conventional imaging. The term "runner's knee" is a broad descriptor for anterior knee pain in athletes, encompassing not only PFPS but also other conditions such as patellar tendinopathy, IT band friction syndrome, and saphenous nerve entrapment, though PFPS remains the most common etiology in this cohort.

Epidemiologically, PFPS affects individuals across various activity levels but exhibits a higher incidence in active populations, particularly adolescents and young adults engaged in sports. Its lifetime prevalence is estimated to be as high as 25-30% in the general population, with female athletes demonstrating a higher predisposition compared to males. Incidence rates in runners vary, often cited between 16% and 25%. Recurrence rates are substantial, with up to 70-90% of individuals experiencing persistent or recurrent symptoms years after initial diagnosis and treatment. The multifactorial etiology of PFPS, involving intricate interactions between biomechanical, anatomical, and training-related factors, complicates both its management and understanding.
Surgical Anatomy & Biomechanics
Understanding the intricate anatomy and biomechanics of the patellofemoral joint (PFJ) is paramount for diagnosing and managing PFPS. The PFJ comprises the patella, a sesamoid bone embedded within the quadriceps tendon, and the trochlear groove of the distal femur. Articulation occurs via the posterior surface of the patella and the anterior aspect of the femoral condyles.
Patellar Anatomy and Articulation
The patella's posterior surface is covered by hyaline cartilage, typically thicker than any other joint in the body, which articulates with the trochlear groove. This articulation begins around 20-30 degrees of knee flexion, with contact areas shifting superiorly and laterally with increasing flexion. The lateral facet of the patella is generally larger and more congruent with the lateral femoral condyle.
Extensor Mechanism
The extensor mechanism of the knee consists of the quadriceps femoris muscle, quadriceps tendon, patella, patellar ligament (patellar tendon), and tibial tubercle. This system functions as a lever to transmit forces from the quadriceps across the knee joint, facilitating efficient knee extension.
Static and Dynamic Stabilizers
Patellar tracking within the trochlear groove is influenced by both static and dynamic stabilizers.
*
Static Stabilizers:
*
Bony Anatomy:
The depth and congruence of the trochlear groove (trochlear morphology) and patellar shape are critical. A shallow trochlea or patella alta can predispose to instability and aberrant tracking.
*
Medial Patellofemoral Ligament (MPFL):
The primary static restraint against lateral patellar displacement, originating from the medial femoral epicondyle and inserting onto the superomedial patella.
*
Lateral Retinaculum:
While contributing to lateral stability, excessive tension can pull the patella laterally.
*
Medial Retinaculum:
A less distinct structure providing medial restraint.

-
Dynamic Stabilizers:
- Quadriceps Femoris: All four heads contribute, but the vastus medialis obliquus (VMO) is particularly important in controlling medial patellar tracking, especially in the terminal degrees of extension.
- Iliotibial Band (ITB): Can exert a lateralizing force on the patella, particularly if tight.
- Hip Musculature: Weakness in hip abductors (gluteus medius) and external rotators (gluteus maximus) can lead to increased femoral internal rotation and adduction during dynamic activities (valgus collapse), effectively increasing the Q-angle and lateralizing the patella.
- Foot and Ankle Mechanics: Pronation of the foot can lead to internal tibial rotation, which in turn can increase femoral internal rotation and alter patellar kinematics.
Biomechanics of PFPS
The underlying biomechanical pathology in PFPS is often attributed to abnormal patellar tracking, leading to increased stress on the patellofemoral joint cartilage and surrounding soft tissues. This can result from:
*
Malalignment:
*
Patella Alta/Baja:
High or low patellar positioning.
*
Increased Q-angle:
The angle formed by a line from the anterior superior iliac spine (ASIS) to the center of the patella and a line from the center of the patella to the tibial tubercle. An increased Q-angle (>15 degrees for males, >20 degrees for females) is associated with lateralizing forces.
*
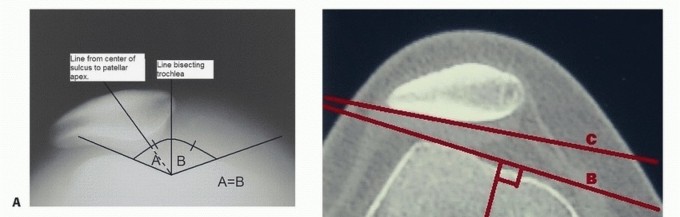
Trochlear Dysplasia:
An abnormally shallow or flat trochlear groove.
*
Tibial Torsion/Femoral Anteversion:
Rotational malalignment of the tibia or femur.
*
Muscle Imbalance/Weakness:
*
VMO Insufficiency:
Relative weakness or delayed activation of the VMO compared to the vastus lateralis (VL), leading to lateral patellar pull.
*
Hip Abductor/External Rotator Weakness:
Contributes to dynamic knee valgus and increased femoral internal rotation during weight-bearing activities.
*
Soft Tissue Tightness:
*
Tight Lateral Retinaculum:
Increases lateral compressive forces.
*
Tight ITB:
Pulls the patella laterally.
*
Tight Hamstrings/Gastrocnemius:
Can alter limb mechanics and increase patellofemoral joint stress.
*
Overuse and Training Errors:
Rapid increase in training volume, intensity, or duration, or running on cambered surfaces, can overload the PFJ.
The pain generated in PFPS is believed to stem from several sources:
*
Subchondral Bone Stress:
Repetitive loading on areas of cartilage, leading to increased pressure on the underlying bone.
*
Synovial Inflammation:
Irritation of the synovium lining the joint.
*
Retinacular Nociceptors:
Increased stress on the richly innervated retinacular tissues.
*
Fat Pad Impingement:
Hoffa's fat pad can become inflamed and impinged.
Indications & Contraindications
The management of PFPS is overwhelmingly non-operative, with surgical intervention typically reserved for a small subset of patients who fail comprehensive conservative treatment and have identifiable, addressable underlying structural pathologies contributing to their symptoms. The decision for surgery is complex, requiring a thorough evaluation of patient-specific factors, imaging findings, and careful consideration of the risk-benefit profile.
Indications for Operative Intervention (for associated pathologies)
- Recalcitrant Patellofemoral Pain Syndrome: Persistent, debilitating anterior knee pain despite a minimum of 6-12 months of high-quality, supervised physical therapy addressing strength, flexibility, biomechanics, and activity modification.
- Recurrent Patellar Instability: Clear episodes of patellar subluxation or dislocation, often associated with identifiable risk factors such as trochlear dysplasia, patella alta, increased tibial tubercle-trochlear groove (TT-TG) distance, or MPFL insufficiency. While instability is a distinct diagnosis, it frequently presents with symptoms mimicking or directly causing PFPS.
- Focal Chondral Lesions: Symptomatic, localized chondral defects within the patellofemoral joint, especially those greater than ICSS grade II or III, that are not responding to conservative measures.
- Osseous Malalignment: Significant structural abnormalities such as severe trochlear dysplasia, excessive TT-TG distance (>20 mm), or significant genu valgum/varum that fundamentally alter patellofemoral mechanics and are unresponsive to non-surgical means.
- Plica Syndrome (Symptomatic): A distinct, symptomatic medial plica that is thickened and inflamed, reliably reproducible on examination, and has failed conservative treatment (e.g., injections, physical therapy). This is a less common indication and often managed arthroscopically.
- Lateral Retinacular Tightness (Symptomatic and Isolated): Rarely, isolated and severe lateral retinacular tightness documented by physical examination (positive apprehension test, excessive lateral pull on patella) and dynamic imaging, without other significant contributing factors. Lateral retinacular release is increasingly scrutinized and less commonly performed in isolation due to potential iatrogenic medial instability.
Contraindications for Operative Intervention
- Absence of Identifiable Structural Pathology: The most significant contraindication. If clinical examination, advanced imaging (MRI, CT for alignment), and dynamic studies do not reveal a correctable anatomical or structural abnormality contributing to the PFPS symptoms, surgery is unlikely to be beneficial and carries inherent risks.
- Unsuccessful or Incomplete Conservative Management: Patients must demonstrate adherence to and failure of an extensive, structured conservative treatment program. Premature surgical intervention without adequate conservative trials often leads to poor outcomes.
- Poor Patient Compliance/Expectations: Patients unable or unwilling to adhere to post-operative rehabilitation protocols, or those with unrealistic expectations regarding surgical outcomes, are poor candidates.
- Active Infection: Absolute contraindication for any elective orthopedic surgery.
- Severe Osteoarthritis (OA): While some PFPS patients may develop OA, widespread, severe, or tricompartmental knee OA typically warrants broader arthroplasty considerations rather than isolated PFJ procedures.
- Complex Regional Pain Syndrome (CRPS): Undiagnosed or unmanaged CRPS is a contraindication, as surgery can exacerbate symptoms.
- Systemic Inflammatory Arthropathy (uncontrolled): Uncontrolled inflammatory conditions affecting the knee joint should be managed medically prior to considering surgery.
- Psychological Factors: Unaddressed psychosocial factors, somatization, or significant psychiatric comorbidities can negatively impact surgical outcomes.
Summary of Operative vs. Non-Operative Indications
| Indication Type | Description | Management Strategy |
| Feature | Non-Operative Approach |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
| Operative (Indications) | Failed extensive, compliant non-operative treatment AND presence of identifiable, correctable structural pathology contributing to anterior knee pain/instability. Examples: recurrent patellar instability, significant trochlear dysplasia, excessive TT-TG, MPFL insufficiency, severe patella alta/baja, focal symptomatic chondral lesions, symptomatic plica syndrome. | Patellofemoral realignment (e.g., Tibial Tubercle Osteotomy, MPFL reconstruction), trochleoplasty, arthroscopic debridement/chondroplasty, microfracture, OATS procedure, lateral retinacular release (rarely primary). |

Figure: A conceptual model for the decision-making process in PFPS management, emphasizing the role of failed conservative treatment prior to surgical consideration.
Pre-Operative Planning & Patient Positioning
Once operative intervention is deemed necessary based on the criteria for underlying pathologies, meticulous pre-operative planning is essential to ensure a successful outcome and minimize complications.
Pre-Operative Planning
-
Comprehensive Patient Evaluation:
- Detailed History: Reconfirm symptoms, previous conservative treatments, functional limitations, episodes of instability, and patient expectations.
- Physical Examination: Reassess patellar tracking, Q-angle, patellar tilt, apprehension test (if instability is a concern), quadriceps tone, VMO bulk, hip strength (abductors, external rotators), foot arch mechanics, and general lower limb alignment.
-
Radiographic Assessment:
- Standard Radiographs: AP, lateral (weight-bearing), merchant/sunrise views to evaluate patellar height (Insall-Salvati, Caton-Deschamps ratios), patellar tilt, trochlear morphology, and joint space.
- MRI: Essential for assessing cartilage status, meniscal and ligamentous integrity, bone marrow edema, Hoffa's fat pad, plica pathology, and MPFL integrity.
- CT Scan (with rotational profile): Crucial for evaluating osseous alignment, including TT-TG distance, femoral version, and tibial torsion, particularly when realignment osteotomies are contemplated. Dynamic CT or MRI may be considered in select cases to assess patellar tracking throughout the range of motion.
- Procedure Selection: Based on the identified pathology, select the most appropriate surgical intervention (e.g., MPFL reconstruction, tibial tubercle osteotomy, trochleoplasty, chondral repair). For multi-planar deformities, a combination of procedures may be necessary.
- Implant Selection and Sizing: Pre-operative templating based on imaging (especially for osteotomies) to determine appropriate hardware (screws, plates) and graft material (for MPFL reconstruction, e.g., semitendinosus autograft/allograft).
- Informed Consent: Thorough discussion with the patient regarding the chosen procedure, expected outcomes, potential complications (infection, stiffness, pain, non-union, iatrogenic instability), and rehabilitation timeline.
- Anesthesia Consultation: Standard pre-anesthetic workup. Regional anesthesia (femoral nerve block, adductor canal block) may be considered for post-operative pain management.
Patient Positioning
The specific positioning depends on the planned surgical procedure. However, for most patellofemoral interventions, the following principles apply:
*
Supine Position:
Standard for all anterior knee approaches.
*
Tourniquet Application:
A pneumatic tourniquet is typically applied to the proximal thigh, providing a bloodless field, which is critical for precision.
*
Leg Holder:
A lateral leg holder or bolster under the contralateral hip may be used to allow for unrestricted knee flexion and extension intra-operatively. Some surgeons prefer to allow the leg to hang free off the edge of the table to achieve full flexion.
*
Preparation and Drape:
Standard sterile preparation and draping from the thigh to the foot. The ipsilateral hip is often included in the sterile field if autograft harvest (e.g., gracilis/semitendinosus) is anticipated.

Figure: Standard supine positioning with a tourniquet applied for anterior knee surgery.
Detailed Surgical Approach / Technique
The "surgical approach" for PFPS is not a single, direct procedure for the syndrome itself, but rather a spectrum of operations targeting specific underlying anatomical or biomechanical pathologies that contribute to recalcitrant anterior knee pain or instability. Below, we detail common procedures.
1. Diagnostic Arthroscopy (Often Initial Step)
- Purpose: To confirm or rule out intra-articular pathologies such as meniscal tears, loose bodies, plica syndrome, and chondral lesions, and to assess patellar tracking dynamically.
-
Technique:
- Portals: Standard anteromedial and anterolateral portals. A suprapatellar portal may be used for a comprehensive view of the patellofemoral joint.
-
Assessment:
- Patellofemoral Joint: Evaluate the patellar and trochlear cartilage surfaces for softening (chondromalacia), fissuring, or full-thickness defects. Assess patellar tracking by gently manipulating the patella through a range of motion. Observe the central portion of the trochlea and patella.
- Plica Assessment: Identify and probe the medial plica. A symptomatic plica will appear thickened, inflamed, and may show evidence of chondral wear on the medial femoral condyle.
- Other Compartments: Systematically evaluate the tibiofemoral joint (menisci, articular cartilage, cruciate ligaments).
-
Intervention (if indicated):
- Chondroplasty: Debridement of unstable chondral flaps.
- Plica Resection: Excision of a symptomatic medial plica.
- Loose Body Removal: Excision of osteochondral fragments.
2. Medial Patellofemoral Ligament (MPFL) Reconstruction (for patellar instability with PFPS)
- Indications: Recurrent patellar dislocations or significant subluxations, often with associated PFPS, due to MPFL insufficiency.
- Graft Choice: Autograft (semitendinosus, gracilis) or allograft (hamstring, tibialis anterior). Autograft is preferred in younger, active patients.
-
Technique (Semitendinosus Autograft):
- Graft Harvest: A small (~2-3 cm) longitudinal incision is made over the pes anserinus insertion. The semitendinosus tendon is identified and harvested using a tendon stripper. The graft is prepared, typically folded to create a double-stranded graft, and whipstitched at the ends.
-
Femoral Tunnel Creation:
- Localization: The femoral attachment of the MPFL is crucial, typically located between the adductor tubercle and the medial epicondyle, proximal to the posterior femoral physis (if open). It's approximately 1 cm proximal and posterior to the medial femoral epicondyle. Intra-operative fluoroscopy or anatomical landmarks (medial epicondyle, adductor tubercle) are used.
- Drilling: A guide pin is inserted, and a tunnel (typically 4.5-6 mm) is drilled, avoiding violation of the femoral articular cartilage. The tunnel should be bicortical or short cortical, depending on fixation.
-
Patellar Fixation:
- Patellar Tunnels: Two bone tunnels are drilled through the superomedial quadrant of the patella. Alternatively, a single transosseous tunnel or patellar anchors can be used. Tunnels are typically placed at 1 o'clock and 11 o'clock positions for the right patella, approximately 1.5-2 cm apart, converging slightly towards the posterior cortex.
- Graft Passage: The graft is passed through the patellar tunnels from anterior-to-posterior, emerging on the medial side of the patella.
-
Graft Tensioning and Fixation:
- Tracking: The knee is brought to 30 degrees of flexion, the ideal point for MPFL tensioning, allowing the patella to track centrally. A varus force may be applied to the tibia to slightly reduce the patella, ensuring appropriate tension.
- Fixation: The femoral end of the graft is secured with an interference screw, suture button, or staple, ensuring appropriate isometric tension without over-constraining the patella. Over-tensioning can lead to medial patellar tilt, increased medial PFJ pressure, and pain.
- Final Assessment: Patellar tracking is re-assessed through full range of motion. There should be no medial patellar tilt or restriction of lateral patellar glide (typically 2 quadrants).

Figure: Illustration of MPFL reconstruction technique with patellar tunnels and femoral fixation.
3. Tibial Tubercle Osteotomy (TTO) (for excessive TT-TG or patella alta)
- Indications: Excessive TT-TG distance (>20mm), patella alta, or lateral patellar maltracking causing symptomatic PFPS or instability. A combination of procedures (e.g., TTO + MPFL) may be indicated.
-
Technique:
- Incision: A longitudinal incision is made along the anterior aspect of the tibia, typically slightly lateral to the midline.
- Exposure: The periosteum over the tibial tubercle is incised and elevated. The patellar ligament insertion is carefully protected.
-
Osteotomy:
- Distal Osteotomy: A distal oblique cut is made approximately 4-6 cm distal to the tibial tubercle.
- Proximal Osteotomy: A proximal oblique or transverse cut is made just inferior to the patellar ligament insertion.
- Medial Osteotomy: A medial longitudinal cut is made, creating a bone block of the tibial tubercle. The lateral cortex is carefully preserved as a hinge to prevent comminution and provide stability.
-
Translation:
- Medialization: The tubercle fragment is translated medially to reduce the TT-TG distance. The exact amount is determined pre-operatively from CT scans.
- Distalization (Maquet/Elmslie-Trillat type): If patella alta is present, the fragment can be distalized by resecting a small wedge of bone from the distal aspect of the osteotomy site.
- Anteriorization (Fulkerson type): If chondral lesions are present on the patella, anteriorization can offload the lesion, though this is less common for isolated PFPS without significant chondral defects.
- Fixation: The osteotomized fragment is typically secured with two or three cortical screws, ensuring stable fixation.
- Closure: Layered closure with careful attention to periosteum and soft tissues.

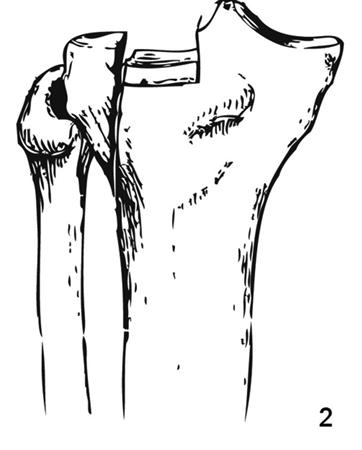
Figure: Diagram illustrating the principles of tibial tubercle osteotomy, including medialization and anteriorization.
4. Trochleoplasty (for severe trochlear dysplasia)
- Indications: Severe trochlear dysplasia (Dejour type B, C, D) causing recurrent patellar instability and potentially contributing to PFPS, particularly in young patients with good patellar cartilage.
-
Technique (Deepening Trochleoplasty):
- Incision & Exposure: A medial parapatellar incision provides access to the trochlear groove. The quadriceps tendon and patella are retracted laterally. The synovium over the trochlea is incised.
- Cartilage Elevation: The articular cartilage of the trochlea is carefully elevated as a single osteochondral flap, often with a thin layer of subchondral bone, using an osteotome or thin chisels. This requires precision to avoid fracturing the cartilage.
- Bone Resection: A small wedge or trough of subchondral bone is resected from the central portion of the trochlea, effectively deepening the trochlear groove.
- Cartilage Redraping: The elevated cartilage flap is then seated back into the newly deepened groove and fixed with absorbable sutures or temporary pins, allowing the cartilage to heal in its new, more congruent position.
- Variations: Other techniques exist, such as recession trochleoplasty, which involves removing bone from the entire trochlea, or sulcus-deepening trochleoplasty.
- Combined Procedures: Trochleoplasty is often combined with MPFL reconstruction and/or TTO to address all components of patellofemoral instability.
5. Chondral Repair/Restoration (for focal chondral lesions)
- Indications: Symptomatic, focal patellar or trochlear chondral defects (typically grade III-IV), often identified during diagnostic arthroscopy, especially after conservative treatment failure.
-
Techniques:
- Chondroplasty/Debridement: Arthroscopic smoothing and removal of unstable cartilage flaps. Primarily for pain relief, not true repair.
- Microfracture: Creation of small holes in the subchondral bone to stimulate bone marrow stem cells to form fibrocartilage. Best for smaller lesions (<2-3 cm²) in younger patients.
- Osteochondral Autograft Transfer System (OATS/Mosaicplasty): Transplantation of cylindrical osteochondral plugs from a less weight-bearing area (e.g., intercondylar notch) to the defect site.
- Autologous Chondrocyte Implantation (ACI)/Matrix-Induced Autologous Chondrocyte Implantation (MACI): A two-stage procedure involving biopsy of articular cartilage, culturing of chondrocytes, and then implanting them into the defect under a periosteal flap (ACI) or scaffold (MACI).
- Autologous Matrix-Induced Chondrogenesis (AMIC): Combines microfracture with a scaffold to enhance repair tissue quality.
- Approach: Typically arthroscopic, but larger or more complex defects may require mini-open arthrotomy.

Figure: Diagram illustrating an osteochondral autograft transfer procedure (OATS).
6. Lateral Retinacular Release (Limited Indications)
- Indications: Extremely rare as an isolated procedure for PFPS. May be considered only in cases of documented, severe, and isolated lateral retinacular tightness causing excessive lateral patellar tilt and compression, often confirmed by dynamic imaging and unresponsive to aggressive non-operative treatment. It is almost never indicated in the presence of patellar instability, as it can exacerbate lateral instability.
-
Technique:
- Arthroscopic or Open: Typically performed arthroscopically through a lateral portal.
- Release: The lateral retinaculum is sharply incised from the superolateral aspect of the patella distally, ensuring that only the fibrous retinaculum is released and not the vastus lateralis obliquus, which could lead to quadriceps weakness. The goal is to allow for medialization of the patella and reduction of lateral pressure.
- Controversy: The procedure is highly controversial due to high failure rates, potential for iatrogenic medial instability, and often addresses only a symptom rather than the root cause of maltracking.

Figure: Arthroscopic view showing instruments for a lateral retinacular release.
Complications & Management
Surgical interventions for patellofemoral pathologies, while often necessary for specific indications, are not without risks. Complications can range from minor to debilitating and require prompt recognition and appropriate management.
Common Complications and Management Strategies
| Complication | Incidence | Salvage Strategies / Management |
| Failure to meet the indicated endpoints for a candidate for surgical intervention, e. particularly after adequate conservative care, can lead to persistent symptoms or a worsening condition. Conversely, operating without proper underlying pathology justification or patient non-compliance to rehabilitation may yield complications without tangible improvement. | |
|
Primary
|
Runner's Knee (PFPS)
| Pain localized to retropatellar region, exacerbated by repetitive knee flexion/extension. Symptoms present for > 6-12 months despite adequate conservative treatment. No identifiable structural pathology amenable to direct surgical repair. | Persistent pain despite aggressive non-operative treatment, including activity modification, physical therapy (addressing hip abductor/ER strength, core stability, VMO strengthening, gluteal activation), bracing/taping, modalities, NSAIDs, and injections. |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
| Management Strategy |
| If a patient meets the criteria for underlying instability or painful structural lesions: |
|
Recurrent Patellar Instability
| Multiple episodes of patellar subluxation/dislocation. Positive apprehension test. Associated findings: trochlear dysplasia, patella alta, increased TT-TG, MPFL rupture. | MPFL reconstruction, Tibial Tubercle Osteotomy (TTO) (medialization/distalization), trochleoplasty, or combined procedures. |
|
Symptomatic Focal Chondral Lesions
| Persistent pain, locking, or catching localized to a specific chondral defect (>Grade II-III) in the patellofemoral joint, failed conservative management. | Arthroscopic chondroplasty, microfracture, OATS procedure, ACI/MACI, AMIC. | |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
| |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
| It's crucial for orthopedic surgeons to remember that direct surgical intervention for PFPS itself is rare. Instead, surgery is reserved for identifiable and often co-occurring structural pathologies (e.g., instability, severe malalignment, symptomatic chondral lesions) that contribute to the PFPS symptoms and have failed exhaustive conservative management. The surgical approaches described above address these underlying issues, not PFPS directly. |
| | |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
|
Symptomatic Plica Syndrome
| A distinct, thickened medial plica, reproducibly tender and producing symptoms with knee motion, resistant to conservative treatment. |
| |
| |
| |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. | |
| |
| |
| |
| |
| Non-operative (PFPS) | Chronic anterior knee pain, exacerbated by activity, often multifactorial in nature. |
| Non-operative (PFPS) | Persistent, diffuse anterior knee pain, exacerbated by activity, in the absence of obvious mechanical symptoms or identifiable structural pathology. |
| Non-operative (PFPS) | Persistent, diffuse anterior knee pain, exacerbated by activity, in the absence of obvious mechanical symptoms or identifiable structural pathology. |
| |
| |
| | | |
| |
| |
| |
| |
|
Clinical & Radiographic Imaging










You Might Also Like